jmmodernpublishers.ijmaes.org


Beriman Rahmansyah1, Lucky Anggiat2
Corresponding Author:
Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
Email : beriman.rahmansyah@uki.ac.id
Author:
Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
| ABSTRACT |
Background: In applying the physiotherapy interventions, physiotherapists frequently use electro physical agent (EPA) which is therapeutic modalities that have indeed become one of the popular therapies besides exercise therapy and manual therapy. This study aimed to identify the availability and usage of EPA by physiotherapists in East Jakarta, Indonesia.
Methods: This study used online survey research method. The target population was physiotherapists in East Jakarta who joined in the WhatsApp group of the Indonesian Physiotherapy Association, East Jakarta Branch. From 189 target respondents, only 73 respondents were willing to fill out the questionnaires given by the researchers.
Results:In the view from the availability of EPA modalities, most respondents or 91.8% answered the availability of electrical stimulation. It is followed by ultrasound therapy (84.9%). The least EPA modalities found in the respondent’s workplace were paraffin bath (23.3%). From the results, the use of EPA modalities in the form of ultrasound therapy and electrical stimulation was the most widely used. Subsequently, as many as 49.3% of respondents used the ultrasound therapy modality every day. A total of 45.2% of respondents used electrical stimulation modality.
Conclusion. The EPA modalities are quite widely available among physiotherapists in East Jakarta, Indonesia. The most widely available modalities are electrical stimulation, ultrasound therapy, and infrared radiation and in addition to the diathermy modality, which is also quite widely available. The availability of EPA tools is also in line with the frequency of use dominated by ultrasound therapy, electrical stimulation, and Microwave Diathermy.
Keywords: Electro Physical Agents; Modality, Intervention; Physiotherapy
| Received on 4thFebruary 2022, Revised on 19thFebruary 2022, Accepted on 26thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.008 |
INTRODUCTION
In clinical practice, physiotherapists carried out all physiotherapy processes from examination, planning, physiotherapy interventions and evaluations, to developing, maintaining, and restoring body movement and function1. Physiotherapists can provide interventions to patients with various options, such as manual therapy, therapeutic exercise, and interventions with physical equipment as well as electrophysical and mechanical modalities2. In applying the physiotherapy interventions, physiotherapists frequently use electro physical agent (EPA) which is therapeutic modalities that have indeed become one of the popular therapies besides exercise therapy and manual therapy3.
Electrophysical agent is defined as the use of physiotherapy modalities for evaluation, treatment, prevention of activity disturbances, and participation restrictions. With EPA, physiotherapist can help establish a physiotherapy diagnostic and evaluate treatment outcomes4. Furthermore, EPAis an important component of physiotherapy and consists of the application of various forms of EPA for therapeutic purposes3. Electro physical agents modalities are generally categorized as thermal (hot and cold), electromagnetic (diathermy, ultraviolet, and infrared light), or mechanical (traction and compression)5,6. Electro physical agents is very widely used in physiotherapy interventions because it has become a standard in hospitals, such as Micro Wave Diathermy (MWD), Short Wave Diathermy (SWD), Infra-Red Radiation, and Laser Therapy and Ultrasound therapy (US)7. There are also electrical stimulations such as Transcutaneous Electrical Nerve Stimulation (TENS), Interferential Therapy (IFT), and Neuromuscular Electrical Stimulation (NMES). However, there are also types of non-thermal applications, namely variations in the use of Pulsed MWD, Pulsed SWD, Pulsed Laser Therapy, and Pulsed Ultrasound therapy. However, scientific results related to the frequency of using EPA device are still rare8,9.
There are not many studies on the use of EPA in Indonesia. Therefore, the development of EPA in Indonesia is not known4,8. From that background, this study is needed to be able to identify the use of EPA by physiotherapists. However, this study is a preliminary study in the East Jakarta area because it is close to the researchers’ university (Universitas Kristen Indonesia) and there are quite a number of representative hospitals. In addition, it is suggested that future studies are conducted more comprehensively. This study also aims to see the availability of EPA modalities used by physiotherapists so that they can be used as a reference in teaching and learning EPA at universities.
METHODOLOGY
This study used online survey research method. The target population were physiotherapists in East Jakarta who joined in the WhatsApp group of the Indonesian Physiotherapy Association, East Jakarta Branch with 189 respondents. The questionnaires were distributed to all respondents. However, only 73 physiotherapists were willing to fill them out. The data were collected using survey questionnaires to obtain responses from the respondents. The questionnaire consisted of 14 questions. The questions in the questionnaire were divided into several parts, firstly profile part which includes the identity of the physiotherapist and their education level. However, the respondent’s detailed identity was not displayed to maintain the respondent’s privacy. Subsequently, the second part was related to the physiotherapist’s work experience, namely the length of years of work, the number of patients treated in one day, and the condition of the patients often encountered. After that is the last part related to the availability and frequency of using EPA modalities. Before distributing the questionnaires, the questionnaires were tested by physiotherapists and made improvements if needed. The questionnaires were distributed within 3 months, namely December 2021 to February 2022. After the distribution was the processing of the survey results from the questionnaires. At the end, the results were reported and discussed.
RESULTS AND DISCUSSION
From 189 target respondents, only 73 respondents were willing to fill out the questionnaires given by the researchers. The physiotherapist’s identity is in the following table of respondent profiles.
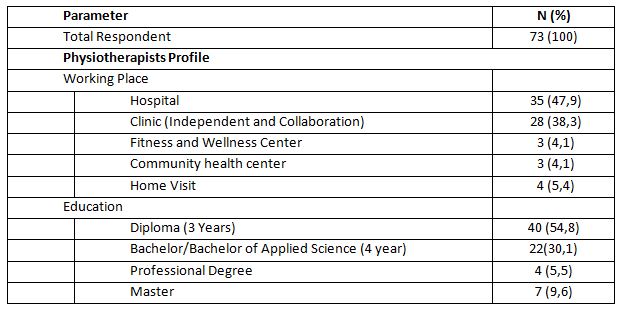
It can be seen that of 73 physiotherapists as respondents in this survey, 35 people or around 47.9% worked in hospitals and only 4 people or around 4.1% worked in community health centers. The previous study also stated that in a hospital, there were more than 10 physiotherapists8. The workplace of physiotherapists in some countries is also dominated by hospitals and clinics10,11. In terms of education level of the respondents, as many as 40 respondents or around 54.8% had a diploma which is three-year study in university level.
There were 7 people or around 9.6% who had a master’s degree. In Indonesia, those who are given the authority to practice physiotherapy are physiotherapists starting at the diploma level to the professional level2. This is already in line with the provisions of the World Physiotherapy Organization, although there is still a national government that gives authority to physiotherapists at the diploma level1. Thus, physiotherapists in East Jakarta are considered to meet the minimum qualifications to practice physiotherapy. Likewise, in some countries, it is found that the qualifications for physiotherapy education are quite varied and still follow the national regulations of each country10,11.
The following result of the questionnaire is about the physiotherapists’ work experience which describes the range of work of physiotherapists, the average number of patients treated in one day, and the condition of patients treated by the physiotherapists. The data are presented in the following Table 2.
The following result of the questionnaire is about the physiotherapists’ work experience which describes the range of work of physiotherapists, the average number of patients treated in one day, and the condition of patients treated by the physiotherapists. The data are presented in the following Table 2.
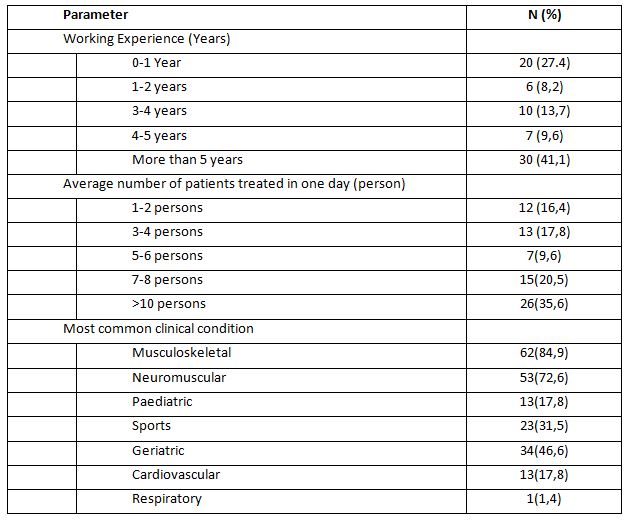
In the table, it can be seen that the majority of respondents who have worked for more than five years are 41.1%, which indicates that the physiotherapists have experienced in working and using EPAmodalities. Physiotherapists with more than five years of experience will indeed provide better patient satisfaction12.
As many as 35.6% physiotherapists treated more than ten patients daily and around 16.4% treat one to two patients every day. From these data, it can be seen that some physiotherapists still treat too many patients in one day, that is, more than ten patients daily. If there are more than 10 patients treated daily by the physiotherapist, assuming one patient is an hour, it indicated that the physiotherapist in providing services is not optimal, because in general, the number of daily working hours is only about 8 hours11–13. However, there are not many studies that support this. It can also cause harm to the physiotherapist who is likely to experience fatigue. Thus, the number of physiotherapists must be increased in order to provide optimal services14.
Most respondents or 84.9% treated patients with musculoskeletal condition and the least treated were patients with respiratory condition. Several studies also support this. As in a study by Jahan et al., (2021) who found that physiotherapists mostly treated musculoskeletal patients. Likewise, in a study in a hospital, physiotherapists generally dealt with various types of patients with musculoskeletal disorders8. In addition, a study in a certain region also stated that musculoskeletal cases were very dominant in the physiotherapy practice15.
The following result is related to the availability of EPA modalities as well as the frequency of use. Table 3 shows the available modalities in each physiotherapist’s workplace.
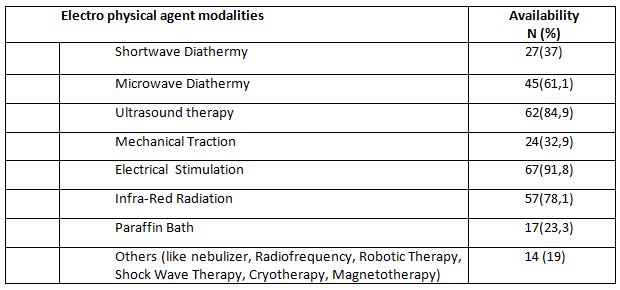
In the view from the availability of EPA modalities found in each respondent’s workplace, most respondents or 91.8% answered the availability of electrical stimulation. It is followed by EPA modalities in the form of ultrasound therapy (84.9%). The least EPA modalities found in the respondent’s workplace were paraffin bath (23.3%). The availability of diathermy modalities in the form of Micro Wave Diathermy at the respondents’ workplace had a considerablevalue of around 61.1%, including Short Wave Diathermy which had a considerable percentage (37%).
There are also heat therapy modalities that are quite popular among physiotherapists, namely Infrared Radiation device which was answered by 50% of the total respondents. A study in Australia also shows that ultrasound therapy is a modality that has considerable availability16. Furthermore, the use of EPA interventions is still a trend among physiotherapists in Asia4,17.
However, apart from Asia, in America there is also a trend in the use of EPA18. The most widely available modality tools are cold and hot agents, with electrical stimulation therapy and ultrasound therapy. It was also found that in America, there are very few diathermy modalities available.
From the results of this study, it can be seen that physiotherapists in East Jakarta have the availability of adequate EPA modalities in accordance with the needs of the patients. Nevertheless, the needs for EPA must really be acknowledged and the latest research developments should keep up with the effectiveness of existing EPA modalities(Belanger, 2015; Bellew et al., 2016;
Goh &Abe, 2015). There are also some EPA modalities in the table 3 that tend to be new and have very little availability.In addition, the existing modalities data can also be a reference for lecturers to continue to provide updates on the science of EPA modalities. By understanding the availability, the lecturer needs to provide understanding to physiotherapy students at the university in order to be more critical in the use of electrophysical instruments in clinical practice. Previous studies also used the survey results in the availability of physiotherapy modalities for teaching purposes at universities18.
The last results of this study were related to the frequency of the use of EPA. In this study, we only prepare the types of modalities that are popularly used by physiotherapists, which are SWD, MWD, US, IRR, Mechanical Traction, Electrical Stimulation, LASER, and paraffin bath. It is also based on the availability of such modalities at the physiotherapists’ place of practice. Moreover, we conducted a survey related to how many combinations of EPA modalities were used by physiotherapist for each patient with certain condition.
The time frame we chose was one week to make it easier for the physiotherapists to remember the modalities they used on average. Frequency classification was also made using the range: always (everyday), often (four to five times a week), rarely (one to three times a week), and none (not using the modality or the modality is not available). All usage and frequency data are shown in Table 4.
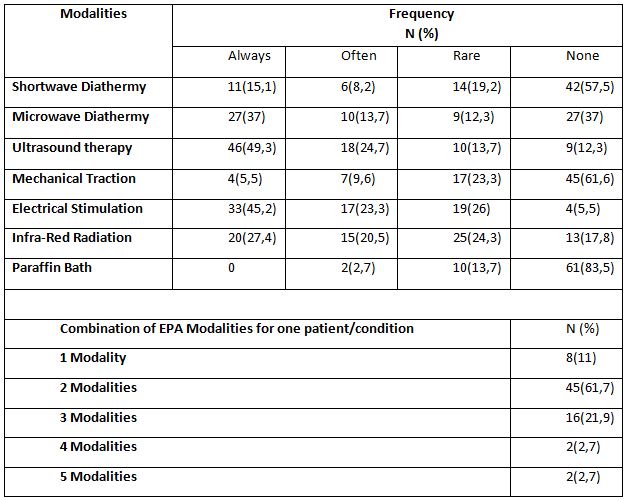
From the results above, it can be seen that the use of EPA modalities in the form of ultrasound therapy and electrical stimulation was the most widely used. Subsequently, as many as 49.3% of respondents used the ultrasound therapy modality every day and only 12.3% never used the ultrasound therapy modality. A total of 45.2% of respondents used electrical stimulation modality and only 5.5% never used it. The modalities of paraffin bath and mechanical traction were the least used EPA modalities. As many as 83.5% of respondents never used paraffin bath and 61.6% of respondents never used mechanical traction.
The use of electrical stimulation is believed to reduce neuromusculoskeletal disorders. As in the results of a previous study by Manik & Rahmansyah (2021), it mentioned that EPA modalities in the form of electrical stimulation can reduce pain in neuromuscular and musculoskeletal conditions20. In line with this, a study by Abe et.al (2016), which surveyed 1099 respondents from 170 hospitals/clinics showed that the use of electrical stimulation in the form of low frequency currents and ultrasound therapy ranked second and third below the modality in the form of hot pack4. Furthermore, a study by Greco et al. (2018) also found that the use of electrical stimulation was quite dominant, along with ultrasound therapy and thermal modality (cold or hot). In addition, we should take attention to the results of the existing research is that despite the availability of diathermy physiotherapy tools, it does not guarantee that they are often used. The trend that is developing in the world is that diathermy modality should be abandoned and replaced with more effective modality 9,18,19.
In this study, it was also found that physiotherapists used more than two modalities in one patient with one condition. This shows that physiotherapists very often used EPA modalities. The use of more than two modalities is possible if the patient’s condition requires intensive intervention and there are more than two symptoms in one condition19,21. Knowledge of the use of appropriate and effective interventions needs to be carried out in the future to be able to provide optimal services to the patients22,23.
This study is a very simple survey as a preliminary study. More complex analysis in the existing data can be done as a development of future research. Likewise, the survey in this study was only conducted in one city, so more detailed research using a larger population is needed as a development in the future. This study also has many limitations, one of which is the willingness of the physiotherapist to fill out the questionnaire. Therefore, it is possible to conduct more interesting research that can attract the attention of the physiotherapist to fill out the questionnaires in the future. The reasons for selecting interventions related to the condition of the patients have not been captured in this study, so further research development is needed.
CONCLUSION
The EPA modalities are quite widely available among physiotherapists in East Jakarta, Indonesia, both in health facilities and independent clinical practices. The most widely available modalities are electrical stimulation, ultrasound therapy, and infrared radiation and in addition to the diathermy modality, which is also quite widely available. The availability of EPAtools is also in line with the frequency of use dominated by ultrasound therapy, electrical stimulation, and Microwave Diathermy. Physiotherapists also quite often use EPA because in one patient with one condition, physiotherapists frequently use more than one modalities.
Recommendation: Physiotherapists in East Jakarta should pursue their education to a higher level to find out the latest developments in electrophysical interventions. The use of diathermy should also be reduced by its decreasing use abroad. The number of patients handled by one physiotherapist in one day is too many, so it is necessary to add the number of physiotherapists who work in a hospital. Based on the result, it also suggested that at universities, it is still necessary to provide scientific development in EPA, especially the frequent modalities like ultrasound therapytherapy, electrical stimulation, and diathermy so that when the students graduate, they can practice well.
Acknowledgement: The researcher would like to thank every physiotherapist who is willing to participate in this research. Furthermore, we also thank the of the Indonesian Physiotherapy Association, East Jakarta Branch, for allowing us to collect data from the organization members.
Conflict of interest: The author has no conflict of interest to declare.
Funding of study: This study was funded by Universitas Kristen Indonesia.
Compliance with Ethics: This research does not provide anything that is harmful to the respondents so that it does not use ethical research. However, this research was conducted with the permission of the university and the permissionfrom chairman of the Indonesian physiotherapy association, East Jakarta branch, with reference number 03/IFI-JAKTIM/XI/2021.
REFERENCES
1. World Confederation for Physical Therapy. Guideline for standards of physical therapy practice. Published online 2011:1-19. https://world.physio/sites/default/files/2020-07/G-2011-Standards-practice.pdf
2. Kementerian Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan No.80 Tahun 2013.; 2013.
3. Watson T. The role of electrotherapy in contemporary physiotherapy practice. Man Ther. 2000;5(3):132-141.
4. Abe Y, Goh AC, Miyoshi K. Availability, usage, and factors affecting usage of electrophysical agents by physical therapists: A regional cross-sectional survey. J Phys Ther Sci. 2016;28(11):3088-3094. doi:10.1589/jpts.28.3088
5. Starkey C. Therapeutic Modalities. Fourth Edi. (McDonald Q, ed.). F. A. Davis Company; 2013. www.fadavis.com
6. Belanger A-Y. Therapeutic Electrophysical Agents. Lippincott Williams & Wilkins; 2015.
7. Kementerian Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia Nomor 65 Tahun 2015 Tentang Standar Pelayanan Fisioterapi. Vol 16.; 2015.
8. Panjaitan LA. Penggunaan Terapi Elektrofisis Pada Satu Rumah Sakit Umum Swasta di Jakarta. J Fisioter. 2020;20(2):40-45.
9. Goh A-C, Abe Y. New directions in electrophysical agents : where do we go from here? Japanese J Electrophysical Agents VO – 22. 2015;(April):4.
10. Khairy WA, Bekhet AH, Sayed B, Elmetwally SE, Elsayed AM, Jahan AM. Prevalence, profile, and response to work-related musculoskeletal disorders among egyptian physiotherapists. Open Access Maced J Med Sci. 2019;7(10):1692-1699.
11. Nkhata L a, Zyaambo C, Nzala SH, Siziya S. Work-related Musculoskeletal Disorders : prevalence , contributing factors and coping strategies among Physiotherapy personnel in Lusaka , Kitwe and Ndola districts , Zambia. Physiotherapy. 2010; 37(4):262-267.
12. Jahan AM, Rwaiha AE, Gusaibat SR, Al-Ahwal NA, Al-Jafairi ZM, Al-Rashidi MA. Patient Satisfaction With Physiotherapy Services in Libya: A Cross-Sectional Study. J Patient Exp. 2021;8:1-7.
13. Hima Bindu P, Thiruppathi A. Work Related Musculoskeletal Discomfort (WRMSD) among Physiotherapists. Int J Physiother. 2014;1(4):200.
14. Manurung NSA, Sunaryo T, Gunawan I, Anggiat L. Analysis of the need for Physiotherapists in a private hospital in Indonesia using the workload indicator of staffing need referring to the implementation of the physiotherapy process as risk mitigation of services. Int J Med Exerc Sci. 2020;06(01):697-705.
15. Odumodu IJ, Olufunlayo TF, Ogunnowo BE, Kalu ME. Satisfaction With Services Among Attendees of Physiotherapy Outpatient Clinics in Tertiary Hospitals in Lagos State. J Patient Exp. 2020;7(4):468-478.
16. Chipchase LS, Williams MT, Robertson VJ. A national study of the availability and use of electrophysical agents by Australian physiotherapists. Physiother Theory Pract. 2009;25(4):279-296.
17. Shah SGS, Farrow A. Trends in the availability and usage of electrophysical agents in physiotherapy practices from 1990 to 2010: a review. Phys Ther Rev. 2012;17(4):207-226.
18. Greco JL, Lamberg EM, McKenna RF, Muratori LM. Trends in availability and usage of biophysical agents among physical therapists in the United States. Phys Ther Rev. 2018;23(2):116-123.
19. Bellew JW, Michlovitz SL, Nolan TP. MODALITIES For Therapeutic Intervention. F. A. Davis Company; 2016.
20. Manik JWH, Rahmansyah B. The effect of nerve mobilization on the median nerve in pain perception of electrical stimulation. Int J Med Exerc Sci |2021;7(3). 2021; 7 (August):1104-1112.
21. Kim MK, Ji SG, Cha HK, Chang JS. Effects of electromagnetic diathermy in conjunction with nerve mobilization in the management of lower back pain. J Phys Ther Sci. 2012;24(12):1337-1339.
22. Beales D, Mitchell T, Holthouse D. Stepped care for musculoskeletal pain is ineffective: A model for utilisation of specialist physiotherapists in primary healthcare management. Aust J Prim Health. 2021;27(6):431-436.
23. Tiktinsky R, Chen L, Narayan P. Electrotherapy: Yesterday, today and tomorrow. Haemophilia. 2010;16(SUPPL. 5):126-131.
| Citation: Beriman Rahmansyah, Lucky Anggiat. Availability and usage of electro physical agentmodality by Physiotherapist in East Jakarta, International Journal of Medical and Exercise Science, March 2022; 8(1); 1228-1237. |
Lisnaini
Corresponding Author:
Physiotherapy Program, Faculty of Vocational Studies, Universitas Kristen Indonesia, Jakarta
Mail id: lisnaini@uki.ac.id
| ABSTRACT |
Background: Diastasis Recti Abdominis (DRA) is a stretching and widening of the linea-alba which is a connective tissue that stretches in the middle of the abdomen that occurs in the second trimester to the third trimester and will continue until after delivery. Usually it cause complaints such as abdominal muscle weakness, lower back pain and posture disorders. Efforts that can be made to reduce the dilation of the postnatal linea-alba are by therapeutic exercise or physical exercise on the abdominal muscles. This study will focus on plank exercise was conducted to determine its effect on reducing the distance of the DRA below umbilicus.
Method: This research is a quantitative analysis with a quasi-experimental design that uses a two-group approach where the treatment was only given to one group and the other group only as a control.
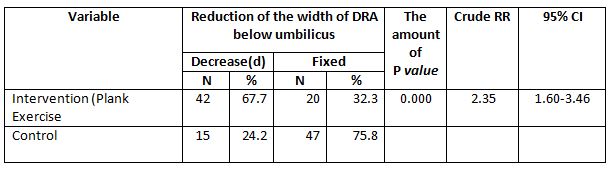
Result: There was a reduction in the width of the diastasis rectus abdominis below the umbilicus by (67.7%) or as many as 42 people who did plank exercise while in the control group only (75.8%) or as many as 47 people who experienced a reduction in the width of the DRA lower umbilicus.
Conclusion: There is an effect of plank exercise on changes in the distance of the DRA below umbilicus and there is a relationship between plank exercise and a reduction in the width of the DRA below umbilicus in postpartum women.
Keywords: Diastasis Recti Abdominis; Postpartum; Plank exercise; Physiotherapy
| Received on 4thFebruary 2022, Revised on 19thFebruary 2022, Accepted on 26thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.007 |
INTRODUCTION
Diastasis Recti Abdominis (DRA) is stretching and widening of the linea alba, which is the connective tissue that runs down the middle of the abdomen and connects major abdominal muscles such as external obliques, internal obliques, transversus abdominis, and rectus abdominis1. Some researcher also stated that this condition usually happens when entering the second trimester and will become clearer in the third trimester and will continue after childbirth (postpartum)2,3.
Diastasis Recti Abdominis will widen due to frequent pregnancies. It also occurs because during pregnancy there is an increase in body weight and an increase in the hormonal levels of relaxin, progesterone, and estrogen from the connective tissue which causes mechanical pressure on the abdominal wall by the growing fetus so that the connective tissue becomes soft and the linea alba becomes tenuous4.
Almost 100% of pregnant women experience DRA5,6. Approximately 50% of nulliparous women experienced DRA and in women who undergo abdominal surgery and in postmenopausal patients7.Factors causing DRA are found in women who do excessive abdominal exercises especially in the first trimester, women who like to use hormone therapy, women who perform repeated operations on their abdomen, women with multiple pregnancies, large babies, and caesarean sections8. Ambarwati and Candido also stated that age and multiparity can be risk factors for rectus abdominis diastasis in women9,10.
Several studies have stated that the general impacts of DRA are the weakness of the abdominal muscles, urinary incontinence, decreased elasticity of the abdominal wall, functional and cosmetic disorders, low back pain5,6,9. Furthermore, about 52% of patients with urogynecological disorders stated that they had DRA and about 66% had complaints of pelvic floor muscle weakness such as stress urinary incontinence, stool incontinence and/or pelvic organ prolapse7.
Efforts that can be made to reduce the dilation of the postnatal linea alba are by therapeutic exercise or physical exercise on the abdominal muscles4. Previous research by Gitta et al. (2016) which stated that static contraction exercises in the abdominal muscles have been shown to reduce the DRA distance11. Research by Acharry & Kutty (2015) also stated that to prevent and reduce the DRA, physical therapy can be carried out after childbirth12. Another research by Wijayanti, (2016) proved that abdominal circumference can be reduced by strengthening abdominal muscles, sit-ups, postpartum exercise, physiotherapy, and plank exercise13.
Plank exercise is a type of static contraction exercise that is isometric exercise, which is muscle contraction exercises against resistance without causing changes in muscle length and joint motion14. This exercise can activate neuro-adaptive and proprioceptor mechanisms through altered sensory input to muscles. Lee et al.,stated that muscle activity in plank exercise is related to posture and muscle position exercises and has been proven to strengthen core muscles (especially transverse abdominis)15.
Based on all previous evidences obtained that exercise and physical exercise of the abdominal muscles can prevent and reduce postnatal women’s problems such as reducing abdominal circumference and increasing abdominal muscle strength. This study willfocus on plank exercise was conducted to determine its effect on reducing the distance of the DRA below umbilicus.
METHODS
This research is a quantitative analysis with a quasi-experimental design that uses a two-group approach where the treatment was only given to one group and the other group only as a control16. Meanwhile, the research design used pre and post-test design and how to take samples using a purposive sampling method.This study aims to determine the effect of plank exercise on DRAin women postpartum. Before and after being given treatment, the sample was measured for the length of the uterus by palpation and using a measuring device,calipers. The number of postpartum women who participated in this study was 124 people and was divided equally into 62 people in each group.
This research was conducted in the working area of the Makassar District Health Center, East Jakarta, and was carried out from April 2019 to June 2019. Plank Exercise intervention is carried out 3 times a week for 6 weeks.
The criteria set for the research sample are as follows:
Inclusion criteria:
Exclusion Criteria:
Measurement of DRA:
Measurement by palpation of the fingers and calipers DRA measurements were carried out before and after plank exercise. According to Bursch, Mantle et al. and Rett et al. (2009), the palpation measurement technique meets the criteria of reliability and ease to use. The measurement can be done by placing a finger palpation between the medial border of the right and left rectus abdominis muscles, which is parallel to the linea alba3,17,18.
The size of DRA is determined by the number of fingers that enter between the two gaps in the abdominal wall that are the muscles above and below the umbilicus when the individual performs the movement placing her chin on her chest. Clinically, this palpation technique is simple.

1.Measurement procedure by palpation is carried out as follows:
2. Measurement using calipers
Measurement procedure the rectal distance was measured using a caliper technique, the participant was in a lying position with a pillow under the head and feet resting on the base and arms by the side of the body. The desired measurement location is marked 4.5 cm above the midpoint of the umbilicus and 4.5 cm below the midpoint of the umbilicus. Each participant raises their head until the spine of the scapula is off the table surface.
Participants were asked to maintain this position while the examiner palpated the medial border of the right & left abdominis abdominal muscles at the marked area. Measuring the inside of the jaws of a digital nylon caliper, positioned at the location of the palpated finger, perpendicular to the direction of the muscle and adjusted for the width of the perceived intra-rectal distance. Three measurements were taken for each assessment and then recorded. Participants are allowed to rest between measurements and are also allowed to rest if they feel tired 21.

Intervention Group
In the treatment group, interventions were given in the form of plank exercise.Plank exercise is an isometric type of exercise, which is a type of static muscle contraction exercise against resistance without any change in muscle length or not followed by joint movement14. This exercise begins by extending the legs while supporting the upper body with the arms. Bend elbow position, hold abdominal and gluteal muscles.
This exercise is done 3 times a week for 6 weeks with 3 repetitions of each exercise. The prone plank exercise is carried out by holding it for 30 seconds for each movement then resting for 15 seconds and then repeating it 20.

Control Group
In the control group, the research sample was given an education program in the form of counseling on the importance of exercise to restore the health of postpartum women with DRA conditions. Based on research, regular exercise can also improve the DRA4.
RESULTS AND DISCUSSION
Following is the distribution of Plank Exercisevariables and the control group

Based on table 1, each postpartum woman performs Plank Exercise that the intervention group also included 62 people (50%) and the control group with 62 people (50%).

Based on table 2, the number of postpartum women aged < 20 years or > 30 years was 59 people (47.6%), multiparous status was 59 people (47.6%), had Obesity/Overweight BMI which was 60 people (48.4%), history of singleton pregnancy namely 120 people (96.8%), and the weight of newborns was normal (not macrosomic) that was 112 people (90.3%).
Relationship between Independent and Confounding Variables on Reduction of the width of the DRA below umbilicus)
Table 3. shows that those who did plank exercise mostly reduced the width of the DRA below umbilicus was 42 people (67.7%).
While most of the postpartum women who do not do plank exercise did not experience a reduction in the width of the DRA below umbilicus (fixed) was 47 people (75.8%). Chi Square test results stated that there is a relationship between plank exercise with a reduction in the width of the DRA below umbilicus (p value <0.05).
Postpartum women who did Plank Exercise had a 2.3 times chance of experiencing a reduction in the width of the DRA below umbilicus compared to those who did not do it (p value =0.000; cRR=2.35;95%CI= 1.60-3.46).
Based on Table 4, the results of the cross-tabulation show that most of the postpartum women aged < 20 years or >30 years did not experience a reduction in the width of the DRA below umbilicus (fixed) was 31 people (52.5%). While those aged 20-30 years most did not experience a reduction in the width of the DRA below umbilicus (fixed) was 36 people (55.4%). Chi Square test results showed that there was no relationship between age and a reduction in the width of the DRA below umbilicus (p value> 0.05).
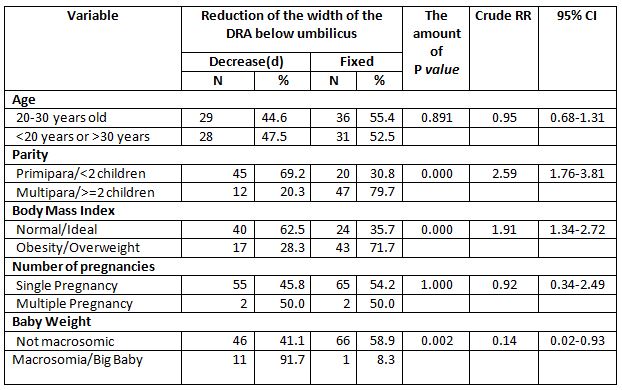
The results of cross tabulation showed that most of the postpartum women with multiparous status did not experience a reduction in the width of the DRA below umbilicus (fixed) was 47 people (79.7%). While most of the primipara experienced a reduction in the width of the DRA below umbilicus was 45 people (69.2%). Chi Square test results stated that there is a relationship between plank exercise with a reduction in the width of the DRA below umbilicus (p value <0.05). Primipara postpartum women were 2.6 times more likely to experience a reduction in the width of the DRA below umbilicus than multiparous women (p value =0.000; cRR=2.59;95%CI= 1.76-3.81).
The results of the cross tabulation showed that the postpartum women who were obese/overweight mostly did not experience a reduction in the width of the DRA below umbilicus (fixed) was 43 people (71.7%). Meanwhile, postpartum women with normal/ideal BMI experienced a reduction in the width of the DRA below umbilicus was 40 people (62.5%). Chi Square test results showed that there was a relationship between excess BMI and a reduction in the width of the DRA below umbilicus (p value <0.05). Postpartum women with normal/ideal BMI were 1.9 times more likely to experience a reduction in the width of the DRA below umbilicus compared to obesity/overweight (p value=0.000; cRR=1.91;95%CI=1.34-2.72).
The results of cross tabulation showed that postpartum women with multiple pregnancies 50% experienced a reduction in the width of the DRA below the umbilicus. While postpartum women with singleton pregnancies mostly did not experience a reduction in the width of the DRA below the umbilicus (fixed) was 65 people (54.2%). Fisher Exact test results showed that there was no relationship between multiple pregnancies with a reduction in the width of the DRA below umbilicus (p value> 0.05).
The results of cross tabulation showed that postpartum women who gave birth to babies weighing 4000 grams mostly experienced a reduction in the width of the DRA below the umbilicus was 11 people (91.7%). Meanwhile, postpartum women with babies weighing <4000 grams mostly did not experience a reduction in the width of the DRA below umbilicus (fixed) was 66 people (58.9%). Chi Square test results showed that there was a relationship between large baby weight and a reduction in the width of the DRA below umbilicus (p value <0.05). Postpartum women with not macrosomic babies were 0.1 times more likely to experience a reduction in the width of the DRA below umbilicus compared to women with macrosomic babies (p value=0.002; CRR=0.14;95%CI=0.02-0.93).
The results of this study are in line with research by Fitriahadi 21. With a quasi-experimental research model and similar types of interventions. The results of the study stated that most of the decrease in DRA occurred quickly in the treatment group (plank exercise) by 10 (66.65), while a slower decline in DRA occurred in the untreated group (control group) by 9 (60%), supported by bivariate analysis with p value = 0.003, this proves that there was an effect on strengthening the rectus abdominis muscle to reduce the DRA distance in postpartum women.
The results of the study are in line with previous research that there was an effect of sit-up exercise with prone plank exercise on decreasing abdominal circumference in adolescent girls13. Other research also stated that exercise will have an effect after being done for 6 weeks, for example, weight training can increase muscle strength by 20.1% within those weeks22. In general, previous research by Khandale & Hande also stated that abdominal muscle training can reduce DRA in early postpartum women and can prevent complications due to DRA23.
This research still has some limitations. This research method is still very simple and needs to be improved for the better in future research. The examination is also carried out in a simple manner, the use of other, more sophisticated examination tools is needed in future research. Likewise, this study only evaluates short-term effects, then, long-term research to determine long-term effects also needs to be done. The use of the results of this study must be responsible to avoid misunderstanding.
CONCLUSION
Based on data analysis, it was found that there was a reduction in the width of the DRA below umbilicus in postpartum women with treatment of 42 people (67.7%) while in the control group only 15 people (24.2%). Thus, it can be concluded thatthere is an effect of plank exercise on changes in the distance of the DRA below umbilicus and there is a relationship between plank exercise and a reduction in the width of the DRA below umbilicus in postpartum women.
Recommendations: As a recommendation from this study, physiotherapists would be able to advise postpartum women to do plank exercise in reducing various postnatal complaints and increasing quality of life both in the community and at home.
Ethical Clearance: This research was approved by the East Jakarta Health Service Center with reference number 1950/1.772.2.
Acknowledgements: We would like to thank the postpartum women in Makassar Health Center, East Jakarta who are willing to participate in this research.
REFERENCE
1. Lee D, Lee L, McLaughlin L. Stability, continence and breathing: The role of fascia following pregnancy and delivery. J Bodyw Mov Ther. 2008;12(4); 333-348.
2. Estiani M, Aisyah A. Faktor-Faktor Yang Berhubungan Dengan Kejadian Diastasis Rekti Abdominis Pada Ibu Post Partum Di Wilayah Kerja Uptd Puskesmas Sukaraya Baturaja. J Keperawatan Sriwij. 2018; 5(2); 24-31.
3. Rett MT, Braga MD, Bernardes NO, Andrade SC. Prevalence of diastasis of the rectus abdominis muscles immediately postpartum: Comparison between primiparae and multiparae. Brazilian J Phys Ther. 2009; 13(4) ;275-280.
4. Michalska A, Rokita W, Wolder D, Pogorzelska J, Kaczmarczyk K. Diastasis recti abdominis – A review of treatment methods. Ginekol Pol. 2018; 89(2):97-101.
5. Mota P, Pascoal AG, Carita AI, Bø K. Normal width of the inter-recti distance in pregnant and postpartum primiparous women. Musculoskelet Sci Pract. 2018;35; 34-37.
6. Walton LM, Costa A, LaVanture D, McIlrath S, Stebbins B. The effects of a 6 week dynamic core stability plank exercise program compared to a traditional supine core stability strengthening program on diastasis recti abdominis closure, pain, oswestry disability index (ODI) and pelvic floor disability index score. Phys Ther Rehabil. 2016;3(1); 3.
7. Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J. 2007;18(3); 321-328.
8. Aswini D, Srihari SK. An Overview of the Studies on Diastasis Recti Abdominis in Postpartum Women. J Gynecol Womens Heal. 2019; 14(5).
9. Ambarwati ER. Asuhan Kebidanan Nifas. Nuha Medika; 2010.
10. Candido G. LT. JPA. Risk factors for diastatis of the recti abdominis. J Assoc Chart Physiother Women’s Heal. 2005;97(January 2005); 49-54.
11. Gitta S, Magyar Z, Tardi P, et al. How to Treat Diastasis Recti Abdominis with Physical Therapy: A Case Report. J Dis. 2016;3(2); 16-20.
12. Acharry N, Kutty RK. Abdominal Exercise With Bracing, a Therapeutic Efficacy in Reducing Diastasis-Recti Among Postpartal Females. Int J Physiother Res. 2015; 3(2); 999-1005.
13. Wijayanti D. Perbedaan Pengaruh Sit-up Exercise Dan Prone Plank Exercise Terhadap Penurunan Lingkar Perut Remaja Putri. Publ Manuscript, Univ Aisyiyah Yogyakarta. Published online 2016; 1-16.
14. Schoenfeld BJ, Contreras BM. The long-lever posterior-tilt plank. Strength Cond J. 2013; 35(3):98-99.
15. Lee J, Jeong K, Lee H, et al. Comparison of three different surface plank exercises on core muscle activity. Phys Ther Rehabil Sci. 2016;5(1); 29-33.
16. Sugiyono. Metode Penelitian Pendidikan Pendekatan Kuantitatif, Kualitatif Dan R&D. Alfabeta; 2013.
17. Bursch SG. Interrater reliability of diastasis recti abdominis measurement. Phys Ther. 1987;67(7); 1077-1079.
18. Mantle J, Haslam J, Barton S. Physiotherapy in Obstetrics and Gynaecology. Elsevier Ltd; 2004.
19. Chiarello CM, McAuley JA. Concurrent validity of calipers and ultrasound imaging to measure interrecti distance. J Orthop Sports Phys Ther. 2013;43(7); 495-503.
20. Bennett VR, Brown LK. Myles Textbook for Midwives. Churchill Livingstone; 1999.
21. Fitriahadi E. Pengaruh Penguatan Otot Rectus Abdominis Terhadap Penurunan Tfu Pada Ibu Postpartum Pervaginam Di Bpm Kabupaten Sleman. J Kebidanan. 2019; 8(1); 61.
22. Sudarsono S. Penyusunan Program Pelatihan Berbeban Untuk Meningkatkan Kekuatan. J Ilm SPIRIT. 2015;12(1); 31-43.
23. Khandale SR, Hande D. Effects of Abdominal Exercises on Reduction of Diastasis Recti in Postnatal Women. Int J Heal Sci Res. 2016; 6(6); 182. www.ijhsr.org
| Citation: Lisnaini. Effect of plank exercise on diastasis recti abdominis lower umbilicus in postpartum women, International Journal of Medical and Exercise Science, March 2022; 8(1): 1219-1227. |
James Wilson HasoloanManik1, KiranaWardhani2, Adinda Amira Putri3, JeremiaBernardito4, Abi Wiranata5, Alberta YatiWulang6, Lucky Anggiat7
Corresponding Author:
7Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
Email: lucky.panjaitan@uki.ac.id
Authors:
1Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
2-6 Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
| ABSTRACT |
Background: Physiotherapists, as health care professionals, also have a role in providing main services in primary health care facilities. The practice of physiotherapy in the clinic can be done independently, or in collaboration or integrated with other health care professionals. Physiotherapy services with direct access will facilitate the patients to get physiotherapy services. This study aimed to observe one of physiotherapy service model with direct access in Indonesia.
Methods: This research is observational study and observed a clinic that provides direct access to the physiotherapy without having to go through a doctor or other health care professionals. The clinic being observed is the NT Clinic, which is an integrated clinic between general practitioners, medical specialists, and dentists.
Results: In a one-year service from January-December 2021, physiotherapists have handled 1,184 patient visits. The direct access to physiotherapy services at NT Clinic mostly treat patients with musculoskeletal conditions. Physiotherapists at NT Clinic also prioritize manual therapy with types of massage, joint mobilization, and stretching. Then intervention using ultrasound is also the most frequently used intervention and is followed by exercise therapy.
Conclusion.Physiotherapy services at NT Clinic are easy to reach by patients and are supported by medical specialists who can collaborate to provide optimal service to patients. Cases handled by physiotherapists at NT Clinic are musculoskeletal and neuromuscular. With direct access, physiotherapists can provide optimal services for patients based on the patient’s age, case, and appropriate intervention. Furthermore, physiotherapists can also provide referral options and receive referrals from medical specialists if needed.
Keywords: Physiotherapy, Direct Access, Primary Health Care, Clinic.
| Received on 4thFebruary 2022, Revised on 19thFebruary 2022, Accepted on 26thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.006 |
INTRODUCTION
Indonesia provides various health services, such as independent practice, community health centers, clinics, and hospitals1. Health services must include health promotion, preventive, curative, and rehabilitative. Health services consist of health care professionals who can work independently or in collaboration. Community health centers, clinics, and hospitals are health services with a collaborative work system. Clinical services are categorized into primary service facilities which are the foremost health services2.
According to the Regulation of the Minister of Health of the Republic of Indonesia Number 9 of 2014, a clinic is a health service facility that arranges individual health services and provides medical services or specialist3. Health service facility is a tool and/or place used to organize health service efforts, whether health promotion, preventive, curative or rehabilitative carried out by the government, local government, and/or the community. Physiotherapists, as health care professionals, also have a role in providing main services in primary health care facilities4.
Physiotherapy services are included to health services that provided to patients in terms of develop the body movement functions which include improvement, maintenance, and recovery using modalities such as exercise therapy, electrical modalities, and others5,6. In physiotherapy services, there are some patients with various disorders such as musculoskeletal (orthopedic or sports injuries), neuromuscular (neurological disorders), pediatrics (child development, neurology), cardiovascular and respiratory, integumentary and women’s health (SPA, beauty care)7. Physiotherapy services are also found in health centers, general hospitals, specialist hospitals and/or independent practice2,8.
The practice of physiotherapy in the clinic can be done independently, or in collaboration or integrated with other health care professionals such as medical specialists and pharmacy services8.
Physiotherapy services focus on patients through flow that can be accessed directly or through referrals from other health care professionals or fellow physiotherapists. Referrals for physiotherapy to other health care facilities/hospitals are made if the patient/client refuses physiotherapy services, requires further examination, or requires other interventions that are not available at the clinic2,9.
Physiotherapy services with direct access will facilitate the patients to get physiotherapy services. This solution was initiated by the Indonesian government4,7. In line with this regulation, the World Physiotherapy organization also states that physiotherapist can work an important role in direct health promotion, preventive, curative and rehabilitative activities10.
Several countries also already implemented similar rules so that the public’s health status can be improved properly with direct access to physiotherapy services11–13.
This study aimed to observe one of physiotherapy service model with direct access in Indonesia. The results of this study are indispensable as initial research because of the absence of research data on direct access to physiotherapy in Indonesia. This research was conducted at a clinic in North Jakarta, Indonesia which is integrated with the services of general practitioners, medical specialists, dentists and physiotherapist. In addition, the results of this study can be used as a reference for physiotherapists to build direct access physiotherapy services that integratedwith other health care professionals in primary health care service clinic.
METHODOLOGY
This research is observational study and observed a clinic that provides direct access to the physiotherapy without having to go through a doctor or other health care professionals. The clinic being observed is the NT Clinic, which is an integrated clinic between general practitioners, medical specialists, and dentists. The clinic provided us access to information related to direct access to physiotherapy services and a brief profile of the clinic.
The first information was the clinic profile, which is the vision and mission of the NT Clinic. Then, we continued to collect information on the flow of direct access physiotherapy services in the form of tables and descriptions. Next, we collected the data of active physiotherapists, physiotherapists’ level of education, and the availability of existing modalities and facilities.
The next data was the demographics of active patients that cover the number of patients who come directly to the physiotherapist both referrals and independent arrivals, age range, gender. The last data was the classification of cases handled by physiotherapists, some details of cases that are often found, and interventions carried out by physiotherapist. All data were processed using Microsoft Excel and presented in the form of tables and graphs.
RESULTS AND DISCUSSION
NT Clinic Profile: The vision of NT Clinic is to become a health clinic that is trusted by the community and its mission is to provide the best, affordable, and quality health services. The NT Clinic is a primary health care clinic led by a neurologist. Other services available are pediatricians, obstetricians, internal medicine specialists, neurologists, dentists, and physiotherapists. In addition, NT Clinic also hires nurses to help the health services run properly. Even though NT Clinic is led by a neurologist, all services provided by them can be accessed by patients directly based on the patient’s preference without having to go to the doctor, including physiotherapy.
Physiotherapy Direct Access Service Flow: The flow of physiotherapy services at NT Clinic as an outpatient clinic is in accordance with the Regulation of the Minister of Health of the Republic of Indonesia year 2015 Number 654. The service flow starts from registration via the website, telephone/WhatsApp, or face to face. Patients can come with a referral from a doctor or independently. New patients must register at the receptionist by providing an identity card. If the patient uses insurance, the insurance card must be given to the receptionist. The receptionist will fill in the patient identity section on the “Physiotherapy Patient Status Card”.
After registering, the receptionist will fill in patient data and tell the patient to go to the physiotherapy service. Furthermore, the physiotherapist will conduct an assessment to determine the appropriate physiotherapy intervention based on the diagnosis. If there is no indication to get physiotherapy services, the patient will be referred back to the referrer or the appropriate health care professionals (general or medical specialist) or after undergoing a series of physiotherapy processes. After receiving the therapeutic procedure, the patient returns to the receptionist to complete the administration.
Physiotherapy Service Profile: Physiotherapists who work in direct access physiotherapy services consist of 3 physiotherapists.
Led by a physiotherapist with a master’s degree with 2 physiotherapists who become general physiotherapists with diploma education. The availability of modalities is also quite complete. All profiles are presented in the following table1.
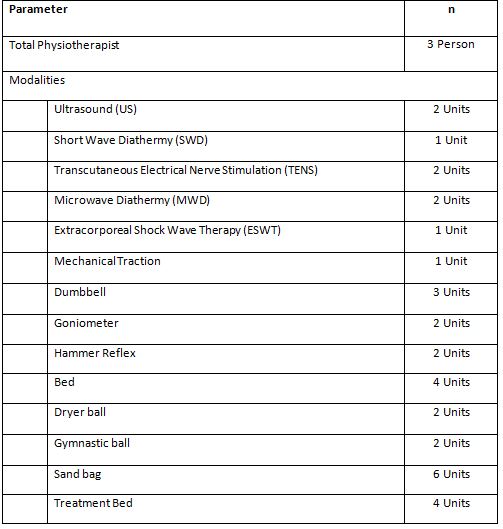
It can be seen in the table 1 physiotherapists are supported with various modalities. As well as several exercise therapy tools and treatment beds that support the best interventions for patients (Figure 1).

In a one-year service from January-December 2021, physiotherapists have handled 1,184 patient visits. Detailed demographic data on the number of patients per month can be seen in table 2.
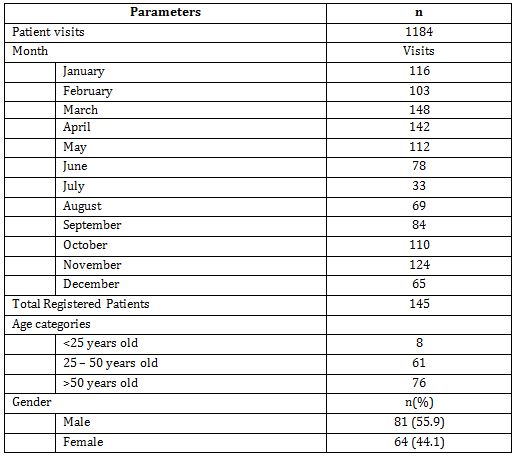
From the data, we can see that patients are quite high, indicating that patients are disciplined to take part in the physiotherapy program. Seen in June and July, there was a decrease in the number of patients to below 80 people in 1 month due to the second wave of COVID-19 in Indonesia. With a total of 145 patients registered in 1 year, it is also seen that active patients are dominated by patients over 50 years of age with mostly male (55.9%).
The next data is the classification of cases handled with detailed case diagnosis for the 10 most cases. In addition, the data related to the use of physiotherapy interventions were also presented for each patient who came to physiotherapist.
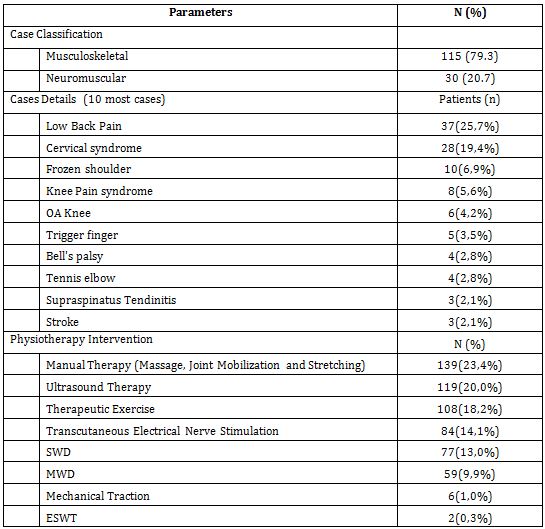
From the data in table 3, it can be seen that the direct access to physiotherapy services at NT Clinic mostly treat patients with musculoskeletal conditions, but there is also a large proportion of neuromuscular disorders both centrally and peripherally. This is also in line with research conducted by Demont et al. (2021) that it is true that physiotherapists in primary care have more patients with musculoskeletal conditions14. Physiotherapists will work an important role in reducing musculoskeletal disorders in the community through primary health services. Physiotherapists will be more efficient in treating patients. In fact, it was further explained that it would be able to improve the quality of life of patients, reduce disability in the community, and reduce the cost of health services. With direct access, patients can immediately go to a physiotherapist and get the right treatment, without having to spend time seeing a medical specialist15,16. Moreover, other studies have also concluded that patients with musculoskeletal conditions get better results and require less other services to improve their health conditions1715. However, taking into account the condition of the patient’s case, which may require a referral to a medical specialist, both at the beginning of the examination and after therapy9,12,14.
Physiotherapists at NT Clinic also prioritize manual therapy with types of massage, joint mobilization, and stretching. Then intervention using ultrasound is also the most frequently used intervention and is followed by exercise therapy. Research by Anggiat et al. also shows that physiotherapists use manual therapy more than other modalities18. However, exercise therapy is also the most popular intervention and is very often used in direct access physiotherapy practice8,19. From the intervention, the physiotherapists can use manual therapy and exercise to be the main intervention, supported by various modalities such as ultrasound and electrical stimulation. Diathermy interventions in several studies have been abandoned because of their high cost and low effectiveness compared to manual therapy and exercise20,21. However, interventions based on electro physical agents still dominate in Asia.
This study is an initial study that only made observations in one clinic. In the future, larger studies are needed and involve many clinics or health care services that provide direct access to physiotherapy.
CONCLUSION
NT Clinic is a primary health care clinic that integrates physiotherapy, medical specialist, and support direct access to physiotherapy services. Thus, physiotherapy services at NT Clinic are easy to reach by patients and are supported by medical specialists who can collaborate to provide optimal service to patients.
NT Clinic’s physiotherapy patients are dominated by patients over 50 years of age. Cases handled by physiotherapists at NT Clinic are musculoskeletal and neuromuscular such as low back pain, cervical syndrome, frozen shoulder, knee syndrome, and knee OA. The most frequently used physiotherapy modalities are manual therapy, US, exercise therapy, TENS, and MWD. With direct access, physiotherapists can provide optimal services for patients based on the patient’s age, case, and appropriate intervention. Furthermore, physiotherapists can also provide referral options and receive referrals from medical specialists if needed.
As a recommendation, the current physiotherapy service system at NT Clinic can be an example for colleagues to provide direct access physiotherapy services. With the intervention of manual therapy, exercise therapy, and ultrasound, the physiotherapist is sufficient to provide optimal services supported by other facilities such as bed treatment and exercise equipment.
Acknowledgements: The researcher would like to thank Kirana Wardhani, Adinda Amira Putri, JeremiaBernardito, Abi Wiranata, Alberta YatiWulang, and all NT Clinic’s physiotherapists for collecting and providing the data.
Conflict of interest: The author has no conflict of interest to declare.
Funding of study; This study was self-funded study
Compliance with Ethics: This study does not provide intervention and endangers the respondents so that it does not use ethical studies. However, data collection in this study was carried out with the acceptance of the university with reference no. 351/UKI.F8.PF/PP.5.1/2021 and permission from the clinic.
REFERENCES
1. Kementerian Kesehatan Republik Indonesia. Peraturan Pemerintah No. 47 Tahun 2016 Tentang Fasilitas Pelayanan Kesehatan.; 2016:1-16.
2. Holdsworth LK, Webster VS. Direct access to physiotherapy in primary care: Now? – And into the future? Physiotherapy. 2004; 90(2):64-72.
3. Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia no.9 Tahun 2014 tentang Klinik. Republik Indones. 2014;9:1-16.
4. Kemenkes RI. Peraturan Menteri Kesehatan Republik Indonesia Nomor 65 Tahun 2015 Tentang Standar Pelayanan Fisioterapi. Menteri Kesehat Republik Indones. 2015;16(2):39-55.
5. Manurung NSA. Manajemen Proses Fisioterapi Pada Satu Rumah Sakit Swasta Di Jakarta Timur. J Ilm Fisioter. 2020; 20(2):54-63.
6. World Confederation for Physical Therapy. Guideline for standards of physical therapy practice. Published online 2011:1-19. https://world.physio/sites/default/files/2020-07/G-2011-Standards-practice.pdf
7. Kemenkes RI. Peraturan Menteri Kesehatan No.80 Tahun, 2013;(1536):1-13.
8. Manurung NAS, Anggiat L. Entrepreneurship Models in Physiotherapy Practice: an Observational Study. Int J Med Exerc Sci. 2021;7(3):1088-1095.
9. Deyle GD. Direct Acces Physical Therapy and Diagnostic Responsibility: The Risk-to-Benefit Ratio. J Orthop Sport Phys Ther. 2006; 36(9): 632-634.
10. World Confederation for Physical Therapy. Direct access and patient/client self-referral to physical therapy: Policy Statement. Published online 2019.
11. Leemrijse CJ, Swinkels ICS, Veenhof C. Direct access to physical therapy in the Netherlands: Results from the first year in community-based physical therapy. Phys Ther. 2008;88(8):936-946.
12. Praestegaard J, Gard G, Glasdam S. Practicing physiotherapy in Danish private practice: An ethical perspective. Med Heal Care Philos. 2013; 16(3):555-564.
13. Bury TJ, Stokes EK. Direct access and patient/client self-referral to physiotherapy :A review of contemporary practice within the European Union. Physiother (United Kingdom). 2013; 99(4): 285-291.
14. Demont A, Bourmaud A, Kechichian A, Desmeules F. The impact of direct access physiotherapy compared to primary care physician led usual care for patients with musculoskeletal disorders: a systematic review of the literature. Disabil Rehabil. 2021;43(12): 16371648.
15. Ojha HA, Snyder RS, Davenport TE. Direct access compared with referred physical therapy episodes of care: A systematic review. Phys Ther. 2014;94(1):14-30.
16. Piano L, Maselli F, Viceconti A, Gianola S, Ciuro A. Direct access to physical therapy for the patient with musculoskeletal disorders, a literature review. J Phys Ther Sci.2017; 29(8):1463-1471.
17. Gagnon R, Perreault K, Berthelot S, et al. Direct-access physiotherapy to help manage patients with musculoskeletal disorders in an emergency department: Results of a randomized controlled trial. Acad Emerg Med. 2021; 28(8): 848-858.
18. Anggiat L, Altavas AJ, Budhyanti W. Joint Mobilization: Theory and evidence review. Int J Sport Exerc Heal Res. 2020;4(2):86-90.
19. Caparrós T, Pujol M, Salas C. General guidelines in the rehabilitation process for return to training after a sports injury. Apunt Med l’Esport. 2017; 52(196): 167-172.
20. Abe Y, Goh AC, Miyoshi K. Availability, usage, and factors affecting usage of electrophysical agents by physical therapists: A regional cross-sectional survey. J Phys Ther Sci. 2016; 28(11):3088-3094.
21. Panjaitan LA. Penggunaan Terapi Elektro-fisis Pada Satu Rumah Sakit Umum Swasta di Jakarta. J Fisioter.2020; 20(2):40-45.
| Citation: James Wilson HasoloanManik, KiranaWardhani, Adinda Amira Putri, et al. Direct access physiotherapy service model in primary health care facility: an observational study , International Journal of Medical and Exercise Science, March 2022; 8(1); 1210-1218. |
K. Kamatchi1, Rajesh Kumar.N.T2, Kandhasamy.S3
Corresponding Author:
1Assistant Professor, Faculty of Physiotherapy, A.C.S. Medical College and Hospital Campus, DR. MGR. Educational and Research Institute, Deemed to be University, Chennai, Tamil Nadu, India
Mail Id: kamatchi.physio@drmgrdu.ac.in
Co-Authors:
2, 3 MPT Students, Faculty of Physiotherapy, A.C.S. Medical College and Hospital Campus, DR. MGR. Educational and Research Institute, Deemed to be University, Chennai, Tamil Nadu, India
| ABSTRACT |
Background: Varicose veins are torturous, widened superficial veins in the subcutaneous tissues of the legs which are often easily visible these are generally larger than 3mm in size. According to the population in India patients with varicose veins in India is about 15-20% of populations and is increasing day by day. Objective of the study is to find the effectiveness of aerobic exercise versus Buerger’s exercise in varicose vein among security guards.
Methodology: This is a comparative study with 30 patients of the security guards from A.C.S. Medical College and Hospital. The inclusion criteria will be both males and females with the age group of 35 to 55 years and the patients having grade 2 oedema. In this study group A consists of 15 patients was trained with aerobic exercise training and group B consists of 15 patients was trained with Buerger’s exercises. Aerobic exercise was performed for 30 minutes per day for four sessions in a week and this was given for 12 weeks and Buerger’s exercises was performed for 30 minutes per day for four session in a week and this was given for 12 weeks. The pre and post-test values were compared using the VAS (visual analogous scale), 6- minute walk test.
Result: On comparing Pre test and Post test within Group A& Group B on Visual Analog Scale & 6 Minute Walk Test score showed highly significant difference in Mean values at P ≤ 0.001 but buerger’s exercise is more effective than aerobic exercise.
| Conclusion: Buerger’s exercise is more effective on reducing varicose vein among security guards |
Keywords: Varicose vein; Aerobic exercise; Buerger’s exercise.
| Received on 29thJanuary 2022, Revised on 19thFebruary 2022, Accepted on 26thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.005 |
INTRODUCTION
Generally, the leg veins have one-way valve in them so that muscle contract them and blood can go only in one direction this up the leg which are seen in normal veins.Due to which there is failure of valves to close properly and allows in both directions. This backward flow of blood is known as venous reflex 1,2.
Due to this there is accumulation of blood in legs causing varicose veins. Varicose veins are torturous, widened superficial veins in the subcutaneous tissues of the legs which are often easily visible. Varicose veins are among the most common chronic conditions seen by physicians today. A varicose vein, sometimes called varicosity occurs when a valve weakness putting more pressure on the other valves and causing blood to stagnate 3, 4.
There are generally larger than 3mm in size located on the size of the calf muscles.Varicose veins are preventable. Maintaining healthy body weight and doing exercises help lessen their emergence appropriate exercise can be the best preventive and defensive strategies against varicose veins 5.
Any program of regular exercises circulation improves muscle tone and helps prevent varicosities. However, high-impact aerobics, jogging, strenuous cycling, or any intense activity may increase blood pressure in the legs and accentuate varicose vein. Walking is the great exercise for the lower leg area–either out in the open or in a treadmill especially with the incline level simple intervention like leg elevation, water immersion and exercise should be studied6,7.
The mechanism of Buerger’s exercises use gravitational changes in positions that are applied to smooth musculature of vessels and to vascular 8. Gravity helps alternate to empty and fill blood columns, which can eventually increase transportation of blood through them9.
The exercises involve the individual lying flat in bed with the legs elevated at 45 degrees until blanching occurs or for a maximum of 2 minutes. The patient then sits on the edge of the bed with the feet hanging down. Further exercise includes dorsiflex, plantarflex, then inward and outward movements of the feet, followed by flexing and extending the toes 10, 11.
Before and after World War 2 medical experts did not know how to operate or treat the patient suffering from atherosclerosis or vessel occlusion, as well as stiffening in their peripheral arteries. Some medical genius at that time developed postural treatment to improve circulation in the lower extremities12-15.
Aim & Need of the Study: Varicose veins are torturous, widened superficial veins in the subcutaneous tissues of the legs which are often easily visible these are generally larger than 3mm in size. They are usually enlarged and are located on the inside of the calf muscles. Varicose veins are more common seen in women than men. According to the population in India patients with varicose veins in India is about 15-20% of populations and is increasing day by day. This study aims to find the comparative effect between buerger’s exercise and aerobic exercise.
Hence the need of the study is to find the effectiveness of aerobic exercise versus Buerger’s exercise in varicose vein among security guards.
This was an experimental comparative study pre and post study conducted at ACS Medical College and hospital Chennai. Total 30 patients were selected for this study; they were security guard in ACS College. The study conducted for study duration of 3 months. Inclusion criteria for the study were both male and female aged between 35 to 55 years; Patients were clinically diagnosed with varicose vein with edema grade 2. Patient with deep vein thrombosis, recent lower limb fracture, uncooperative subjects, any neuropathies or ulcers in lower limb, patients undergone with recent lung surgical intervention in lower limb were excluded from this study. Outcome measures for the study were VAS (Visual Analog Scale) and 6 min walk test
Procedure: The patients who fulfill the inclusion criteria were included in the study. The consent was obtained from the patient and the assessment was done and they were divided into two groups each group having 15 patients. Group A patients received aerobic exercise. Group B received Buerger’s exercise. Both groups received treatment duration for 4 sessions in a week up to 12 week after 12 weeks the patients was assessed by pre and post values of VAS scale and 6 minutes’ walk test.
Aerobic exercises
Walking or running: Walking just 20 minutes a day and running minimize the stress on your joint.
Bicycle legs: 5 minutes riding a bicycle or lying on back put legs in the air, bending them at knee. Pedal them slowly either leg at once or alternate one at a time.
Lunges: 5 minutes stand with legs apart. Step forward slow bending knee and make sure to keep knee directly above the ankle hold it then slowly straighten the leg and step back to original position, repeat with the other leg. While standing with Leg straight, rise up on tip toes and then lower back down.
Buerger’s exercise: Buerger Allen exercise- specific exercises intended to improve circulation to the feet and legs. The lower extremities are elevated to a 45 to 90 degree angle and supported in this position until the skin blanches (appears dead white). The feet and legs are then lowered below the level of the rest of the body until redness appears (care should be taken that there is no pressure against the back of the knees); finally the legs placed on the bed for few minutes.
The length of the time for each position varies with the patient’s tolerance and the speed with which colour change occurs. Usually the exercises are prescribed so that the legs are elevated for 2 to 3 minutes, down 5 to 10 minutes and then flat on the bed for 10 minutes.






Data Analysis: The collected data were tabulated and analyzed using both descriptive and inferential statistics. All the parameters were assessed using statistical package for social science (SPSS) version 24.
Paired t-test was adopted to find the statistical difference within the groups & Independent t-test (Student t-Test) was adopted to find statistical difference between the groups.
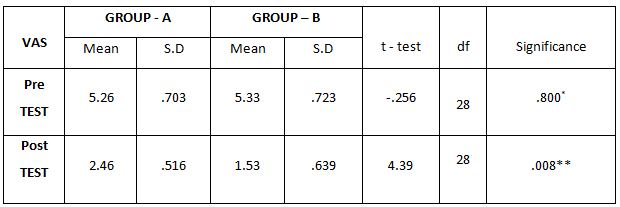
The above table reveals the Mean, Standard Deviation (S.D), t-test, degree of freedom(df) and p-value between (Group A) & (Group B) in pre test and post test weeks.
This table shows that statistically significant difference in post test values between Group A& Group B (**- P ≤ 0.05)
This table shows that there is no significant difference in pre test values between Group A& Group B (*P > 0.05).
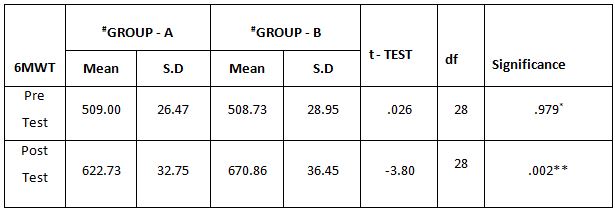
The above table reveals the Mean, Standard Deviation (S.D), t-test, degree of freedom(df) and p-value between (Group A) & (Group B) in pre test and post test weeks.
This table shows that there is no significant difference in pre test values between Group A& Group B (*P > 0.05). This table shows that
statistically significant difference in posttest values between Group A& Group B (**- P ≤ 0.05)

The above table reveals the Mean, Standard Deviation (S.D), t-value and p-value between pre-test and post-test within Group – A &Group – B. There is a statistically highly significant difference between the pre test and post test values within Group A and Group B(***- P ≤ 0.001).


The above table reveals the Mean, Standard Deviation (S.D), t-value and p-value between pre-test and post-test within Group – A &Group – B.
There is a statistically highly significant difference between the pre test and post test values within Group A and Group B(***- P ≤ 0.001).

RESULTS
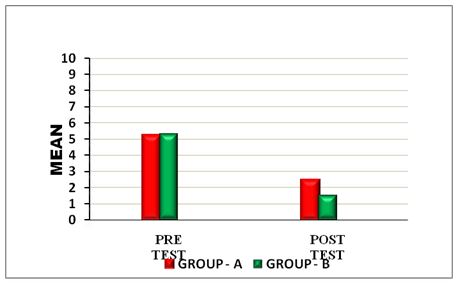
On comparing the Mean values of Group A & Group B on Visual Analog Scale Score, both the groups showed significant decrease in the post test Mean values, but (Group B – Buerger’s Exercise) shows 1.53 which has the Lower Mean value is effective than (Group A -Aerobic Exercise) 2.46 at P ≤ 0.05. Hence Null Hypothesis is rejected.
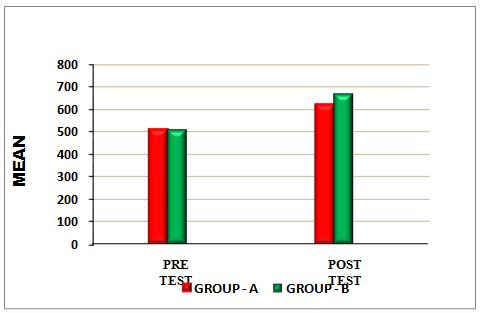
On comparing the Mean values of Group A & Group B on 6 Minute Walk Test Score, both the groups showed significant increase in the post test Mean values but (Group B – Buerger’s Exercise) shows 670.86 seconds which has the Higher Mean value is effective than (Group A -Aerobic Exercise) 622.73 , secondsat P ≤ 0.05. Hence Null Hypothesis is rejected.
On comparing Pre test and Post test within Group A& Group B on Visual Analog Scale & 6 Minute Walk Test score showed highly significant difference in Mean values at P ≤ 0.001
DISCUSSION
The purpose of this study is to find out the comparative effect between aerobic exercises versus Buerger’s exercise in varicose veins. Varicose veins are torturous, widened superficial veins in subcutaneous tissues of the legs which are often visible.
The study was carried out and the result was drawn by using vas scale and 6-minute walk test as the outcome measure. 30 patients diagnosed as varicose veins the age group between 35- 55 years. Study place was ACS Medical College and hospital, Chennai. The patients are evaluated and divided into two groups. Group A included 15 subjects treated with aerobic exercise and Group B included 15 subjects treated with Buerger’s exercise. In the present study
When comparing the Mean values of Group A & Group B on Visual Analog Scale Score, both the groups showed significant decrease in the post test Mean values, but (Group B – Buerger’s Exercise) shows 1.53 which has the Lower Mean value is effective than (Group A -Aerobic Exercise) 2.46 at P ≤ 0.05.
When comparing the Mean values of Group A & Group B on 6 Minute Walk Test Score, both the groups showed significant increase in the post test Mean values but (Group B-Buerger’s Exercise) shows 670.86 seconds which has the Higher Mean value is effective than (Group A -Aerobic Exercise) 622.73 seconds at P ≤ 0.05.
On the comparing the pre and post values by VAS (visual analogous scale) and 6 minute walk test both the exercises shows significant results but buerger’s is more effective than aerobic exercise. Evidence of similarly enhanced buerger’s exercise has been found in the previous studies.
Jian Wei-Ya, et al. (2009) compared with conventional rehabilitation training, buerger’s exercise was more effective in reducing the post –surgery pain asd swelling of patients with the lower limb fractures.
Chyong Fang Chang Rn, MSN et al. (2015) showed that buerger’s exercise combined with the health promoting program significantly improved among community residents at high risk for diabetic foot ulceration.
Poonam Thakur, et al. (2019) proved that buerger’s exercise is improving peripheral circulation among patients with diabetes mellitus admitted in sharda hospital at Noida.
Chyong Fang Chang, et al. (2015) found that buerger’s exercise benefits for PAOD patient’s post- operative patients with orthopaedics and gynaecology problems by improving local circulation.
Ethical clearance: There was no risk of conducting this study.Ethical clearance was obtained from the ethical Institutional Review Board of Faculty of Physiotherapy, Dr. MGR. Educational and Research Institute, Chennai with reference No. A43/PHYSIO/IRB/2018-2019 approval letter dated 07/01/2019.
Conflicts of Interest: There is no conflict of interest to conduct this study.
Fund for the study: This is self-funded study.
CONCLUSION
The present study concluded that both exercise showed a significant results but Buerger’s exercise is more effective than aerobic exercise.
REFERENCES
1. Clendo J A, child J D, stowell T et al., immediate effects thoracic manipulation in patients with neck pain: a randomized clinical trial. Man ther. 2005 May; 10(2); 127-35.
2. Conley MS, mayor RA, Bloomberg JJ, et al., non-invasive analysis of human neck muscle function. Spinc, 1995, 20; 2505-2512.
3. Ariens GA, bongers PM, Dowes M, et al., Are neck flexion, neck rotation, and sitting at work risk factor for neck pain? Occup environ med, 2001; 58; 200-207.
4. Haldemen S, carrol L, Cassidy JD, et al. Finding from bone and joint decade 2000-2010 task force on neck pain andits associated disorders. J Occup Environ med. 2010; Apr: 52(4); 424-7.
5. Janda V; muscles and motor control in cervicogenic disorder: assessment and management. In: physical therapy of the cervical and thoracic spine. 2nd ed. New York: Churchill Livingstone, 1994; pp. 195-216
6. Jull GA, falla DL et al. Clinical assessment of the deep cervical flexor muscles; the craniocervical flexion test. J manipulative physio ther. 2008 Sep.; 31(7); 525-33.
7. Jhohans blomgren et al., effects of deep cervical flexor training on impaired physiological functions associated functions with chronic neck pain: a systematic review. BMC musculoskeletal disorders 2018, 19:415.
8. Sinho Chung et al. Effects of the cranio cervical flexion and isometric neck exercise compared in patients with neck pain: A randomized controlled trail. Physiotherapy theory and practice, 2018:1-10.
9. Stretching Exercises to Prevent Work-related Musculoskeletal Disorders – A Review Article; Journal of Sports Science & Medicine, May 2017; 5(2):27-37.
10. Mohammed Ali et al. the effects of different exercise programs on size and function of deep cervical flexor muscles in patients with chronic non-specific neck pain: A systematic review of randomized. American journal of physical of physical medicine & rehabilitation, 2017; 96(8); 582-588.
11. Jin young Kim et al., Clinical effects deep cervical muscular activation in patients with chronic neck pain. J. Phys. Ther. Sci. 2016; 28; 269-273.
12. Akbari Asghar et al., investing the effects of stabilization exercise and proprioceptive neuromuscular facilitation exercise on cross-sectional area of deep cervical flexor muscles in patients with chronic non-specific neck pain. International journal of medical research &health science, 2016; 11; 502-508.
13. Amira hussian draz et al., efficacy of deep cervical flexor exercise for neck pain: a randomized controlled study. Turk J phys med rehab., 2016; 62(2); 107-115.
14. Eun young Kim et al., comparison of the effects deep cervical flexor strengthening and Mackenzie neck exercises on head forward postures due to the use of smart phones .Indian journal of science and technology, April 2015; Vol.8(S7); 567-575.
15. Dong yeon kang et al., deep cervical flexor training with a pressure biofeedback unit is an effective method for maintaining neck mobility and muscular endurance in college students with forward head posture. J. Phys. Ther. Sci. 2015; 27; 3207-3210.
16. Zaheen Ahmed iqbal et al., Flexor training using pressure biofeedback on pain and disability of school teachers with neck pain. J. Phys. Ther. Sci. 2013,25; 657-661.
17. Nezamuddin, MD., et al., Efficacy of pressure biofeedback guided deep cervical flexor training on neck pain and muscle performance in visual display terminal operators. Journal of musculoskeletal research. 2013; Vol. 16; No.03; 1350011.
18. Saad Ammar Al-Harbi, et al., compare the effects of deep cervical flexor strengthening exercises verses electrotherapy modalities on head forward postures resulting from the use of smart phones. World Journal of Pharmacy and Pharmaceutical Sciences, 2013; Volume 6; Issue 6; 266-277.
19. Petri salo et al., neck muscle strength and mobility of the cervical spine as predictors of neck pain: a prospective 6-year study, 2012; Spine 37(12); 1036-1040.
20. Takala ep et al., active neck muscle training in the treatment of chronic neck pain in women: A randomizes controlled trial .jama.2003 may 21; 289(19): 2509-16.
21. Geoffrey R. Williams et al., colony collapse disorder in context. Trends Ecol. 2012; Vol 20; 367-72.
22. Falla et al., the change in deep cervical flexor activity after training is associated with the degree of pain reduction in patients with chronic neck pain. Clin. J. Pain, 2012; 28 (7); 628-634.
23. Aquino RL, et al., applying joint mobilization at different cervical vertebral levels does influence immediate pain reduction in patiets with chronic neck pain. J Man Manip Ther. 2009; 17(2):95-100.
24. Luch E, et al., effects of deep cervical flexor training on pressure pain thresholds over myofacial trigger points in patients with chronic neck pain. J Manipulativ Physiol Ther. 2013 Nov-Dec; 36(9): 604-11.
| Citation: K. Kamatchi, Rajesh Kumar.N.T, Kandhasamy.S. A comparitive study to analyse the effectiveness of aerobic exercise versus Buerger’s exercise in varicose vein among security guards, International Journal of Medical and Exercise Science, March 2022; 8(1); 1199-1209. |
Kandhasamy.S1, Meena.S2, Rajesh Kumar.N.T3
Corresponding Author:
1MPT Student, Faculty of Physiotherapy, A.C.S. Medical College and Hospital Campus, DR. MGR. Educational and Research Institute, Deemed to be University, Chennai, India
Mail Id: aaronstark24@gmail.com
Co-Authors:
2Assistant Professor, Faculty of Physiotherapy, A.C.S. Medical College and Hospital Campus, DR. MGR. Educational and Research Institute, Deemed to be University, Chennai, India
3MPT Student, Faculty of Physiotherapy, A.C.S. Medical College and Hospital Campus, DR. MGR. Educational and Research Institute, Deemed to be University, Chennai, India
| ABSTRACT |
Background of the study: Neck pain is a common epidemiological problem in nowadays. Neck pain is more predominant in middle age and a typical condition influencing 20% to 70% of all inclusive community. Most instances of the neck pain are brought about by mechanical factors, for example, injuries and strains of the neck muscles or tendons. The objective of the study is to investigate the impacts of endurance training on deep cervical flexor muscles on neck pain using pressure biofeedback.
Methodology: A comparative study with 30 patients taken from the outpatient department of A.C.S Medical College and Hospital. Inclusion criteria were neck pain of VAS below 7, patients with forward head posture, cervical spondylosis, aged between 18 to 70, both genders with poor deep flexor endurance were selected for the study. Self-reported Performa was given to all the patients and then they will be divided into two groups. Group a patient will be receiving strengthening exercises and deep cervical flexor training with pressure biofeedback and group b will be receiving strengthening exercises only. Both group receiving treatment duration for four times in a week up to four weeks. After 4 weeks treatment patients were improved by numeric pain rating scale, neck handicap file scale.
Results: Cervical movement has increased essentially after four weeks training in experimental group contrasted with that in control group.
| Conclusion: Deep cervical flexor preparing with pressure biofeedback gives better clinical improvement as far as pain, cervical flexion, expansion ROM, DCF perseverance and NDI score. |
Keywords: Neck pain; Deep cervical flexor; Pressure biofeedback.
| Received on 28thJanuary 2022, Revised on 18thFebruary 2022, Accepted on 26thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.004 |
INTRODUCTION
Neck pain is a critical medical condition for grown-ups as well as for youthful. The beginning and course of neck pain is impacted by different elements with physical, psychosocial and individual elements communicating in the improvement of these disorders. Neck pain is turning out to be progressively pervasive in the public eye. Gauges show that 67% of people will endure neck pain at same phase of their life 1, 2.
Neck pain was portrayed as anon explicit agony in the district of the cervical thoracic intersection that is bothered by neck developments. Pain and disability of the neck is generally dominating among 20 to 60 years old. Neck pain predominance increments with age and become most normal in ladies around the fifth ten years of life. However the specific reason for the aggravation is obscure, most instances of neck pain are because of mechanical factors like injuries and strain of the muscles or tendons of neck 3.
Neck pain with related inability, the 1-years commonness in everybody went from 2% to 11% and from 11% to 14% in laborers detailed restricting their exercises as a result of neck pain. A few literary works investigated neck pain without reference into the upper appendages that endured something like 1 day. The worldwide point pervasiveness in 2010 was assessed to be 4.9% (females: 5.8%; guys: 4.0%)4.
Various physical constructions in the cervical locale can be wellspring of nociception, including zygapophyseal joints, vertebral end plates, muscles, tendons, brain structures, and the inter vertebral circle .However, proof is missing to help the theory that these patho-physical elements are an essential wellspring of mechanical neck pain across the age range in most of patients.
The Deep Cervical Flexor Muscle (DCF) are viewed as a significant stabilizer of the Head-on-neck pose .It has been hypothesized that when the muscle execution is hindrance, the harmony between the back neck stabilizers and the DCFs will be upset and appropriate arrangement and stance is lost, which is then liable to add to cervical disability. In this way Deep Cervical Flexor Muscle (DCF) preparing is prescribed to expand the perseverance of these postural muscles, to progress in neck pain 5.
The Cranio Cervical Flexor Test (CCFT) is a clinical test for the physical activities of the physical activity of the profound cervical flexor muscles, longus capitis, and colli. The perseverance of DCF was characterized as the most extreme time that subjects could keep a base pushing pressure more prominent than 50mmHg. Solid perseverance estimation followed a laid out convention utilizing a Pressure Biofeedback Unit 6.
In a 2012 moderate-quality systematic review of patient has revealed result estimates on 8 distinct instruments. Of these, the NDI was the most widely examined over an assortment of neck pain condition and has been converted into numerous dialects. The NDI was likewise widely surveyed for its psychometric properties. They tracked down the estimation properties of the NDI to be satisfactory, aside from dependability, and temporarily suggested its utilization7.
This is an Experimental study with sample size of 30 patients. This study was conducted at A.C.S Medical College and Hospital, Velappanchavadi, Chennai. The study duration was 4 weeks and sampling design was convenient sampling method. Inclusion criteria of the study were Neck pain of vas below 7, Patient with forward head posture, Patient with primary complaint of neck pain, subjects those aged 18 to 70, both genders and subjects having poor deep flexor endurance.
Patients with history of trauma to neck, bilateral upper limb symptoms, cervical radiculopathy, myogenic neck pain, positive 2 or more neurological signs, History of cervical surgery, non chronic neck pain, headaches occurring during the last six months were excluded from the study. Outcome measures for the study were Neck Disability Scale and Numeric Pain Rating Scale. Materials used in the study were towels and pressure biofeedback.
Procedure: The patients who full fill the inclusion criteria will be included in the study. Self-reported Performa will be given to all the patients and then they will be divided into two groups.Group A patient will be receiving strengthening exercises and deep cervical flexor training with pressure biofeedback and group B will be receiving strengthening exercises only.Both group receiving treatment duration for three times in a week up to four weeks.After the four weeks subjects will be assessed by NPRS,NDI scale.
Numerical Pain Rating Scale: The NPRS is a Segmental numeric form of the visual analogue scale (VAS) in which a respondent chooses an entire number (0-10 whole numbers) that best mirrors the force of his\her pain. The normal organization is a level bar or line22.
Cervical range of motion (CROM): Cervical ROM (dynamic) in flexion and expansion was estimated for each subject. Before estimation, the subject eliminated eye glasses, jewelry, T-shirt or tank top; and noticed a short exhibition of the cervical movement to be performed. To limit fluctuation in estimation brought about by contrasts in the subject body head position, and to be lay out an unbiased head and neck position, toward the beginning of each position measurement.
Flexion and extension:
Test Position: The subject in sitting position, with thoracic and lumbar spine supported by the back of a chair. The cervical spine is positioned in zero degrees of the rotation and later flexion.
Test Procedure: Neck movement degrees were measured on cervical flexion and extension. Specific instruction was given to the subjects for performance of neck flexion followed by chin tuck , then move head forward and downward as far as possible until limited by tightness or discomfort. Normal range of cervical flexion averages to around zero 0-50 degrees.
Specific instructions for neck extension was raise chin first, followed by move head backward, looking up as far as possible until limited by tightness or discomfort. Normal range of cervical extension averages to around 0-60 degree23.
Cranio-cervical Flexion Test (CCFT): The cranio cervical flexion test is performed with the patient in supine lying with the neck in an impartial position (no cushion) to such an extent that the line of the face is level and the line bisecting the neck longitudinally is flat to the testing surface. The uninflated pressure sensor is set in the curve of neck with the goal that it adjoins the occiput and is swelled to a steady benchmark tension of twenty mm Hg; this addresses a guidelines pressure sufficiently adequate to occupy the space between the testing surface and the neck yet doesn’t expand the lordosis. The input and course is given by the gadget to play out the necessary five phases of the test. The patient is told that the test is for precision rather than strength. The head gesturing activity is preformed delicately and gradually. The ever-evolving inward reach enactment and perseverance of the profound cervical flexors are tried by Cranio Cervical flexion tests. Pressure increments during the technique as the patient endeavors a progressive 3 endeavor of 2 mm Hg movement (20 mmHg to 30 mmHg). Likewise keep an isometric withdrawal during moderate tensions as a perseverance task.
Deep cervical flexor training: It targets deep flexors of the upper cervical district, the longus capitis, and colli, rather than the shallow flexors, sterno-cleidomastoid, and foremost scalene muscles, which flex the neck however not the head. The patient was told to perform and hold logically the inward scopes of Cranio Cervical Flexion while attempting to keep the shallow flexors loose. Patients were first instructed to play out a sluggish and controlled Cranio Cervical Flexion development. They were than prepared to have the option to statically hold dynamically expanding inward scope of Cranio Cervical Flexion.
Subjects were directed to the expansion the inward reach positions through criticism acquired structure the dial of an air-filled pressure sensor put behind the neck, which screens the slight leveling of the lordosis. This smoothing has been displayed to go with constriction of longus colli.

Strengthening exercises: To begin, sit in a seat with your feet level on the floor. Your weight ought to be somewhat forward so that you’re adjusted equally on your bottom. Loosen up your shoulders and keep your head level. Utilizing a seat with arms might assist you with keeping your equilibrium.
1. Press your palm against your temple. Resist with your neck muscles. Hold for 10seconds.Relax, Repeat multiple times.
2. Rehash the activity, pushing on your head. Rehash multiple times, Switch sides.
3. Rehash the activity, pushing on the rear of your head. Rehash multiple times.
For your wellbeing, check with your medical services supplier prior to beginning an activity program. Both group receiving conventional exercises for 15 minutes and experimental group receiving deep cervical flexor training for 10 minutes. Both group receiving conventional exercises three times week for four weeks .The experimental group receiving deep cervical flexor training thrice a week.

Neck disability index: This questionnaire has been intended to give us data regarding what your neck pain has meant for your capacity to oversee in daily existence. Every one of the 10 things is scored from 0-5. The most extreme score is along these lines 50. They got score can be duplicated by 2 to deliver a rate score. Incidentally, a respondent won’t finish some inquiry. The normal of any remaining things is then added to the finished items 24.
Data analysis: The graphic insights, rate investigation were utilized for classified factors and mean and S.D was utilized persistent factors. The investigation of slanted information between the gatherings was finished by Mann Whitney U test. Matched t test was utilized to examine the factors the inside the gathering, aside from pain. While, Wilcoxon marked
positions test was utilized to break down inside the gathering NPRS score. The factual tests were viewed as critical when the p esteem is under 0.05.
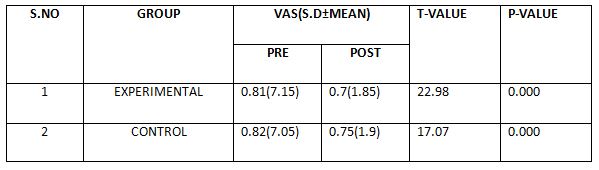
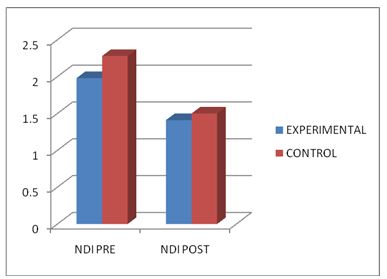
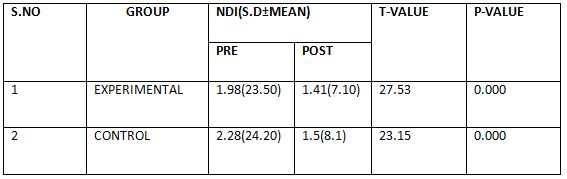
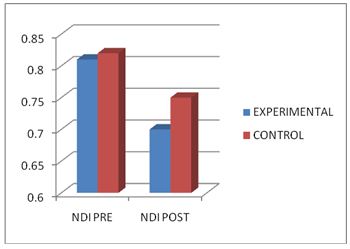
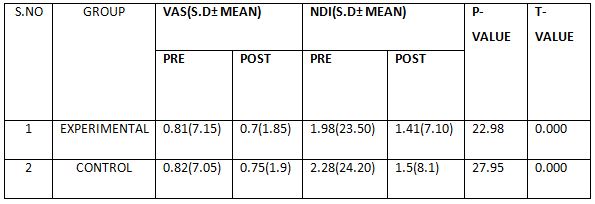
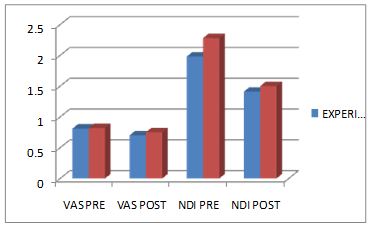
RESULTS
The trial group showed a fundamentally more noteworthy expansion in cervical ROM between post-preparing and the multi week detraining period, contrasted with control group. Solid perseverance of DCF, showed an essentially more noteworthy increment between pre-preparing and post-preparing in the exploratory gathering, contrasted with control group.
DISCUSSION
Neck pain is a constant issue and adds to monetary weight to the general public. Contributing mechanical reason for repetitive neck pain can be aggravation in engine control of the cervical spine which might build the gamble of miniature/full scale injury of cervical structure25.
Limitation of muscle work is hence viewed as crucial for the treatment of cervical spine problem. Diminished actuation of the profound cervical flexors muscle has been noticed straightforwardly and by implication when individuals with neck pain play out the cranio cervical flexion test. Up until this point, there are no investigations contrasting the profound cervical flexor preparing and without biofeedback6.
A comparative report has been led on pressure biofeedback directed profound cervical flexor preparing alongside traditional treatment and regular treatment just in neck pain. Practice including extending of sternoclediod muscle, upper trapezius, levator scapulae, trapezius for 10 redundancies. The review inferred that cervical flexor with biofeedback was successful than the benchmark group. The entomb group examination showed genuinely huge contrast in muscle execution (p=<.001) and pain forces (p=<.004) 17. An investigation of results inside the gatherings was finished utilizing t-test, Wilcoxon marked rank test and the perception of present review were as per the following:
The post aerobic exercise information of DCF perseverance for groupes 1, 2 and 3 were 17%, 4.8%, and 3.6% improvement when contrasted earlier with preparing once more gathering a had a critical extent of progress15.
The post mediation information of NPRS for group 1 uncovers. A comparatively of 58% decrease of manifestation (pain) in group 2 and 55% decrease of side effect (pain) in group 3 were found. The post mediation results of NPRS uncover that group 1 had more prominent extent of progress, when contrasted with other two groups 26.
Concerning a cervical ROM finished up, the post mediation information of gathering 1 had critical 14.6% improvement for group 2 and 3 separately. The result for ROM uncovers a more prominent extent of progress among group 1 patients. The NDI for group 1, post entomb information uncovers a critical 81% decrease of incapacity, when contrasted with preintervention. The NDI for group 2, post mediation information uncovers a critical 57.5% decrease of incapacity, when contrasted with pre intercession. The NDI for group 3, post mediation information uncovers a critical 32.7% decrease of incapacity, when contrasted with pre intercession27.
The investigation of previously mentioned results perhaps induced that the examination of result factors had an improvement for every one of the three review gatherings include Albeit, a general contrast existed between the gatherings. An examination of results between the gatherings was finished utilizing mann-whitney u test.
The post mediation investigation between group 1&2, group 1&3 and gatherings 2&3, shows that there is huge decrease in the pain force of gatherings 1&2 (p=<.004), contrasted with group 2&3 (p=<.944) and group 1&2 (p=<.010) separately. This expresses that the aggravation force between the tension biofeedback directed DCF preparing and just regular treatment was critical (p=.004).
The post mediation investigation between the groups1&3, group 2&3, shows that, there is critical improvement in the cervical flexion (p=<.000) and augmentation (p=.000) in group 1&3, contrasted with group 2&3(p=<.057) (p=<.0.12) and group 1&2 (p=<.005) (p=<.095).
There was critical improvement in DCF perseverance in group1&3(p=<.000) than group 1&2 and groups2&3. The muscle execution of was genuinely huge improvement in pressure biofeedback group than the benchmark group.
The post intercession investigation between the groups1&2, group 1&3 groups2&3, show that, there is critical decrease in the NDI score of gatherings 1&2(p=<.000), and 1&3(p=<.000) and group 2&3 (p=<.018) individually.
Between group investigation of gathering 1 with that of gathering 2 and gathering 3 shows every one of the results factors, for example, pain power, cervical flexion and augmentation ROM, DCF perseverance and neck incapacity file score of gathering 1 displayed to have a serious level of importance than group 2 and 3.
These importance can be contributed the reality basmajian, (1963) expressed that the subject could handle the enrollment as well as the recurrence of release of engine units through hear-able and visual criticism. Adjunctive treatment of tension biofeedback was a compelling method for decreasing pain 17.
Clinical ramifications: The perceptions of present review uncover that, patients having a place with group 1 had a huge clinical and measurable improvement. Henceforth, it could be deduced that for patients with neck pain, the treatment routine ought to incorporate profound cervical flexor preparing with pressure biofeedback. This might achieve a superior clinical result and consequently useful status of neck.
Ethical clearance: There was no risk of conducting this study.Ethical clearance was obtained from the ethical Institutional Review Board of Faculty of Physiotherapy, Dr. MGR. Educational and Research Institute, Chennai with reference No. A26/PHYSIO/IRB/2018-2019 approval letter dated 08/01/2019.
Conflicts of Interest: There is no conflict of interest to conduct this study.
Fund for the study: This is self-funded study.
CONCLUSION
Deep cervical flexor preparing with pressure biofeedback gives better clinical improvement as far as pain, cervical flexion, expansion ROM, DCF perseverance and NDI score.
REFERENCES
1. Clendo J A, child J D, stowell T et al., immediate effects thoracic manipulation in patients with neck pain: a randomized clinical trial. Man ther. 2005 May; 10(2); 127-35.
2. Conley MS, mayor RA, Bloomberg JJ, et al., non-invasive analysis of human neck muscle function. Spinc, 1995, 20; 2505-2512.
3. Ariens GA, bongers PM, Dowes M, et al., Are neck flexion, neck rotation, and sitting at work risk factor for neck pain? Occup environ med, 2001; 58; 200-207.
4. Haldemen S, carrol L, Cassidy JD, et al. Finding from bone and joint decade 2000-2010 task force on neck pain andits associated disorders. J Occup Environ med. 2010; Apr: 52(4); 424-7.
5. Janda V; muscles and motor control in cervicogenic disorder: assessment and management. In: physical therapy of the cervical and thoracic spine. 2nd ed. New York: Churchill Livingstone, 1994; pp. 195-216
6. Jull GA, falla DL et al. Clinical assessment of the deep cervical flexor muscles; the craniocervical flexion test. J manipulative physio ther. 2008 Sep.; 31(7); 525-33.
7. Jhohans blomgren et al., effects of deep cervical flexor training on impaired physiological functions associated functions with chronic neck pain: a systematic review. BMC musculoskeletal disorders 2018, 19:415.
8. Sinho Chung et al. Effects of the cranio cervical flexion and isometric neck exercise compared in patients with neck pain: A randomized controlled trail. Physiotherapy theory and practice, 2018:1-10.
9. Stretching Exercises to Prevent Work-related Musculoskeletal Disorders – A Review Article; Journal of Sports Science & Medicine, May 2017; 5(2):27-37.
10. Mohammed Ali et al. the effects of different exercise programs on size and function of deep cervical flexor muscles in patients with chronic non-specific neck pain: A systematic review of randomized. American journal of physical of physical medicine & rehabilitation, 2017; 96(8); 582-588.
11. Jin young Kim et al., Clinical effects deep cervical muscular activation in patients with chronic neck pain. J. Phys. Ther. Sci. 2016; 28; 269-273.
12. Akbari Asghar et al., investing the effects of stabilization exercise and proprioceptive neuromuscular facilitation exercise on cross-sectional area of deep cervical flexor muscles in patients with chronic non-specific neck pain. International journal of medical research &health science, 2016; 11; 502-508.
13. Amira hussian draz et al., efficacy of deep cervical flexor exercise for neck pain: a randomized controlled study. Turk J phys med rehab., 2016; 62(2); 107-115.
14. Eun young Kim et al., comparison of the effects deep cervical flexor strengthening and Mackenzie neck exercises on head forward postures due to the use of smart phones .Indian journal of science and technology, April 2015; Vol.8(S7); 567-575.
15. Dong yeon kang et al., deep cervical flexor training with a pressure biofeedback unit is an effective method for maintaining neck mobility and muscular endurance in college students with forward head posture. J. Phys. Ther. Sci. 2015; 27; 3207-3210.
16. Zaheen Ahmed iqbal et al., Flexor training using pressure biofeedback on pain and disability of school teachers with neck pain. J. Phys. Ther. Sci. 2013,25; 657-661.
17. Nezamuddin, MD., et al., Efficacy of pressure biofeedback guided deep cervical flexor training on neck pain and muscle performance in visual display terminal operators. Journal of musculoskeletal research. 2013; Vol. 16; No.03; 1350011.
18. Saad Ammar Al-Harbi, et al., compare the effects of deep cervical flexor strength-ening exercises verses electrotherapy modalities on head forward postures resulting from the use of smart phones. World Journal of Pharmacy and Pharmaceutical Sciences, 2013; Volume 6; Issue 6; 266-277.
19. Petri salo et al., neck muscle strength and mobility of the cervical spine as predictors of neck pain: a prospective 6-year study, 2012; Spine 37(12); 1036-1040.
20. Takala ep et al., active neck muscle training in the treatment of chronic neck pain in women: A randomizes controlled trial .jama.2003 may 21; 289(19): 2509-16.
21. Geoffrey R. Williams et al., colony collapse disorder in context. Trends Ecol. 2012; Vol 20; 367-72.
22. Falla et al., the change in deep cervical flexor activity after training is associated with the degree of pain reduction in patients with chronic neck pain. Clin. J. Pain, 2012; 28 (7); 628-634.
23. Aquino RL, et al., applying joint mobilization at different cervical vertebral levels does influence immediate pain reduction in patiets with chronic neck pain. J Man Manip Ther. 2009; 17(2):95-100.
24. Luch E, et al.,
effects of deep cervical flexor training on pressure pain thresholds over
myofacial trigger points in patients with chronic neck pain. J Manipulativ
Physiol Ther. 2013 Nov-Dec; 36(9): 604-11.
| Citation: Kandhasamy. S, Meena.S, Rajesh Kumar.N.T. Impacts of endurance training on deep cervical flexor muscles on neck pain using pressure biofeedback, International Journal of Medical and Exercise Science, March 2022; 8(1); 1188-1198. |
S. M. Divya Mary1, N. Koushik Kumar2, Nelson Arputharaj John3, T. Neelamalar4
Corresponding Author:
1Faculty of Physiotherapy, Dr. MGR Educational & Research Institute, Chennai, Tamil Nadu, India
Mail Id: divyamary.physio@drmgrdu.ac.in
Co-Authors:
2 Faculty of Physiotherapy, Meenakshi academic of Higher education, Chennai, Tamil Nadu, India
3 Departments of Physiotherapy, MAHSA University, Selangor, Malaysia
4Physiotherapist, Fitness Zone, Tambaram, Chennai, Tamil Nadu, India.
| ABSTRACT |
Background of the study: Athletes are exposed to traumatic events that lead to long term psychological and psychosomatic sufferings. After an athlete experience a traumatic event, squeal may include post traumatic stress disorder. In current past year PSTD prevalence was 3.5% among women it was 7.5% and in men it was about 3.6%.
Methodology: A observational study is done with convenient sampling. Post Traumatic Stress Disorder DMS-5 was used as a measurement tool and their psychological and psychosomatic sufferings as an outcome measure. Athletes who have scored more than 5 in questionnaire were divided in two groups. Before starting the study they were assessed with PSTD-DMS5 scale. The subjects were randomly assigned into group A & B. Group A were given behavioural therapy and aerobic exercise includes stepper exercise of 3weeks/session of 30mins/session. Group B were given behavioural therapy with aerobic exercise which includes daily brisk walking of 30 minutes before 8AM. All the 30 participants were made to meet the Psychologist weekly once to receive cognitive behavioral therapy of 12 visits of the whole study duration.
Result: On comparing the pre and post test values of group A and group B on PSTD shows significant difference in the mean values of p≤0.001. Thus it has been proved that stepper aerobics exercise given in groups along with the music has greater significance.
Conclusion: There was improvement in post traumatic stress in athletes of both groups. However stepper aerobics and cognitive behavioural therapy showed more significant improvement than aerobics exercise and cognitive behavioural therapy.
Keywords: Post traumatic stress disorder scale; Aerobic exercise; Cognitive behavioral therapy.
| Received on 24thJanuary 2022, Revised on 18thFebruary 2022, Accepted on 26thFebruary 2022 DOI:10.36678/IJMAES.2022.V08I01.003 |
INTRODUCTION
Post traumatic pressure problem happens in 5-10% of the populace and two times as normal in man as well as in ladies. It is been accounted for that 60.7% in male and 51.2% in ladies would insight something like one expected awful mishap in the course of their life. There are dependably the possibilities of competitors getting harmed while contending or during preparing which is by and large the motivation behind why a clinician would ultimately experience a patient who is a not kidding competitor and is in the need of their help to restore their PSTD.
Competitors might be presented to horrible accidents that can prompt long haul mental and psychosomatic sufferings. After a competitor encounters a horrible accident, spin-off may incorporate post horrendous pressure issue yet in addition different responses particularly culture explicit example of side effect and co morbidities such a pressure and sadness. Post awful pressure problem is portrayed by side effects of re-encountering the awful mishap keeping away from tokens of occasion or feeling genuinely numb and hyper excitement.
Symptom of PSDD adapted from DMS-5: It was officially perceived as a mental issue in the third version of analytic and statistical manual of mental issue (DMS-5). [3,7]
Aerobic exercise stepper exercise: High impact exercise is a type of actual exercise that consolidates with extending and reinforcing preparing schedules determined to work on every one of the components of wellness adaptability, solid strength, and cardio vascular fitness). Step Aerobics is the type of oxygen consuming activity utilizing of a raised stage.
Practicing with a high-impact steps give a few wellness helps that can help in day to day existence. An extreme cardiovascular exercise will make your heart and lungs work all the more productively. The siphoning of the blood from the calf against gravity gives more oxygenated blood to the cerebrum and along these lines it loosens up the brain as well as the entire body.
Role of aerobic exercise:
It improves cholesterols level. Many studies have proved that music with exercise shows positive effects. When music is used before athletic activity, it has been shown to increase the arousal, facilitate relevant imagery and improve the performance of the simple tasks. When music is used during activity, it has ergogenic effects and psychological effects.
Listening to music during exercise can both delay fatigue and lessen the subjective perception of fatigue. It can increase physical capacity, improve energy efficiency, and influence mood. In study after study, the use of muscle during low to moderate level intensity exercise was associated with clear improvements in endurance.
Effects of cognitive behavioural therapy for stress disorder:
The gold standard treatment for PSTD is cognitive behavioural therapy which includes (a) psycho education (b) anxiety management (C) exposure (D) cognitive restructuring.
METHODOLOGY
This observational study was conducted among the athletes by comparative pre and post test type. The 30 subjects were selected at outpatient physiotherapy department, faculty of physiotherapy, DR MGR Educational and research institute. Study duration was 12 weeks (Three sessions per week).
Comparison of Post Traumatic Stress Disorder Dms-5 between Group-A and Group-B in Pre and Post Test


Inclusion criteria were Athletes with post traumatic stress disorder and who are taking medication for stress. Player who scored more than 5 has denoted in trauma screening questionnaire.
Exclusion criteria were any neurological disorder and systemic illness recent surgery and trauma. Stepper, music player, paper pen were the materials used. The subjects were randomly assigned into group A & B. Outcome measures by post traumatic stress disorder scalDMS-5.
Procedure: Athletes who have scored more than 5 in trauma screening questionnaire was grouped into two groups. Group A n=15, Group
Then they were given with PSTD-DMS5 scale. The subjects were randomly assigned into group A & B.
Comparison of Post Traumatic Stress Disorder Dms-5 within Group–A & Group–B between Pre & Post Test Values B n= 15 Before starting the study the whole study was clearly explained to the athletes.


Group A were given behavioural therapy and aerobic exercise includes stepper exercise like stepper Stepper L, step up, step down, grape vine stepper etc., of 3weeks/session of 30mins/session given in the groups along the mild music in groups.
Group B were given behavioural therapy with aerobic exercise which includes daily brisk walking daily of 30 minutes before 8AM.All the 30 participants were made to meet the Psychologist once to cognitive behavioural therapy of 12 vist of the whole study.
RESULTS
On comparing the Mean upsides of Group A and Group B on Post Traumatic Stress Disorder DMS-5, it shows huge difference in the post test Mean qualities however (Group A-Cognitive Therapy with Stepper Aerobics) which has the Lower Mean worth is more successful than (Group B – Cognitive Therapy with Aerobics) P ≤ 0.001.
DISCUSSION
The present study was conducted to determine the effectiveness of cognitive therapy and aerobic exercise in post traumatic stress disorder [PSTD] among athletes. About 50 athletes were selected. They were initially assessed with trauma screening questionnaire. The athletes who scored more than 5 in the questionnaire and athletes who are under medication for PSTD were included in the study. They were randomly selected and at last only 30 participants were selected and remaining 20 were removed from the study due to inconvenient of time, distance and increased stress level. The 30 subjects were grouped into group A [15] and group B [15].
In many studies it has been proved that cognitive behavioural therapy is the gold standard treatment for PSTD. And the beneficial of the regular exercise has a greater impact on psychological makeup which is been provided in the recent studies. The combination of cognitive behavioural therapy and aerobic exercise together plays a major role in bringing back PSTD athletes to the normal.
The statistical reports uncovers that there is no critical distinction in pre test upsides of PSTD[DMS5] score in bunch An and bunch B But there is statically profoundly huge contrast in post test values in PSTD[DMS5] in both gathering An and bunch B.[P≤0.001]. Both the gatherings show critical decline in the post test values Group A is more viable than Group B. This shows the two gatherings are huge in decreasing PSTD in competitors however Group A [Stepper Aerobics and Cognitive Behavioural Therapy] is More Significant When Compared to Group B [Aerobics and Cognitive Behavioural Therapy]. This is no huge distinction in pre test upsides of PSTD [DMS5] score between in Group A and Group B [p≤ 0.001]. Both the gatherings show huge diminishing in post test esteems however Group A is more powerful than bunch B.
Hence, this shows the two gatherings are critical in lessening the PSTD in competitors yet bunch A [Stepper and Cognitive Behavioural Therapy] Is More Significant Than Group B[Aerobics and Cognitive Behavioural Therapy].This is on the grounds that bunch A rehearsed the activity in a gathering and with music. Whenever music is utilized in the any athletic movement it has ergogenic [work enhancing] impacts and mental impact. Standing by listening to the music during activity would both postponement be able to exhaustion and reduces the abstract view of weariness. In bunch practice people had higher aggravation resilience when contrasted with individual exercise performing people.
The increment resistance to agony might come from a more prominent arrival of endorphins-‘the great feel’ chemicals because of individuals in a state of harmony or gathered with each other. Whereas group B also done with morning brisk walk can improve the cardio vascular capacity, improves the mood swing and bring positive vibe, and gives time have significant effect but when compared to group B, group A is more effective because the person is not socially well being and some may be introvert and some may be lazy to wake up in the morning and some will be partial involvement in morning walk.
The cognitive behavioural therapy was most effective on treatment for conditions like anxiety and depression. It is most effective in psychological treatment for moderate and severe depression it is most effective that antidepressants for many types of depression. This is why group A is more effective when compared to group B.
Ethical clearance: Ethical clearance was obtained from the ethical Institutional Review Board of Faculty of Physiotherapy, Dr. MGR. Educational and Research Institute, Chennai with reference No. C53/PHYSIO/IRB/2017-2018 approval letter dated 10/08/2021.
Conflicts of Interest: There is no conflict of interest to conduct this study.
Fund for the study: This is self-funded study.
CONCLUSION
This study shows that there was significant improvement in the post traumatic stress in the athletes in both groups. However stepper aerobics and cognitive behavioural therapy [Group A] showed more significant improve-ement than aerobics exercise and cognitive behavioural therapy (Group B) and reduces the stress level of the athletes and bring back them to the normal.
REFERENCE
| Citation: S. M. Divya Mary, N. Koushik Kumar, Nelson Arputharaj John, T. Neelamalar. Impact of exercise vs cognitive therapy in athletes with chronic fatigue syndrome, International Journal of Medical and Exercise Science, March 2022; 8(1); 1181-1187. |