Vishnupriya.R1, Srividya.G2, Kannan.D3
Corresponding Author:
1PhD Scholar, Annamalai University, Chidambaram, Tamil Nadu and Professor, JKKMMRF College of Physiotherapy, Komarapalayam, Namakkal, Tamil Nadu, India
Mail Id: vpvishnupriyaa114@gmail.com
Co-Authors:
2Research Guide, Department of PMR, Annamalai University, Chidambaram, Tamil Nadu, India
3Professor/Principal, JKKMMRF, College of Physiotherapy, Komarapalayam, Namakkal, Tamil Nadu, India.
| ABSTRACT |
Background of the study: Attention is the behavioural and cognitive process of selectively concentrating on a discrete aspect of information. Difficulty in maintaining attention in the classroom is the main factor for lower grades. However, as an emerging outlook in physiotherapy, engaging the underachievers in structured physical activity will enhance a attention skill. Consequently it will have a tremendous positive impact on children’s academic performance. This study aimed to identify the effect of structured physical activity in improving attention skill among school-going children.
Methodology: The study is an experimental study design and it was conducted among forty Children after obtaining ethical clearance and written consent from the school and parents of these children. All the children were selected based on the selection criteria. All the forty children were randomly allocated into two equal groups. The Children in Group A underwent structured physical activity for 60 minutes per day for three days a week for a period of five months. The children in Group B experienced relaxed indoor activities for 60 minutes and were given three days a week for five months. The pre and post therapy assessment was done using Mindful attention awareness scale (MASS) questionnaire. The SPSS statistical package 26.0 was used to analyze and compare the collected data.
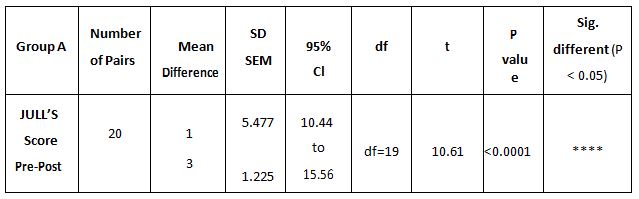
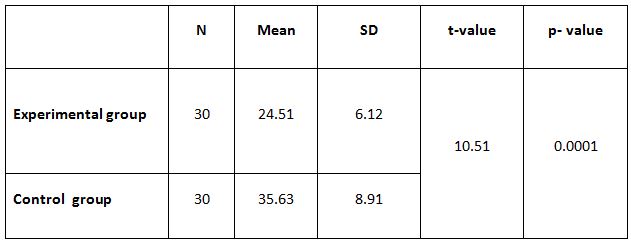
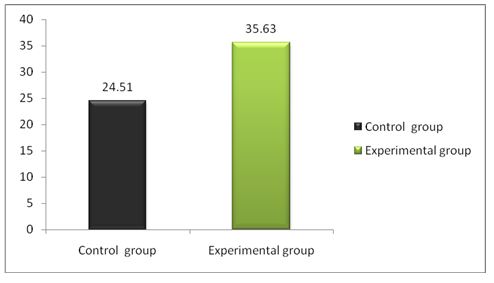
Result: The study result revealed a mean score of 31.68 ± 0.85 for Group A and 14.80 ± 0.87 for Group B with the p-value of 0.0001 which is highly significant.
Conclusion: This study concludes that structured physical activity aids in improving the attention skill of school-going children which in turn improves the academic performance when compared with the children who underwent relaxed in door activities.
Keywords: Attention; MASS; Structured Physical Activity; Relaxed Indoor Activities.
| Received on 24thDecember 2021, Revised on 14thFebruary 2022, Accepted on 25thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.002 |
INTRODUCTION
Attention is the ability to choose and concentrate on relevant stimuli. It is the cognitive process that makes it possible to position ourselves towards relevant stimuli and consequently respond to it. This cognitive ability is very important and is an essential function in students’ daily academic activities1.
In recent pandemic situation there has been a shift in the lifestyles of various age groups including children especially school going children as there was a break in the regular classroom education system of study2. Unlike children a few years ago children now a days are leading increasingly sedentary lifestyle that involves time spent on computer, Television and mobile gadgets.
Effective attention is what allows the children to screen out irrelevant stimulation in order to focus on the information that is important in the moment3. Difficulty with attention will lead to problems like not attending to a academic activity they miss details in instruction4. Children repeatedly make the same mistakes and unable to listen to all the information presented to them.
Prolonged sedentary behavior reduces the attention of the child and reduces the focus on the tasks5. Physical activity in early childhood helps preschoolers establish a healthy lifestyle 6. Various educational objectives propose the physical activity on contribution in mental acuity, skills, and strategies essential for navigating challenges faced across the life span7.
Physical activity (PA) is any bodily movement produced by the muscles which require energy expenditures systematically and safely8.It also includes the motor behaviors such as daily and leisure activities, and it is considered a determinant of life and for general health status 9. Various studies identified that Physical activity facilitates the release of neurotrophic factors, which increases the blood flow to the cerebrum, thereby improving the supply of glucose and lipids to the brain11,12.
The Mindful attention awareness scale is a 15-item scale designed to assess dispositional mindfulness. This scale strongly evaluates the psychometric properties which have been validated. It is unique to measure the consciousness related to predictive of a variety of self-regulation and well-being constructs 13.
Various researches widely acknowledge the physical and mental health benefits of physical activity,14, but there are fewer studies on their effects on cognitive and academic performances and few works were reported on this topic but not on the school children 15, and there is much difference in the exercises prescribed by various researchers and Very few studies have been done in the area of physiotherapy on this perspective. So, this study is aimed to identify the effect of physical activity in improving attention among school-going children.
METHODOLOGY
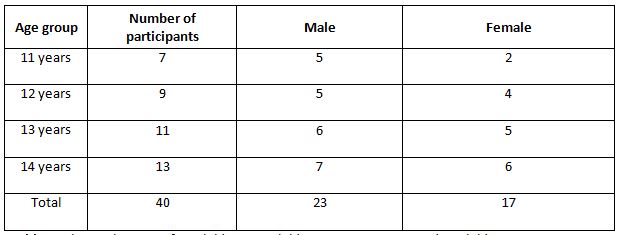
The study was initiated after obtaining ethical approval from the Institutional ethical committee, Annamalai University, Tamil Nadu, India. A pamphlet was created about physical activity and approached the private schools in and around Komarapalayam, Namakkal district, Tamil Nadu. The researcher met the principal and explained the study and around 15 schools were visited only ten school principals agreed to provide samples for the study. Written consent was obtained from the parent of the student who was included for the study prior to the beginning of the study. A meeting with the parent and the class teacher was made and explained the study. Only five schools were taken for this study, and 40 students were randomly selected from each school based on the inclusion criteria. The age group of the participants is 11 years to 14 years of both Genders.
The Children who had good attendance percentage and who were physically healthy with adaptive behavioral skills, were selected for the study. Children who are underachievers in their academic performance and children without any recent infections were also included for the study. Children with orthopedic or neurological disorders, those with injury to the lower limbs, severely obese children, children with psychological disorders, children who are already in sports were excluded from the study.
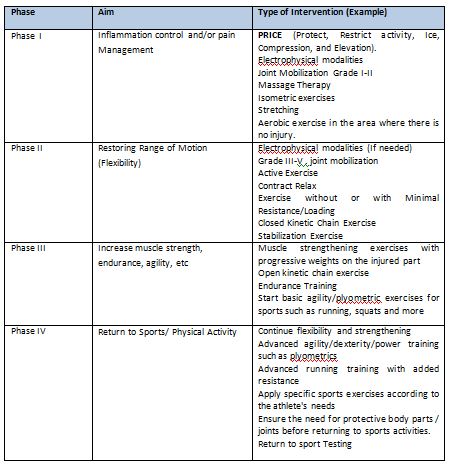
Forty-six children were selected for the study, and they all were divided randomly into two equal groups, twenty-three in each group. Group sampling was done by the computer-generated randomized method. The children in group A underwent structured physical activity for 60 minutes per day over a period of five month and three days per week. Structured physical activity (SPA) taught to the children includes walking with normal speed, walking with maximal speed, slow jogging, slow running, and skipping. Each exercise needs to be done for seven minutes16,17.
Group B underwent relaxed indoor activities (RIA) for 60 minutes per day over a period of 5 months and three days per week. Fifteen minutes were given for warming up exercises, and cool down, activities were also provided. The intensity of the exercises was set at 50%-70% of maximal heart rate 18.
A pre training data was collected using the MASS questionnaire. The post training data was collected by using the MASS Questionnaire at the end of the study (i.e., 5th month). The SPSS statistical package 26.0 was used to analyze and to compare the pre and post training on the impact of physical activity on the attention skill of school going children. The impact of physical activity on the attention skills was analyzed before giving the structured physical activity again the data was collected after 5 months. It was statistically analyzed using SPSS statistical package.
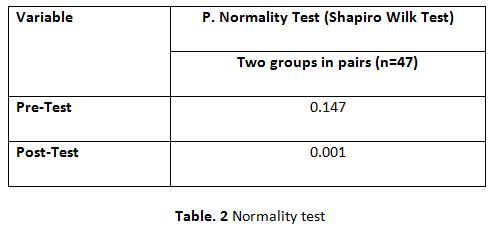
The parametric test was used to determine the level of attention using MASS score. The scores obtained pre-test and post-test values were compared. The obtained p value of 0.05 showed the significant difference between pre and post. Due to illness, three children were not able to attend the part of the study. As a result each groups both groups A and B from the study. As a result, each group had a total of 20 children.
RESULTS
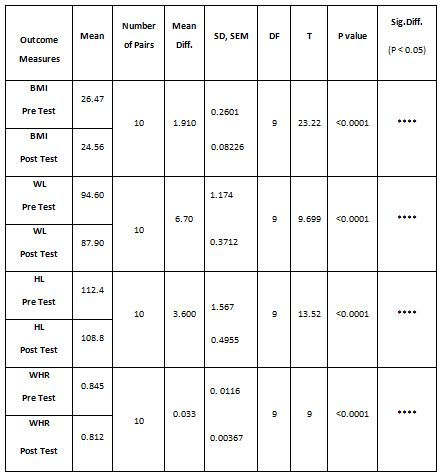
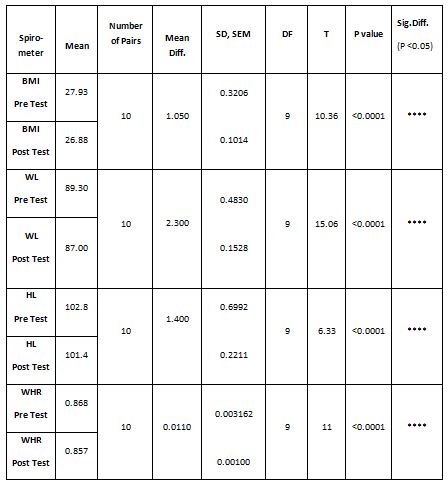
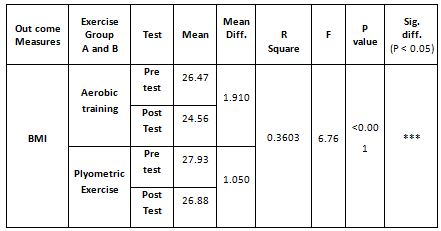
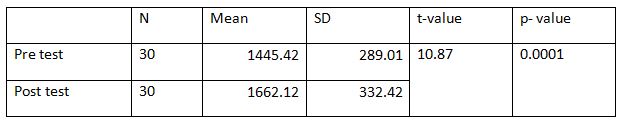
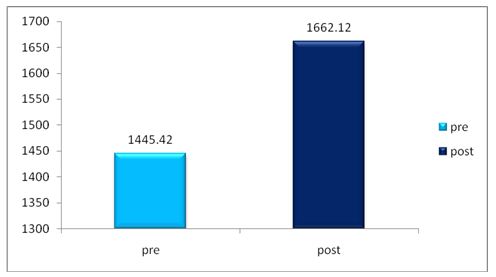
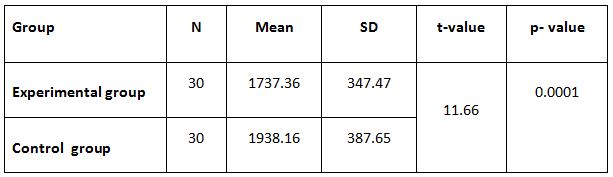
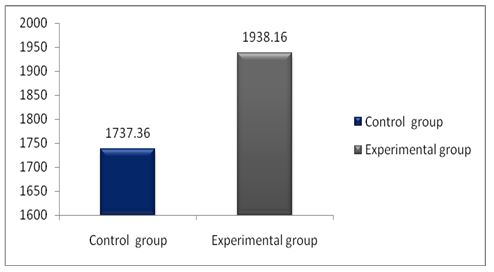
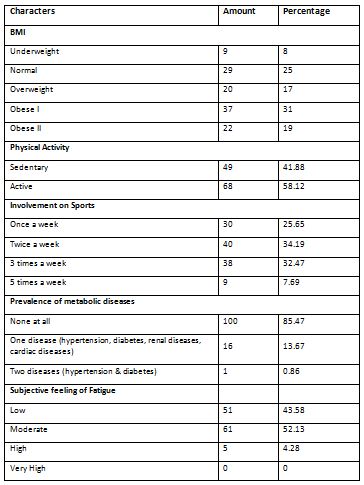
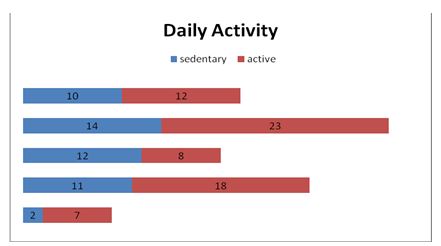
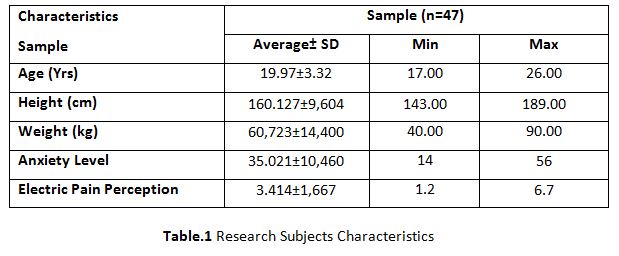
A parametric test is used to analyze the data collected from the children and the data were analyzed using SPSS 26.0. The with-in group analysis is shown in Table II, and the between-group analysis in Table III. The demographical variables are shown in Table I. All of the analysis in the study was done using a critical value of p= 0.05.
Food habits
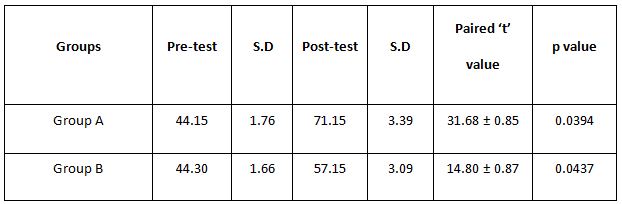
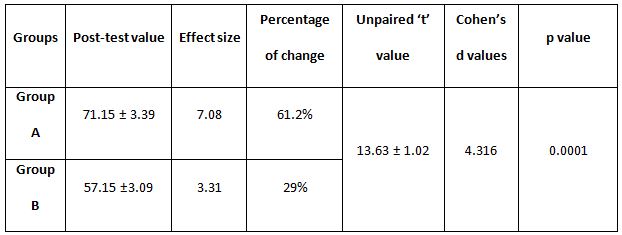
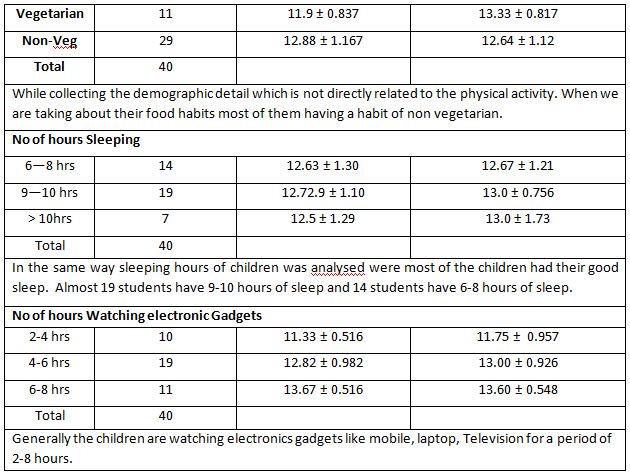
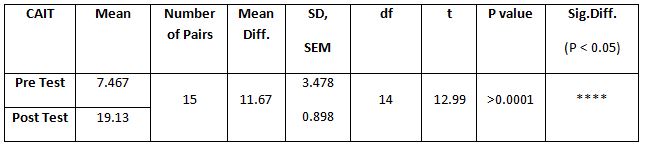
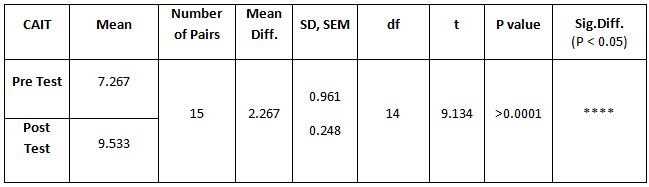
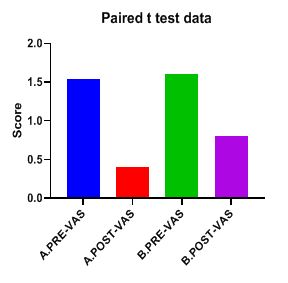
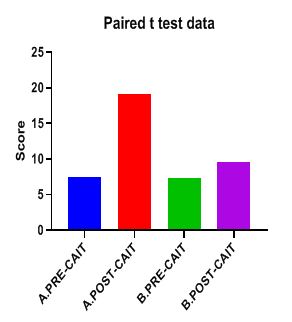
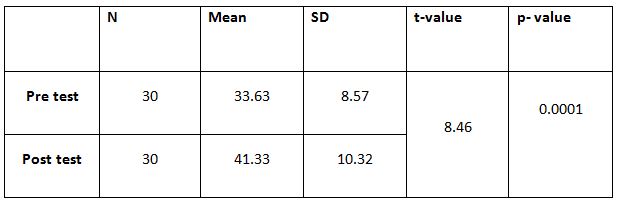
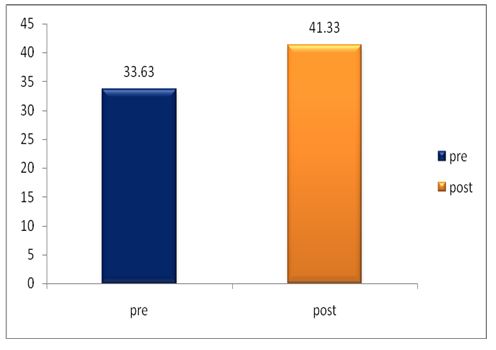
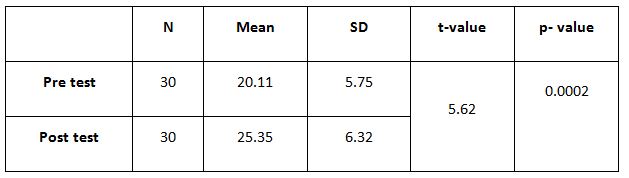
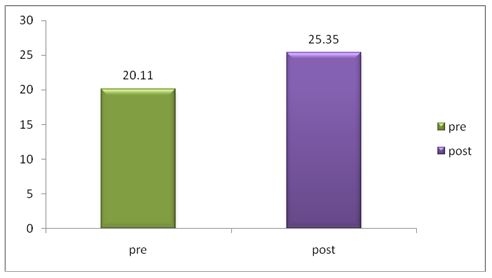
Table 4: Showed the difference between Group A and Group B on analysis of MASS.
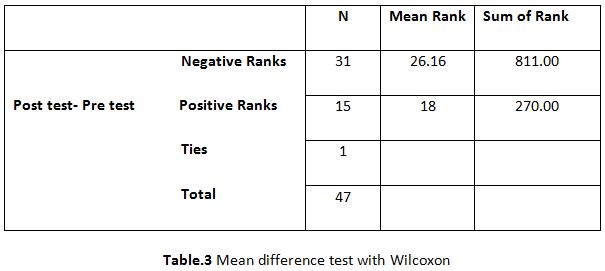
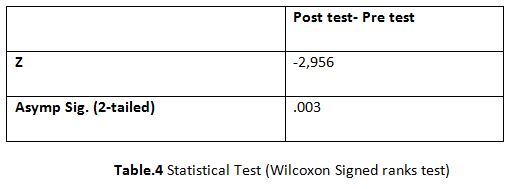
While comparing the pre-intervention and post-intervention data, there is a significant difference obtained between the groups. It was also noted there is a marked increase in attention skills of Group A students.
DISCUSSION
The purpose of the study was to identify the effects of structured physical activity in improving attention skill among school-going children. The problems of attention among the school going children are crucial in its contribution towards learning and academic performances19. School children have trouble having proper attention due to anxiety, frustration, and depression. A prolonged sedentary lifestyle reduces the child’s attention to academic instructions, concentration on the task engagements 20. So, it is mandatory to monitor these children and should give proper attention and training also needs to be given to them to overcome their difficulties 21.
Physical activity (PA) is significant for a child to improve their fitness physically and mentally. It aids in controlling the various psychological symptoms and reduces the risk of developing multiple health issues22. Exercises improve children’s mental health by reducing anxiety, depression, and negative mood by improving self-esteem and cognitive functions23.
Physical activity plays an essential role in improving the child’s moods; the exercises increase circulation to the brain and influence the hypothalamic-pituitary-adrenal axis and reactive to stress24.
Many Studies also identified that acute bouts of aerobic exercises increase cerebral oxygenated blood flow and improve precuneus’ activity 25,26. The Physical activity also enhances Brain-Derived Neurotrophin Factors (BDNF) levels in the blood 27. This improves the activity of the brain and thereby improves the concentration, working memories, and visual-spatial abilities28,29.
A few other studies also supported this study results; Tine and Butler have identified that 12 min single bout aerobic exercises improve attention and concentration in students with the age of 10-13 years30.
A study conducted by Gallotta et al., 2012, identified that the school students involved in aerobic exercises in the physical education sessions showed an improved attention performance than those who didn’t participate31. Above study is supporting the present study.
In a study, Meta-analysis of physical activity and cognitive performances in school-age children showed positive relationship. Several studies have suggested that participation in the PA has a positive relationship with academic performances.
All these findings have suggested that physical activity has a strong influence on academic performances and improvement in the attention of school children. It also plays a significant role in the development of cognitive health.
This study showed a significant improvement in the attention skill of school children who underwent regular physical activity than those who were engaged in non-physical relaxed activity. The improvement in the relaxed activity group may be influence the participant in the research. There are considerable differences obtained within the groups. On comparing the groups, the group who underwent regular PA shows much significant improvement.
This study has identified a few limitations, as selecting the participants and making parents accept to be involved in the study was a monumental task. Home activity or recreational sports activities are not controlled.
As the study duration was higher many students hesitated to participate in the study initially and later, which was liked by them, COVID-19 rules were followed, but the investigation was concluded by using telephone calls to individual parents and direct visits to each child by the researchers.
Ethical Clearance: Ethical clearance has obtained from J.KK. Munirajah Medical Research Foundation, College of Physiotherapy, B. Komarapalayam, Tamil Nadu, to conduct this study with reference number: 001/jkk coptdated 04/06/2019.
Acknowledgment: The authors wish to thank the Principals of Schools, for allowing conducting the study and all the Children and the parents who were involved.
Conflict of Interest: There is no conflict of interest to conduct or publish this study.
Source of Funding: This study is self funded.
CONCLUSION
This study concluded that structured physical activity is better in improving the attention of school-going children. When compare to the relaxed indoor activities.
REFERENCES
- Peretz C, Korczyn AD, Shatil E, Aharonson V, Birnboim S, Giladi N-Computer-Based, Personalized Cognitive Training versus Classical Computer games: A Randomized Double- Blind prospective Trial of cognitive stimulation-Neuroepide-miology 2011; 36: 91-9.
- Sedentary life style; Overview of updated evidence of potential health risks-jung ha park, Ji hyun moon and Yun hwan Oh. 2020 Nov; 41(6): 365–373.
- Plebanek, D. J., & Sloutsky, V. M. Costs of Selective Attention: When Children Notice What Adults Miss. Psychological science, 2017; 28(6), 723–732.
- Cotman CW, Berchtold NC, Christie L-A. Exercise builds brain health: key roles of growth factor cascades and inflammation. Trends Neurosci 2007; 30: 464–72.
- Lowry R., Lee S M., Fulton J E., Kann L. Healthy people 2010 objectives for physical activity, physical education, and television viewing among adolescents: National trends from the youth risk behaviour surveillance system, 1999-2007, Journal of Physical Activity & Health, 2009; 6(1): S36-S45, 2009.
- Gordon E S., Tucker P., Burke S M., Carron AV. Effectiveness of physical activity interventions for preschoolers: A meta-analysis. Research Quarterly for Exercise and Sport. 2013; 84(3):287-294.
- Donnelly J E.,Hillman C H., Castelli D., Etnier J L., Lee S., Tomporowski P., Lambourne K., Szabo-Reed AN. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children: A Systematic Review. Medicine and science in sports and exercise, 2016; 48(6); 1197-1222.
- Mandolesi L., Polverino A., Montuori S., Foti F., Ferraioli G., Sorrentino P., Sorrentino G. Effects of Physical Exercise on Cognitive Functioning and Wellbeing: Biological and Psychological Benefits. Frontiers in psychology. 2018; 9, 509.
- Burkhalter T M., Hillman C H. A narrative review of physical activity, nutrition, and obesity to cognition and scholastic performance across the human lifespan. Adv. Nutr. Int. Rev. J.2011; 2, 201S-206S.
- Robinson A M., Hopkins M E., and Bucci D J. Effects of physical exercise on ADHD-like behavior in male and female adolescent spontaneously hypertensive rats. Dev. Psychobiol. 2011; 53, 383–390.
- Hötting K., Röder B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci. Biobehav. Rev. 2013; 37, 2243–2257.
- Mandolesi L., Gelfo F., Serra L., Montuori S., Polverino A., Curcio G. et al., Environmental factors promoting neural plasticity: insights from animal and human studies. Neural Plast. 2017; 1–10.
- Brown K W. & Ryan R M. The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 2003: 84, 822-848.
- Biddle S J H, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med 2011; 45: 886-95.
- Janssen I, Le Blanc A G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act 2010;7:40
- Bull FC, Al-Ansari SS, Biddle S, Borodulin K, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020 Dec; 54(24):1451-1462.
- Guthold R, Cowan MJ, Autenrieth CS, Kann L, Riley LM. Physical activity and sedentary behaviour among schoolchildren: a 34-country comparison. The Journal of pediatrics. 2010; 157(1); 43-9.e1.
- Subramanian S K., Sharma V K., Aruna-chalam, V., Radhakrishnan, K., Ramam-urthy, S. Effect of Structured and Unstruct-ured Physical Activity Training on Cognitive Functions in Adolescents – A Randomized Control Trial. Journal of clinical and diagnostic research: JCDR, 2015; 9(11); CC04-CC9.
- Lai Y J., Chang KM. Improvement of Attention in Elementary School Students through Fixation Focus Training Activity. International journal of environmental research and public health, 2020; 17(13); 4780.
- Weiyun C, Zhanjia Z, Brooke C, Lexi LC1, Morgan C, Zhonghui H. Acute Effects of Aerobic Physical Activities on Attention and Concentration in School-aged Children. Biomed J Sci & Tech Res.2017; 1(5).
- Sohlberg M.M., Mateer C.A. Effectiveness of an attention-training program. J. Clin. Exp. Neuropsychol. 1987; 9:117-130.
- Centres for Disease Control and Prevention. School Health Guidelines to Promote Healthy Eating and Physical Activity. MMWR. 2011; 60 (No. RR-5).
- Callaghan P. Exercise: a neglected intervention in mental health care? J Psychiatr Ment Health Nurs. 2004; 11;476-483.
- Guszkowska M. Effects of exercise on anxiety, depression and mood [in Polish] Psychiatr Pol. 2004; 38; 611–620
- Widenfalk J, Olson L, Thorén P. Deprived of habitual running, rats downregulate BDNF and TrkB messages in the brain. Neurosci Res. 1999 Aug; 34 (3):125-32.
- Vaynman S, Ying Z, Gomez-Pinilla F. Hippocampal BDNF mediates the efficacy of exercise on synaptic plasticity and cognition. Eur J Neurosci. 2004 Nov; 20(10); 2580-90.
- Ferris LT, Williams JS, Shen CL. The effect of acute exercise on serum brain-derived neurotrophic factor levels and cognitive function. Med Sci Sports Exerc. 2007 Apr; 39(4);728-34.
- Winter B, Breitenstein C, Mooren FC, Voelker K, Fobker M, Lechtermann A, Krueger K, Fromme A, Korsukewitz C, Floel A, Knecht S. High impact running improves learning. Neurobiol Learn Mem. 2007 May; 87(4); 597-609.
- Hillman CH, Erickson KI, Kramer AF. Be smart, exercise your heart: exercise effects on brain and cognition. Nat Rev Neurosci. 2008 Jan; 9(1); 58-65.
- Tine M T., & Butler AG. Acute aerobic exercise impacts selective attention: An exceptional boost in lower-income children. Educational Psychology, 2012; 32; 821-834.
- Gallotta MC, Guidetti L, Franciosi E, Emerenziani GP, Bonavolontà V, Baldari C. Effects of varying type of exertion on children’s attention capacity. Med Sci Sports Exerc. 2012 Mar; 44(3); 550-5.
| Citation: Vishnupriya R, Srividya G, Kannan D. Effects of structured physical activity in improving attention among school going children, International Journal of Medical and Exercise Science, March 2022; 8(1); 1172-1180. |