Kavya Sree.P.P1, Saji.V.T2
Corresponding Author:
1MPT Student, Cooperative Institute of Health Sciences,Thalassery, Kerala, India, Email id: kamalakshanppp@gmail.com
Co-Author:
2Principal and Professor, Cooperative Institute of Health Sciences, Thalassery, Kerala, India
ABSTRACT
Background: In the female population, stress urinary incontinence (SUI) is a disorder in which elevated abdominal pressure caused by coughing, laughing, sneezing, or exercising results in accidental urine leakage. Women exercise in more significant numbers and learns about the cardiovascular and musculoskeletal advantages of regular physical activity.
Method: This is a Cross-sectional survey done at Ladies Fitness Centers Kannur and Kozhikode Districts in Kerala. Five hundred young women were selected who fulfils the inclusion and exclusion criteria by simple random sampling. The participant’s height and weight were measured to calculate BMI. The participants were given two questionnaires, ICIQ- SF (International Consultation on Incontinence Questionnaire-Short Form), which contains four primary items that require participants to rate their symptoms over the previous four weeks. The first two items are demographic, while the final one is self-diagnostic. The QUID (the questionnaire for urinary incontinence diagnosis) is the questionnaire in which six questions regarding urinary incontinence in which three items consist of stress urinary incontinenceand the remaining three items consist of urge incontinence symptoms. Both questionnaires were given to each participant and recorded.
Result: This study enrolled 500 young women with an average age of 22.77. 37.2% of the young women attending the gym had SUI while doing high-impact workouts.
Conclusion: The study reported that there is a risk of stress urinary incontinence during high impact exercises in young women. Both married and unmarried young women experienced leakage during high impact exercises. The finding suggests that continuous high-impact exercise may result in chronic mechanical stress of the pelvic floor.
Keywords: High impact exercises; Stress urinary incontinence; ICIQ-SF score; QUID score.
Received on 27th July 2021, Revised on 12th August 2021, Accepted on 28th August 2021, DOI:10.36678/IJMAES.2021.V07I03.006
INTRODUCTION
Urinary incontinence (UI) is defined by the World Health Organization (WHO) and the International Continence Society (ICS) as an unintentional flow of urine via the urethra, and it is regarded as a concern for one’s health, social well-being, and hygiene. Urinary incontinence can be classified into three categories, according to the standardization steering committee (SSC). Stress urinary incontinence(SUI) or effort urinary incont-inence, urge urinary incontinence (UUI), and mixed urinary incontinence are the three types of incontinence (MUI)1.
The urgency urinary incontinence (UUI), it is described as the uncontrolled loss of urine that occurs in response to a sense of urgency, there are two other clinical presentations to consider: mixed urinary incontinence (MUI), which is described as a relationship between urgency and leaking during physical exertion and SUI, which is characterized as any symptom of uncontrolled loss of urine that occurs following physical efforts, such as sneezing and coughing, or during any other stressful situation2.
Among these types of incontinence, SUIis the most common, with prevalence rates ranging from 10% to 55% in women aged 15 to 64 years.3The significant risk factors can be classified as predisposing factors, such as family history, supporting factors, such as sports participation, and aggravating factors, such as obesity and natural delivery with neuromuscular impairment. In this scenario, women who engage in physical activity, particularly impact sports, have a higher prevalence of urine incontinence. According to a study, 47% of women who regularly exercise may suffer from urine leakage. Numerous individuals link this issue to pregnancy and childbirth. However, 25–28% of non-pregnant high school and collegiate athletes develop stress urine incontinence4.
These percentages are even more remarkable in athletics that dramatically increase intra-pelvic pressure, such as gymnastics and trampoline, where between 60% and 80% of players report incontinence.”The proportion of urinary leakage in the different sports was gymnastic 56%, ballet 43%, aerobics 40%, badminton 31%, volleyball 30% athletics 25%, handball 21% and basketball 17%.”5Jumping was the most probable action to result in leakage. The majority of the time, SUI is the result of a malfunctioning pelvic floor. Urine leakage is a widespread issue, even among young females, and irrespective of age, between 15% and 30% of women have negative consequences from urinary incont-inence in all sectors of life, and including a decline in life quality. SUI affects one in every three women at some point in their lives and is more prevalent in parous women than in nulliparous women6,7.
Urinary incontinence is resulted by a complicated synchronization of the bladder, urethra, pelvic floor muscles, and ligaments, which occurs most frequently during activity when abdominal pressure increases.The magnitude and duration of high-impact, frequent exercise may contribute to pelvic floor muscle fatigue and, as a result, incontinence. Raises in intra-abdominal pressure are evenly transferred to the bladder, bladder base, and urethra in an optimally supported urogenital tract. Increased downward direct pressure caused by coughing, laughing, sneezing, and Valsalva manoeuvreis balanced incontinent women by ancillary tissue tone produced by the levator ani muscle and vaginal connective tissue. However, when descending forces are not resisted in those with a compromised supporting “backboard, “funnelling of the ureterovesical junction occurs, resulting in an open urethra and subsequent urine leakage 8,9,10.
High impact activities are those that need both feet to leave the ground simultaneously, such as sprinting, jumping jacks, plyometrics, some stepping aerobics, and some cardio dancing that requires hopping. These activities should be kept for those who already have a basic level of fitness and are at minimal risk of developing joint problems, as they carry a significant risk of damage, particularly to the ankle, knee, and hip joints, and also the spine.Fit and active women are more prone to experience SUI. Numerous researches have demonstrated that activities requiringmuch physical exertion andhigh impact exercise can significantly increaseintra-abdominal pressure. It may overburden the pelvic organs, resulting in injury to the muscles that brace these organs. Within this setting, exercise becomes a contributor to the progression of urinary incontinence in women, particularly those without a history of childbirth or pregnancy11,12.
Regular exercise was already recommended to people of any age for its health benefits and as a means of compensating for an ina-ctive lifestyle that can develop obesity, muscle weakness, and postural difficulties. Men and women work out at gyms with this goal in mind, oblivious to the fact that when performing the activities, the peripheral and interior muscles are involved and may be harmed if the activities are performed inappropriately. At some stage of life, all women will have stress urinary incontinence. Unfortunately, many of them “live with” the problem, either because they are too ashamed to ask for help or because they believe it is a “natural” aspect of ageing and having children13,14.
There has been little research on the influence of high-impact workout on the female lower urinary system. The more effective treatment for SUI is surgery. In women and individuals with minor symptoms, conservative treatment is now suggested as the first line of defence. Conventional non-surgical treatmentsinclude lifestyle changes, bladder strengthening and conditioning, pelvic floor muscle workout, biofeedback, and activating pelvic floor by applying a small voltage.
Kegel workouts are the most common approach toreinforcing the pelvic floor muscles because they are non-invasive and do not require vaginal weights or cones. Arnold Kegel, an American gynaecologist, characterised them for the first time in 1948. They seem to be the most cost-efficient treatment option and are distinguished from other therapies because they may be performed independently by the patient at any time and location while performing other tasks without requiring regular hospital trips. Simply instructing the patient on how to tense their pelvic floor muscles is all that is required. Kegel exercise consistently strengthens the pelvic floor, according to the majority of studies15.
By conducting the survey,it tries to find out the prevalence of SUI in young women who participate in high impact exercises at the gym in Kannur and Kozhikode districts in Kerala and also give awareness to the public regarding the significance of pelvic floor strengthening exercises and the relevance of the same in having healthy adultlife.
MATERIALS AND METHODOLOGY
Five hundred young women were selected by the proper screening and fulfilling the inclusive criteria: a) Young women aged 20-25 years, b) Young women who satisfied specific questionnaire criteria about the type of activity in the gym, c) Healthy and sexually active women, d) Willingness to participate, e) Young women who attend gym and exclusion criteria f) Handicapped young women, g) Surgical treatment for gynaecological and urological illness, h) Infection of the urinary tract, i) Diabetics Mellitus, j) Respiratory disease, k) Incomplete questionnaire, l) Refusal to take part in the research, m) BMI above 30, n) Combination of multiplesports.
Before the study, the purpose and procedure were explained to the participants, and their consent wasobtained. The participant’s height and weight were measured to calculate BMI. The 500 participants who performed high impact exercises were given two questionnaires.The “ICIQ-SF (International Consultation on Incontinence Questionnaire-Short Form)” questionnaire contains four primary items in which respondents are asked to rate their symptoms during the previous four weeks. The first two items are demographic, while the final one is self-diagnostic. The QUID (the questionnaire for urinary incontinence diagnosis) has six questions regarding urinary incontinence, in which three items consist of SUI and the remaining three items consist of urge incontinence symptoms. Both questionnaires were given to each participantand recorded.
RESULT
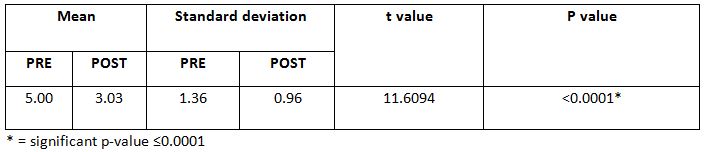
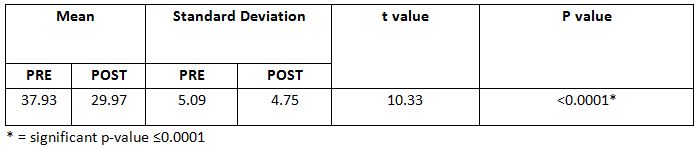
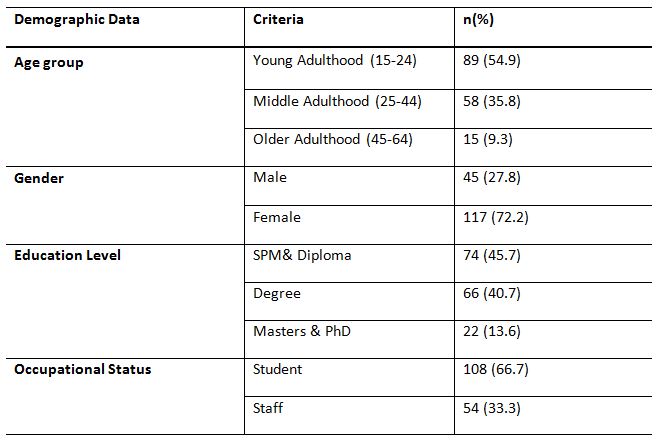
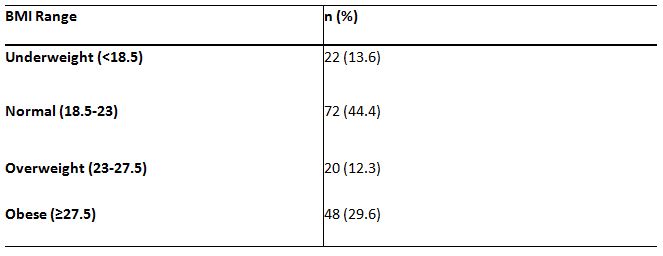
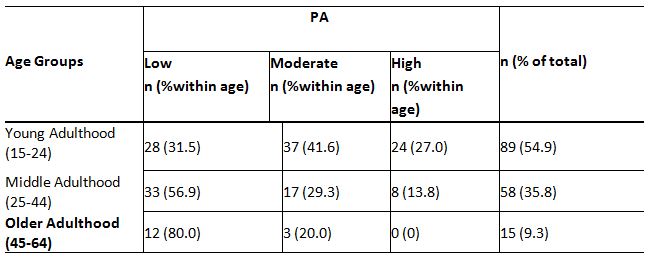
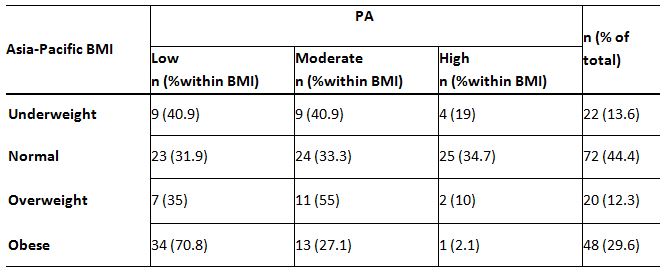
This study enrolled 500 young women with an average age of 22.77.37.2% of the young women attending the gym had stress urinary incontinence while doing high-impact exercises. The majority of the young women having SUI were in the overweight category. The p-value is less than 0.001. In the QUID score, the relation between age and SUI is positive. The SUI is seen to increase with age. However, since the p-value is greater than 0.05, the coefficient is not statistically significant, and the relation between BMI and SUIis positive.
The SUI is seen increasing with BMI. Since the p-value is less than 0.001, the coefficient is statistically significant. According to the ICIQ SF score, the relationship between age and SUI is positive, and the SUI also increases with age. However, since the p-value is greater than 0.05, the coefficient is not statistically significant, and the relation between BMI and SUIis positive. The SUIis seen increasing with BMI. However, the p-value is greater than 0.05; the coefficient is not statistically significant.
DISCUSSION
The research aimed to determine SUI prevalence in young women who go to the gym and participate in high-impact workouts. “According to the World Health Organization (WHO) and the International Continence Society (ICS), urinary incontinence is defined as the involuntary flow of urine via the urethra and is a cause for concern on health, social, and hygiene reasons”.SUI, UUI, and MUI are the three primary kinds of urine incontinence. In a nutshell, SUI is defined as the loss of urine due tohigh intra-abdominal pressure and rise in intravesical pressure beyond the urethral closure limit. This scenario can arise as a result of coughing, sneezing, or jumping. Urinary incontinence is more frequently diagnosed in women than males, and it was anticipated to impact almost 420 million individuals globally in 2018. According to recent data, women have urinary incontinence twice as frequently as males. This condition affects approximately 20-30% of young women, 30-40% of women in middle age, and up to 50% of old aged women.
High impact activities are those that require both feet to leave the ground simultaneously, such as sprinting, jumping jacks, plyometrics, some step aerobics, and some cardio dancing that incorporates leaping. These types of exercise should be confined to individuals who already have a baseline level of fitness and are not at risk of developing joint problems, as they increase the risk of damage, particularly to the ankle, knee, and hip joints, as well as the spine11. Numerous women incorporate recreational physical activity into their daily routines in order to ensure a healthy lifestyle. Physical activity has long been known to benefit blood pressure, weight loss, diabetes, and hyper cholesterolemia. Men and women work out at gyms with this goal in mind, paying little attention to how they are doing so. The impact of physical activity on normal physiology of bladder, on the other hand, is not well recognized.
According to Celina Fozzati c, this occurs on physical workout when the intra-abdominal pressure varies. Pelvic floor muscle activity can be harmed by injury, and their malfunction is one of the determinants of the evolution of SUI in adult females.16High impact activities have been known to rupture the endopelvic fascia or the arch tendinous insertion of the pelvic floor muscles. Another possibility is that alterations in the spine’s physiological curvature result in postural changes and modification of the pelvic cavity’s anatomy due to stretch or compression injury to the pelvic floor muscle.
In this study, 500 young women are selected from the various female fitness centres in Kannur and Kozhikode districts in Kerala based on inclusion and exclusion criteria. A validated “ICIQ-SF questionnaire (International Consult-ation on Incontinence Questionnaire-Short Form)” and “QUID (the Questionnaire for Urinary Incontinence Diagnosis)” questionnaire was used for this study. ICIQ SF questionnaire,has four major sections that ask for a rating of symptoms during the previous four weeks. Items 1 and 2 are demographic, and the final item is self-diagnostic.
The QUID is the questionnaire in which six questions regarding urinary incontinence in which three items consist of SUIand the remaining three consist of urge incontinence symptoms. All the subjects were given and explained the questionnaire. From the questionnaire outcome, we obtained the incidence of SUIin young women who perform high impact exercises atthe gym.
SUI develops when a weakened urethral sphincter cannot withstand the discharge of urine from the bladder during instances of increasing intra-abdominal pressure. “The respective elements affect to urethral continence maintenance: passive urethral closure and coaptation, a critical urethral length, maintenance of the bladder muscle and proximal urethra in their normal anatomic positions, and adaptive changes to the urethra during periods of increased intra-abdominal pressure17.
According to Kari BO, high-impact physical activity increases intra-abdominal pressure. Suppose the muscles of lower pelvic region are unable to co-contract rapidly andsufficiently powerfully to resist this immense pressure or endure the ground compressive force, the levator hiatus may widen, extending and weakening the muscles and increasing the risk of urinary incontinence18.
Epidemiological research on urine incontinence indicates that the disorder is two to three times more prevalent in women. Thus, urinary incontinence can be considered a specific aspect of ageing when it is not reported in women of all ages, cultures, and races, contrary to popular belief that it is more prevalent in the old population, creating a global problem.
According to Hannestad, the frequency grows steadily with age, reaching a significant high in middle age and continuing to rise continuously after age 65. The kind of incontinence may vary with age; some research indicates that SUI is more prevalent in women under the age of 60. According to the survey, the majority of cases were documented among young women under the age of 25. High BMI is a substantial and unique risk factor for SUI, according to Navneet margon10.Evidence suggests that both desire and SUI prevalence increase proportionately with BMI. Thus, a rise in intraabdominal pressure associated with higher BMI results in a correspondingly increased intravesical pressure, which overcomes urethral closure pressure and results in incontinence.
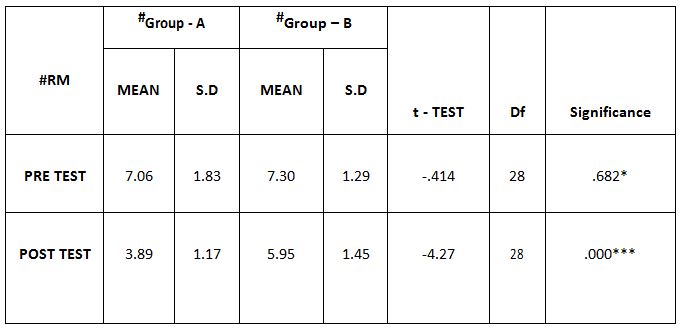
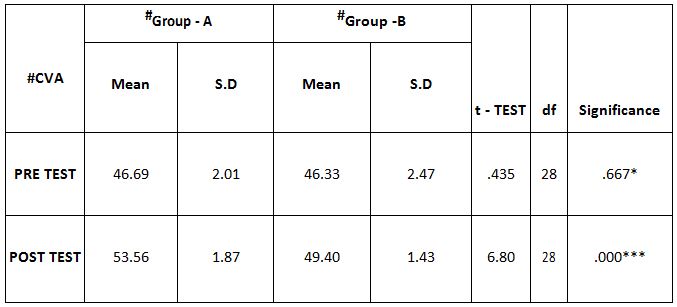
In this study, 37.2% of the young women attending the gym had stress urinary incontinence. According to QUID and ICIQ – SF scoring, the relation between age and stress incontinence is positive. The SUI is seen to increase with age. Nevertheless, since the p-valueis greater than 0.05, the coefficient is not statistically significant. The relation between BMI and SUI is positive.
According to ICIQ –SF score SUI seen in increasing with BMI, the p-value is greater than 0.05; the coefficient is not statistically significant. But in the QUID score, SUI increase with BMI. Since the p-value is less than 0.001, the coefficient is statistically significant.
Ethical Approval: Ethical clearance has been obtained from the Ethical Committee of Cooperative Institute of Health Sciences, with reference number: 01/2018/MPT Musculo-skeletal & Sports/CIHS, dated: 12/04/2019, Kozhikode, Kerala.
Conflicts of Interest: No conflict of interest to conduct and publish this article was reported throughout the study.
Fund for the Study: This study is self-funded.
Limitations: The study was conducted in a small sample size. All the data were collected subjectively, which may introduce an error that treats the study’s reliability. No pilot study was conducted.
CONCLUSION
The study concluded that SUI is a potential danger in young women who engage in high-impact workouts. Both married and unmarried young women reported experiencing leakage throughout high-impact activities.
The study’s findings will assist young women to engage in high-impact activities to strengthen their pelvic floor muscles and prevent stress urine incontinence.
REFERENCES
- Magdelena Weber-Rajek, Agnieszka strac-zynska. Assessment of the effectiveness of pelvic floor muscle training (PFMT) and extracorporeal magnetic innervation (ExMI) in treatment of stress urinary incontinence in women: A Randomized Controlled Trial. Biomed Res Int. 2020 Jan 16; 2020; 1019872.
- SoralaTonon Da Luz. Urinary incontinence in physically active young women: preva-lence and related risk factors. Int J Spors Med2017; 38; 937-941.
- AratiMahishale, Rafat Khalid Hussain Jamadar. Research Article screening of urinary incontinence in female dancers- A cross sectional study. Research Journal of Obstetrics and Gynecology ISSN 1994-7925 DOI: 10.3923/rjog. 2018;31;35.
- Ellen Casey MD. stress urinary incontinence in the female athletes. July 9; 2015.
- H. H.Thyssen, L. Clevin,S. Olesen. Urinary incontinence in elite female athletes and dancers. Int Urogynecol J. 2002; 13; 15-17
- Magdalena Hagovska, Jan Svihra. Prevalence of urinary incontinence in female performing high impact exercises. Int J Sports Med. 2017; 38; 210-216.
- Aletha Silva Caetano, Maria de Consolacao Gomes Cunha. Urinary incontinence and physical activity practice. Esporte Niteroi July/Aug2007; Vol. 13; No 4; pp 245e-248e.
- Jodie G. Dakic, Jill Cook, Jean Hay-Smith Pelvic floor disorders stop women exercising: A survey of 4556 symptomatic women. Journal of Science and Medicine in Sport. June 2021; S1440-2440(21)00147-X.
- Aletha Silva Caetano, Maria de Consolacao Gomes Cunha. Urinary incontinence and physical activity practice.Esporte,Niteroi July/Aug 2007; Vol.13 no 4.
- Navaneet Margon, Bharati karla. stress urinary incontinence what, when, why and then what. Journal of mid life health, Jul- Dec 2011; Volume 12.
- Carls C. The prevalence of stress urinary incontinence in high school and college-age female athletes in the midwest: implications for education and prevention. Urol Nurs. 2007 Feb; 27 (1); 21-24.
- Jyoti S Mandge, ArmaityDehmubed. Study of urinary incontinence affecting quality of life and health seeking behavior in women of an urban slum in Mumbai. Int J community Med Public Health. 2019 Jan; 6(1); 290-292.
- Orly Goldstick, Naam Constantini . Urinary incontinace in physically active women and female athletes. BJSM online First, published on May 18, 2013 as 10.1136/ bjsports-2012-091880.
- Beta Stach-Lempinen, Clas-HakanNygrad. Is physical activity influenced by urinary incontinence. BJOG: an International Journal of Obstetrics and Gynecology May 2004, Vol.111; pp.475-480.
- Seong Hi Park, Chang Bum Kang. Effect of kegel exercise on the management of female stress urinary incontinence. A systemic review of Randomized controlled trials.volume 2014/Article ID640262.
- Celina Fozzatti. Prevalence study of stress urinary incontinence in women who perform high impact exercises. Int Urogynecol J., 2012; 23(12); 1687-1691.
- Rovner, E. S., & Wein, A. J. (2004). Treatment options for stress urinary inco-ntinence. Reviews in urology, 6; Suppl 3; S29–S47.
- Kari. BO .Is physical activity good or bad for the female pelvic floor?. A narrative review. Sports medicine. (2020). 50; 471-484.
| Citation: Kavya Sree.P.P, Saji.V.T(2021). A survey on the effect of high impact exercises on stress urinary incontinence in young women, ijmaes; 7 (3); 1080-1087. |