Back ground: Back pain is common among health workers especially patient’s caregivers in Spinal Cord Injury group. Objectives of the study were to estimate the prevalence of low back pain among the caregivers of adults with spinal cord injury. Care givers of all the spinal cord injured individuals who seeks for rehabilitation in the department of PMR were eligible to participate in the study.
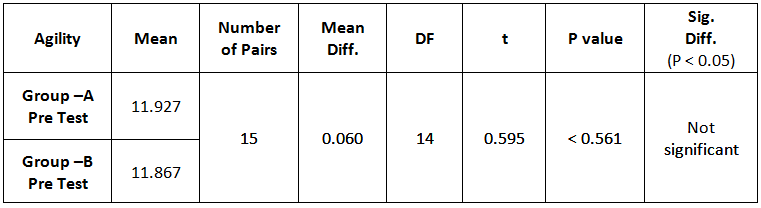
Methodology: This was an observational study with a cross-sectional study design. After receiving the consent, the participants were asked to fill the questionnaire. First part of the questionnaire consists of demographical data of the patients and their caregivers. If the caregiver was reporting LBP, then they were asked to grade their pain intensity through Visual Analogue scale and also to fill Oswestry Disability Index (ODI) to identify the disability caused by the LBP. These data were used to find the prevalence of LBP among caregivers and also to find relationship with various demographical variables.
Results: One hundred patients and their caregivers’ data collected and analyzed. Out of these 20 where drop outs and samples female (42) caregivers reported that they have low back pain. In that 16 caregivers were males and 26 were females. There was no statistically significant difference between the patients and caregivers of the LBA group and no pain group in the demographic data except the duration of injury.
Conclusion: This study aimed to find out the prevalence and characteristics of low back ache of caregivers of the adult with low back pain. Study revealed 51.9% prevalence of low back pain among the SCI caregivers.
Key words: Low back pain, Caregiver, Spinal cord injury
Received on 11th September 2020, Revised on 12th October 2020, Accepted on 10th November 2020 DOI:10.36678/IJMAES.2020.V06I04.001
INTRODUCTION
Low back pain (LBP) is a common problem
affecting most of the adults’ population at some point during their lifetime,
especially in low and middle income countries 1, 2. In a report of the World Health Organization
(WHO) in 2003, it was found that about 80% of people have LBP at some time in
their life 3. Quality of life, burden, satisfaction, and depression
of caregivers have been extensively studied. Back pain is the most frequent
cause of activity limitation in people below 45 years according to (NIH)
guidelines4.
Risk factors associated with LBP in the
workplace have also been studied, particularly in occupations such as nursing,
industrial work, police service, and fire service 5, 6. Lifting
heavy objects, inappropriate lifting techniques and poor fitness levels are
risk factors among nurses, whereas heavy physical activity, frequent bending
and lifting, repetitive movements, being exposed to vibration, and depression
are significant risk factors among industrial workers 7-10.
After the Traumatic or Non- Traumatic
injury the individual becomes spinal cord injury there is of the need for
assistance in their daily living activities. This might be assistance in feeding,
bathing dressing shifting to uneven surfaces or even surfaces toileting or
dressing. Today with the change in health care, we see more family members as
the source of care support more than 40% of spinal cord injured individuals use
some assistance or the other with their family members females are more likely
to have a paid attendant as caregiver, while male have their parent assist.
Manual patients transfer tasks between
bed wheel chair and bath cart, perceived physical exertion were consistently
associated with different measure of LBP. The symptoms of low back pain are
notice with flexion of the back, and when lifting the heavy objects. Patients
handling was found to be an extremely hazardous job that had substantial risk
of causing a low back injury whether with one or two patient handlers.
Prevalence of LBP was significantly higher among caregivers (58%) compared with
age- and BMI-matched controls (27.6%). The prevalence of LBP was also higher
among caregivers of SCI patients with long duration of injury; i.e. LBP was
associated with care-giving duration11.
Objectives of the study: Objectives of the study were to know the prevalence of low back pain among the
caregivers of adults with spinal cord injury and to find the disability caused
by low back pain in caregivers of adults with spinal cord injury.
METHODOLOGY
Care givers of all the spinal cord
injured individuals who seeks for rehabilitation in the department of PMR are eligible to
participate in the study. After receiving the consent, the participants were
asked to fill the questionnaire. First part of the questionnaire consists of
demographical data of the patients and caregivers. If the caregiver is
reporting LBP, then they will be asked to grade their pain intensity through
Visual Analogue scale and also to fill Oswestry Disability Index (ODI) to
identify the disability caused by the LBP.
This study
design was observational study and the study setting done at Urban and rural population around the outskirts of
Bangalore. 100 subjects were taken for the study and Simple Random Sampling
method used to allocate the subjects in different group. Subjects aged between
25 to 50 years of both sexes from urban and rural areas of Bangalore. The study
conducted for duration of 10 months.
Selection criteria
Inclusion Criteria: age-
25-50yrs, both male and female subjects, Subjects with spinal cord injury, subjects
with six months post injury, subjects attending for more than 4 hours.
Exclusion Criteria: Previous
history of back pain irrelevant to care –giving, Caregivers who have history of
back surgery, Caregivers who have a history of back fracture, Caregivers with
physical disability
Outcome Measure: Demographic variables, Pain, Neck Function
Measurement
Tools: Demographic
Questionnaire, Oswestry Disability Index–short form
(ODI) and VAS scales.
Procedure for Intervention: As the questionnaire is being filled and returned by the subjects, the data were analyzed to find outcome and significant differences in assessment of risk of low back pain in caregivers with spinal cord injury patients.
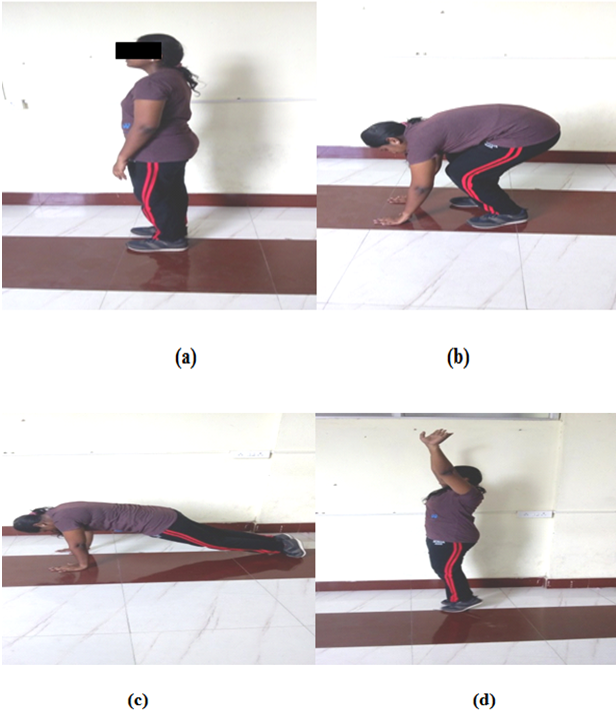
Figure1. Assessment of ODI Scale with Patient
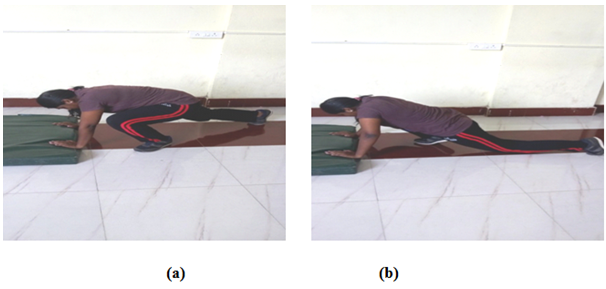
Figure2. Transferring Techniques for
Caregivers
RESULT
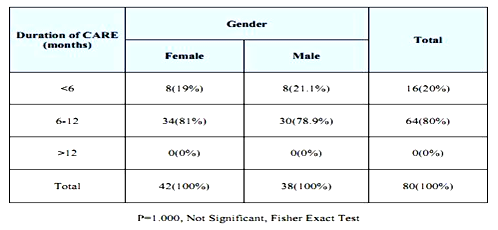
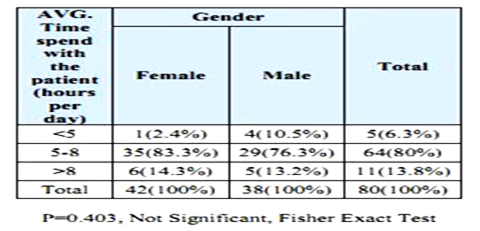
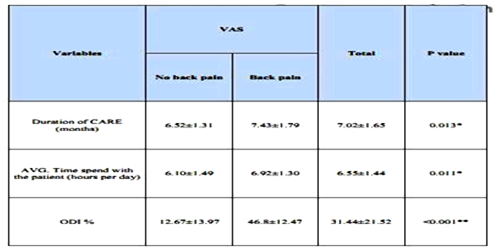
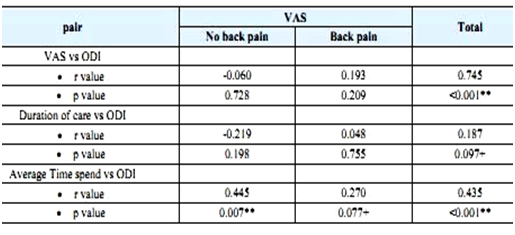
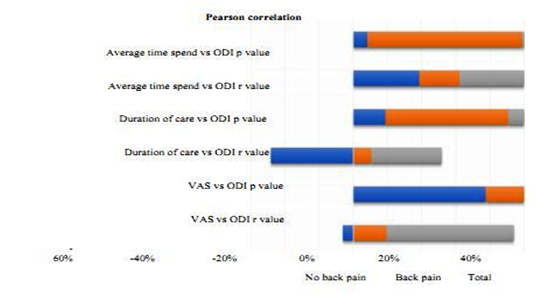
Table1:Demographicdataofgenders Table2: Duration of care in relation to gender Table3: Average time spend with patient according to gender Table4: Duration of care and average time spend on patient with neck and back pain Table5: Duration of care and average time spend with patient in relation to VAS and ODI Graph: 1 Graphical representation of duration of care and average time spend with patient in relation to VAS and ODI
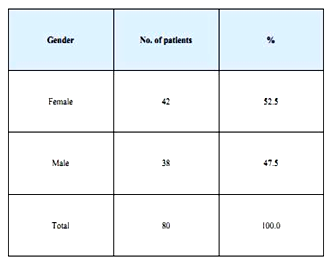
One hundred patients and their
caregivers’ data collected and analyzed. Out of these 20 where drop outs and
samples female (42) caregivers reported that they have low back pain. In that
16 caregivers were males and 26 were females. There was no statistically
significant difference between the patients and caregivers of the LBA group and
no pain group in the demographic data except the duration of injury.
DISCUSSION
In the present study,
prevalence of LBA was found to be 51.9%. Our results are similar to the study
reported by Barak et al among Turkies people and they reported 54%.
The prevalence was also
higher among the caregivers of SCI patients with long duration injury; i.e. LBA
was associated with care giving duration. This was attributed to activities
that cause LBA having carried out for long time. ASIA impairment scale was used
to evaluate the patient’s level of injury and the assistance of caregivers
required in their mobility LBA 12.
SCIM scores were not
associated with caregivers’ LBA. As
there are no mechanical devices available in India to transfer a patient,
manual handling is common. The availability of man power in a home set up also
an issue. A high frequency of LBA among caregivers with low ASIA score was thus
an expected result. The use of mechanical patient lift systems is advantageous
in reducing the load on the back and healthcare workers are recommended to use
these systems 13, 14.
They
also found that LBP was more common among caregivers of patients with motor
complete lesion identified according to the American spinal injury impairment
scale (AIS). transfer and locomotion of the patients nursed by caregivers with
LBP were significantly lower than those of patients nursed by caregivers
without LBP15 .
LBP
causes a large financial burden on individuals, families, communities, industry
and governments including the costs of medical care, compensation payment,
productivity loss, employee retraining, administrative expenses and litigation 16.
Low
back pain (LBP) is well recognized to be an enormous general health problem and
is the leading cause of activity limitation throughout much of the world. LBP
is a major problem all over the world, especially in low and middle income
countries 17.
Ethical clearance:
Ethical
Clearance: Ethical
clearance has obtained from Hosmat College of Physiotherapy and Research
Institute, Bangalore to conduct this study with reference number: 33/PHSIO/IRB/2018-19dated 07/06/2018.
Conflicts of Interest
The author declares that
there is no competing interest in publishing this article.
Fund for the study:
This is self-funded study.
CONCLUSION
This study aimed to find out the
prevalence and characteristics of low back ache of caregivers of the adult with
low back pain. Study revealed 51.9% prevalence of low back pain among the SCI
caregivers. Duration of injury was the key factor for the occurrence of low
back pain.
REFERENCES
Dunn KM, Croft PR. (2004). Epidemiology and natural history of low back pain. Eura Medicophys., 40(1): 9-13.
Tong HC, Haig AJ, Nelson VS, Yamakawa KS, Kandala G, Shin KY. (2003). Low back pain in adult female caregivers of children with physical disabilities. Arch Pediatr Adolesc.; 157:1128-1133.
Feng CK, Chen ML, Mao I F. (2007). Prevalence of and risk factors for different measures of low back pain among female nursing aides in Taiwanese nursing homes. BMC Musculo skelet Disord; 8: 52.
Bardak a, Erhan and Gündüz (2012). Low back pain among caregivers of spinal cord injured patients j rehabil med.; 44: 858-861.
Ebru Yilmaz Yalcinkaya, et al. (2007). A Pilot Study Low Back Pain Prevalence and Characteristics in Caregivers of Stroke Patients, 17(5): 389-393.
Tong HC, HaigAJ, NelsonVS, YamakawaKS, KandalaG, ShinKY (2003). Low back pain in adults’ female caregivers of children with physical disabilities. Arcives of pediatric and Adolescence Medicine; 157(11):1128-33.
TomoikaK, KumagaiS, HiguchiY, TsujimuraH, AraiY, Yoshida J. (2007). Low back load and satisfaction rating of caregivers and care receivers in bathing assistance given in nursing home for the elderly practicing individual care) Sangyo Eiseigaku Zasshi; 49(2); 54-58.
Majim Y, HorikikawaJ, ShonoI, (2004). Study on the Lower back pain in home helper’s and. Development of materials for occupational health education). 1; 26(1); 59-74.
Brown AR, Mulley G P (1997). Injuries sustained by caregivers of disabled elderly people. Age Ageing; 26(1); 21-23.
MarrasWS, Davis KG, Kriking BC, Bertsche PK. (1999). A Comprehensive analysis of low back disorders risk and spinal loading during the transferring and repositioning of patients using different techniques, Ergonomicsn ; 42(7);904-926.
TomoikaK, KumagaiS, HiguchiY, TsujimuraH, AraiY, Yoshida J. (2007).Low back load and satisfaction rating of caregivers and care receivers in bathing assistance given in nursing home for the elderly practicing individual care.)Sangyo Eiseigaku Zasshi , 49(2); 54-58.
SchibyeB, Hansen AF, Hye-Knudsen CT, (2003). Biomechanical analysis of the effect of changing patient-handling technique. Appl Ergon; 34(2):115-123.
FrangalaG, FragalaM, Pontani-Baily L. Proper positioning of clients: a risk for caregivers.) AAOHN J .2005Octuber; 53(10); 438-442.
Davidson M & Keating J (2001). A comparison of five low back disability questionnaires: reliability and responsiveness. Physical Therapy; 82:8-24.
Joshua Israel Vincent, Joy Christine Mac Dermid Ruby Grewa, Vincent Prabhakaran Sekarand Dinesh Balachandran, (2014). Translation of Oswestry Disability Index into Tamil with Cross Cultural Adaptation and Evaluation of Reliability and Validity, Orthopaedics Journal, 8, 11-19.
Matthew O.B. Olaogun, Rufus A. Adedoyin, Innocent C. Ikem & Olubusayo R. Anifaloba Physiotherapy Theory and Practice, Volume 20, 2004-Issue 2; 10 Jul 2009.
Craig CL, Marshall AL, et al. (2003). International physical activity questionnaire: 12-Country reliability and validity. Medicine and Science in Sports and Exercise, 35(8):1381-395.
Citation:
Gummadi Ashish (2020). A study to find out the prevalence and characteristics of low back ache among caregivers of adults with spinal cord injury, ijmaes; 6 (4); 829-835.
2Lecturer, Padmashree Institute of Physiotherapy,
Bangalore, Karnataka, India
Corresponding Author:1Professor, Padmashree Institute of Physiotherapy, Bangalore, Karnataka, India, Mail id: heerapt1977@gmail.com
ABSTRACT
Introduction: A case of 48 year old female patient with multiple fractures atright shoulder, chest and Pelvis was admitted in BGS Global hospital Kengeri, Bangalore. The patient met with an accident in which a tractor passed though half of her body leading to multiple fractures. As most of the fractures were turned out to be stable the patient was given painkillers and calcium tablets and started physiotherapy after 1 week. Methodology: Physiotherapy was started with Ankle Toe Movements, ROM exercise, sponge ball exercise, Incentive spirometry, Trunk rotation exercises, and gentle massage on the injured areas. The patient was given gait training in later stage followed by exercises in walker. Pre and post assessment taken for muscle power of shoulder and hip, Visual Analogue Scale for body pain and Functional Independent Measures to find the outcome. Result: After 8 weeks of daily physiotherapy, the patient improved with muscle power, reduced body pain, improved body function and the patient started walking without any assistive devices. Conclusion: With immediate physiotherapy even with multiple fractures the patients can get back to their Activities of Daily Living. Keywords: Fracture Rehabilitation, Muscle Power, Visual Analogue Scale, Functional Independent Measures, Activities of Daily Living,
Received on 15th August 2020, Revised on 28th August 2020, Accepted on 31st August 2020, DOI:10.36678/IJMAES.2020.V06I03.006
INTRODUCTION
A 48 year old
female patient named Niveditha who was housewife by profession presented with
pain on pubis and upper back region along with right shoulder and right area of
chest. History of present illness showed that on 6th December 2018,
patient went to pond to immerse a god idol after a prayer when a tractor passed
through half of her body. She was immediately shifted to BGS global hospital
Kengeri, Bangalore, where X ray was taken and it was found that she had
multiple fractures of ribs, pelvis, neck of femur and both pubic rami. Along
with that she had also sustained injury on the spine of scapula. But all the
fractures were found to be stable. Her shoulder was immobilized in a sling for
a week whereas, for remaining fractures painkillers and calcium tablets were
advised by Orthopedician1. She was then started on physiotherapy
protocol.
METHODOLOGY
Before the
physiotherapy treatment pre values were taken for Pain using VAS scale, MMT for
muscle power of shoulder and hip and functional Independence through Functional
Independence measure 2,3,4.
Physiotherapy was started with ankle toe movements5, limited
Range of Motion exercises for right upper and lower limbs and full ROM
exercises for left upper and lower limbs6. Patient was advised for
bed rest to prevent pressure sores and she was kept in air Bed7. For
the fingers, patient was given a sponge ball and was advised to squeeze it at
least 3 times a day (1 set of 10 repetitions each time) 8. As
patient was depressed she was given psychological counselling9. The
patient had mild pleural effusion for which she was given incentive spirometry
(1 set of 10 repetitions each time) twice a day10.
On 3rd
week the repeat X ray was taken on which it was seen that fractures were not
healed completely. The shoulder sling was removed and trunk rotation exercises
were started carefully with 15 degrees of spinal rotation11.
On 4th
week, patient’s preparation for sitting was started. Initially patient was
bought to inclined position by placing 2 pillows over her entire back to avoid
the postural hypotension, which could have occurred had the patient been brought
to 90° supine lying directly. The numbers of pillows were weekly increased to
increase the inclination. By 8th week patient was made to sit
90°.After that the patient was slowly brought to long sitting12.
Once long
sitting was achieved, high sitting training was started13. Then
sitting to standing practice was started for the patient with the support from
the physiotherapist14.Once the patient was comfortable in standing
position she was made to stand for more time with the help of walker and it was
followed by walking few steps with the help of walker15.Slowly the
patient could walk herself with the help of walker.
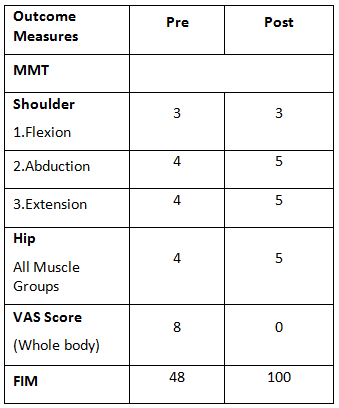
On 8th week, a repeat X ray was done which showed healed fractures. The patient was then taught weight lifting and weight bearing exercises16. The patient started walking without any walking aids. At this stage the post outcome measures scores were taken [Table 1] which showed good improvement. Patient was already off the medications except calcium tablets and she was not taking even painkillers. The patient was than taught home exercises and regular physiotherapy was stopped.
Table 1: Pre and Post Values of Outcome Measures
Ethical Clearance: Ethical clearance has obtained from BGS
Global hospital Kengeri, Bangalore to conduct this study.
Conflict of interest: There
was no conflict of interest to conduct this study.
Fund for the study: It
was aself financed study.
CONCLUSION
Early
physiotherapy intervention is quite helpful for improving the functional
independence of patient even in multiple fracture case. ROM exercises, Bed
Mobility, Trunk rotation exercises, functional reeducation along with
psychological counselling can help a
great deal to make the patient independent.
REFERENCES
Wraighte PJ, Scammell BE. (2006 Jun).
Principles of fracture healing. Surgery (Oxford). 1; 24(6):198-207.
Bergh I, Sjöström B, Odén A, Steen B. (2001
Oct 1). Assessing pain and pain relief in geriatric patients with
non-pathological fractures with different rating scales. Aging Clinical and
Experimental Research, 13(5):355-61.
Aitken DM, Bohannon R W. (2001 Mar 1). Functional
independence measure versus short form-36: relative responsiveness and
validity. International Journal of Rehabilitation Research, 24(1): 65-8.
Gajdosik RL, Bohannon RW. Clinical
measurement of range of motion: review of goniometry emphasizing reliability
and validity. Physical therapy. 1987 Dec 1; 67(12):1867-72.
Hickey BA, Cleves A, Alikhan R, Pugh N,
Nokes L, Perera A. (2017 Sep 1). The effect of active toe movement (AToM) on
calf pump function and deep vein thrombosis in patients with acute foot and
ankle trauma treated with cast–A prospective randomized study. Foot and Ankle
Surgery, 23(3):183-8.
Kisner CA, Colby LA. (2012). Range of
motion Therapeutic exercise foundations and Techniques, 61-73.
Biggie J, et al. (1999 Jul). Air
distribution device for the prevention and the treatment of decubitus ulcers
and pressure sores. United States patent US, 5; 926; 884.
Magnus CR, et
al. (2013 Jul 1). Cross-education for improving strength and mobility after
distal radius fractures: a randomized controlled trial. Archives of physical
medicine and rehabilitation, 94(7); 1247-55.
Cuijpers P,
van Straten A, van Schaik A, Andersson G. (2009 Feb 1). Psychological treatment
of depression in primary care: a meta-analysis. British journal of general
practice., 59 (559); e51-60.
Overend TJ, et al. (2001 Sep 1). The effect of
incentive spirometry on postoperative pulmonary complications: a systematic
review. Chest; 120(3):971-8.
Yamauchi T.(2015 Jun 1). The effect of trunk
rotation during shoulder exercises on the activity of the scapular muscle and
scapular kinematics. Journal of Shoulder and Elbow Surgery; 24(6):955-64.
Ladozhskaya-gapeenko EE, et al. (2018 Jul 3). Method
for treating and preventing diseases having neurological, cardiological and
therapeutic profiles. United States patent US, 10; 10; 469.
Arry RH. (2004 Nov). The interactional
management of patients’ physical incompetence: a conversation analytic study of
physiotherapy interactions. Sociology of Health & Illness. 26(7):976-1007.
Hoppenfeld S, Murthy VL, editors. Treatment and
rehabilitation of fractures. Lippincott Williams & Wilkins; 2000.
Härdi I, Bridenbaugh SA, Gschwind YJ, Kressig
RW. (2014 Apr 1). The effect of three different types of walking aids on
spatio-temporal gait parameters in community-dwelling older adults. Aging
clinical and experimental research, 26(2); 221-8.
Yung P, Lai YM, Tung PY, Tsui HT, Wong CK, Hung VW, Qin L. (2005 Aug 1). Effects of weight bearing and non-weight bearing exercises on bone properties using calcaneal quantitative ultrasound. British journal of sports medicine, 39(8):547-51.
Citation: Heera vijayakumar, Diker Dev Joshi (2020).Rehabilitation of a patient with multiple fractures caused by tractor running over half of body: A case Report, ijmaes; 6 (3); 825-828.
2B.P.T. Graduate, Faculty of Physiotherapy, Dr.MGR.
Educational and Research Institute, Deemed to be University, Chennai,
Tamilnadu, India
Corresponding
Author:
1Pofessor, Faculty of Physiotherapy, Dr.MGR. Educational and Research Institute, Deemed to be University, Chennai, Tamilnadu, India Mail id: physiojibi@gmail.com
ABSTRACT
Background of the study: Overweight is more body fat than optimally healthy individuals, overweight is common where food supplies are plentiful and life style is sedentary. Plyometric is designed to enhance muscular power and explosiveness. The word aerobic meaning exercise with oxygen, high intensity aerobic exercise can help on control weight and reduce stress. Objective of the study was to find the effect of plyometric exercise and high intensity aerobic exercise and also to compare the effect between the exercises among overweight college students. Methodology: This was a comparative study with quasi experimental design. The subjects were divided into two equal groups, 15 samples in Group A and Group B by convenient sample method. Group A received high intensity aerobics like jogging, burpees, mountain climber exercise, squat with side step, wall push ups, where Group B received plyometric exercises like squat jack, skater jump, jumping side lunge, rock star jump and high knees. Both exercises were given for three sessions in a week. Inclusion criteria include BMI of 25-30 and above, both male and female college students of aged 18-23 years. The measurement tool used was Body Mass Index and Waist Circumference. Result: The result showed a decrease in BMI and waist circumference in both the groups. But the weight reduction was more in Group A when compared to the Group B with p >0.000. Conclusion: The study concluded that high intensity aerobic exercise decreases the BMI and waist circumference effectively among overweight college students when compared to the plyometric exercises. Keywords: Plyometric, High intensity aerobic exercise, Waist circumference, Body Mass Index
Received on 15th August 2020, Revised on 27th August 2020, Accepted on 31st August 2020, DOI:10.36678/IJMAES.2020.V06I03.005
INTRODUCTION
Overweight is having more body fat than
is optimally healthy individuals. The definition of overweight in adults has
variations over time. Obesity and overweight constitute an important public
health problem because of associated increase risk of hypertension, coronary
heart disease, type 2 diabetes, stroke, gall bladder disease, certain type of
cancer, osteoarthritis, sleep apnoea and other disorders. Overweight range is
calculated according to the body mass index (BMI), where BMI >25 1, 2.
High intensity aerobics will help to
control weight and reduce stress by conditioning the heart and lungs with the
help of oxygen (4). High intensity aerobics will help to relax the
tensed muscles and regular practice of aerobics will increase the production of
endorphins (a natural sedative) and catecholamine (chemical substance which
stabilize the mood). So, long term aerobic exercise is considered to be reasonable
and effective to reduce weight. Some scholars suggest that high intensive
exercise of 85% VO2 max with appropriate positive rest in short time is more
effective to lose weight 3, 4, 5.
Plyometric is a type of training were
muscles undergo a rapid elongation followed by immediate shortening
(stretch-shortening contraction) utilizing the elastic energy stored during
stretching phase 7. Plyometric training is a fantastic cardio work
out and a great way to burn the calories. So, it is an effective work out
supplement to lose weight. In fact muscle stronger and improve endurance
capabilities. It enhances the metabolism and helps to burn calories. Indeed,
this exercise will facilitate weight loss 6, 7.
Both high intensity aerobics and
plyometric are meant for burning calories by increasing metabolism. So, it is
considered as an important component to reduce overweight. Body mass index
(BMI) is a simple and widely used method for estimating body fat mass. Belgian
statistician developed BMI in 19th century (4). BMI is
not only used classify obesity and overweight but also to find out life
expectancy and prevalence of overweight and obesity related issues and co
morbidities 8,9,10
METHODOLOGY
This was a comparative study with quasi
experimental design. The subjects were divided into two equal groups, 15
samples in Group A and Group B by convenient sample method. All samples were
selected for the study from the ACS medical college and hospital, Chennai.
Group A received high intensity aerobics like jogging, burpees, mountain
climber exercise, squat with side step, wall push ups, where Group B received
plyometric exercises like squat jack, skater jump, jumping side lunge, rock
star jump and high knees. Both exercises were given for three sessions in a
week. Inclusion criteria include BMI of 25-30 and above, both male and female
college students of aged 18-23 years. The measurement tool used was Body Mass
Index and Waist Circumference. The study was conducted for duration of 3
months. Subjects with hypertension, any cardio vascular disease, any
depressions, chronic renal failure, smoking status, history of diabetes, any
history of recent fracture were excluded from the study.
Procedure: According to the BMI reading
of over (26-30) is considered as overweight and the BMI was calculated from the
following equation BMI(in kg m2)=Body mass(in kg)/Height 2 (in m).Thirty
college students were selected from the ACS medical college and hospital, in
the age group of 18-23 years selected conveniently .The selected 30 subjects were
provided with the informed consent after obtaining proper consent the
selected and subjects were divided into
two equal groups of fifteen each namely high intensity aerobic exercise was
given to group A(15 subjects) and plyometric exercise was given to group B(15
subjects).Overweight was tested before(pre) and
after(post) the training program for both experimental groups by using Waist circumference and
conventional method was used to measure BMI, weight, height of each subjects
was measured using a wall stadiometer, WHR, body fat percentage%(4).The
obtained values were recorded. According to the protocol, the exercises had
been given for Group A (High Intensity Aerobic Exercise) and Group B
(Plyometric Exercise) followed by three months, the BMI and Waist circumference
was again measured and the obtained values are recorded.
Exercise
Intervention
The selected subjects had undergone
plyometric and high intensity aerobics thrice a week which have been in
practice. Before the training they had undergone warm up for 5 minutes and cool
down for 5 minutes. The group A has been engaged with High intensity aerobics
of Jogging, Burpees, Mountain climbers, Squat with side sitting, Wall push up,
the group B has been engaged with an Squat jack, Skater jump, Jumping side
lunge, Rock star jump, High knees. Each exercise consists of 5 reputations in
high interval of 30 seconds practice and low interval of 10 seconds of resting
period.
Group A (High
Intensity Aerobic Exercises)
Jogging: Jogging is running at a gentle pace. It is as running slower than 6 miles per hour (10 km/h).Jogging will have a wider lateral spacing of foot strikes, creating side- to-side movement that likely adds stability at slower speeds or when coordination is lacking.
Fig.1 Jogging
Burpees:
Burpees or squat thrust is a full body exercise used in strength training. The
basic movement is performed in four steps and known as a” four-count burpees.”
Method: Begin in a standing position. Move into a squat position with your hands on the ground (count-1). Kick your feedback into a plank position, while keeping your arms extended (count 2). Immediately return your feet into squat position (count 3). Stand up from the squat position (count 4).
Fig. 2 (a, b, c, d) Burpees
Mountain Climber
Exercise: Mountain
climbers are a great total body exercise in which you are going to utilize your
entire core because it is started in plank position.
The shoulders should stabilize your upper body. The triceps muscle should work isometrically to keep you in place.
Fig.3 (a, b). Mountain ClimbersFig.4 (A, B)Squat with Side Step
Squat With Side Step: Side step and squat. Stand with
your feet together. With your right foot take a wide step out to the right and
squat down. As you straighten the legs, step your right foot back in. repeat on
the left side.
Wall Push Ups: Face the wall, standing a little farther than arm’s length away, feet- shoulder width apart. Lean your body forward and put your palms flat against the wall at shoulder height and shoulder width apart.
Fig.5Wall Push Ups
Group
B (Plyometric Exercises)
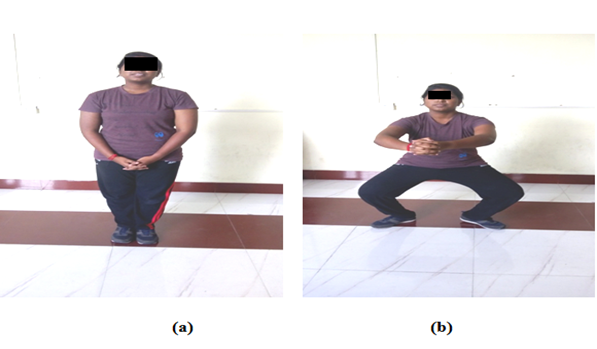
Squat Jack: Squat is a compound, full body
exercise that trains primarily the muscles of the thigh, hips and buttocks,
quadriceps femoris muscle( vastus lateralis, vastus medialis, vastus
intermedius and rectus femoris),hamstrings as well as strengthening the bones,
ligaments and insertion of the tendons throughout the lower body.
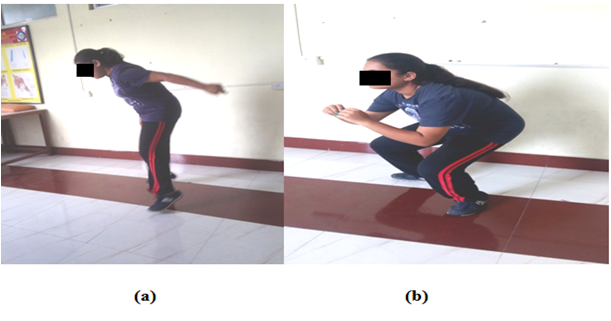
Skater Jump: It is landing in one foot
without touching the other one down and at the same time you can touch the
ground with each jump so to make this a little bit easier you can touch your
foot down on each sides alternatively.
Fig.6 (a, b) Squat JackFig.7 Skater JumpandFig.8 Rock Star Jump
Jumping Side Lunge: Stand on your left leg with your hips and knees slightly bent extend your left hip, knees and ankle to jump forward and to the right at a 45-degree angle land on the ball of your right foot with your hips and knees slightly bent to absorb the impact immediately jump off your right leg in the opposite direction.
Fig.9 (a, b) Jumping Side Lunge
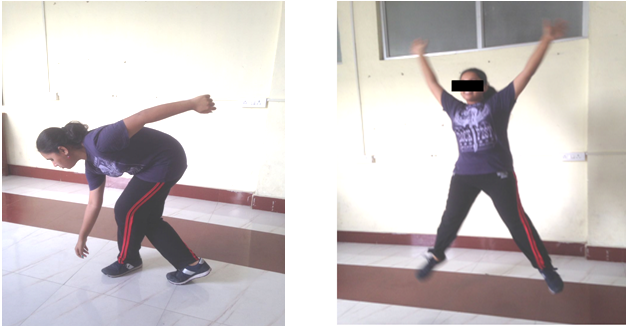
Rock Star Jump: Also called as side-straddle
hop in the US military, is a physical jumping exercise performed by jumping to
a position with the legs spread wide and the hands touching overhead, sometimes
in a clap, and then returning to a position with the feet together and the arm
at the sides.
High Knees: Skip in place by hopping on your right leg while bringing the left knee up towards your chest. Engage your abs as the knee comes towards your chest. Switch legs, and keep skipping while pumping your arms. This completes one reputation.
Fig.10 (a, b) High Knees
Data analysis and interpretation
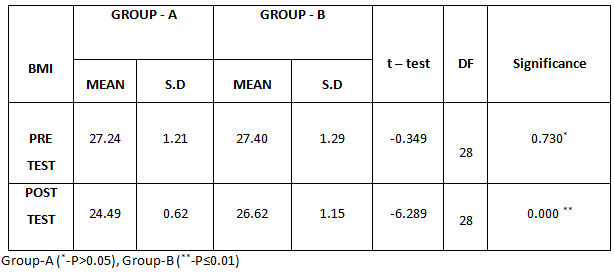
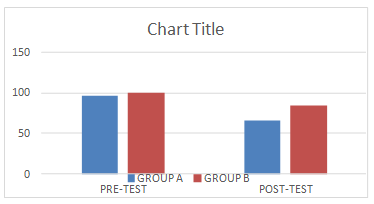
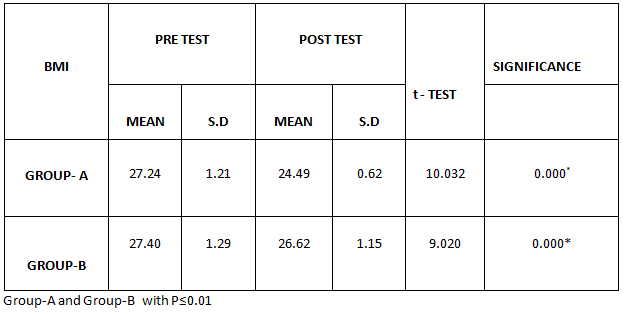
Table-1 comparison of BMI between Group- A and Group- B in Pre and post test
The above table reveals the mean,
standard deviation(S.D),T- test, degree of freedom (DF) and P values of the BMI
between (Group A) and (Group B) in pre-test and post- test.
This table shows that there is no significant difference in the pre-test values of the BMI between Group A and Group B (*P>0.05). This table shows that statistically significant difference in the post test values of the BMI between group A and group B (**-P≤0.01).
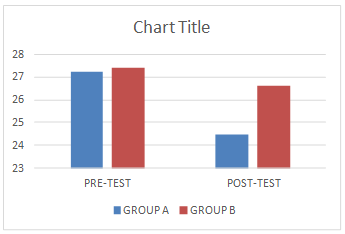
Graph – 1.Comparison of BMI between Group A and Group B in pre and post test. Table- 2: Comparison of waist circumference between group-a and group – b in pre and post test
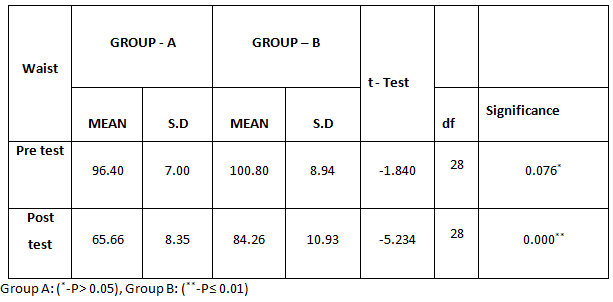
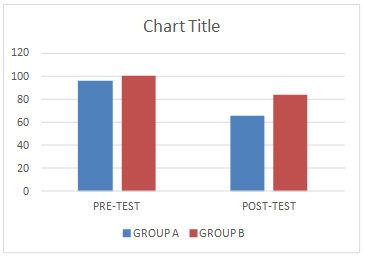
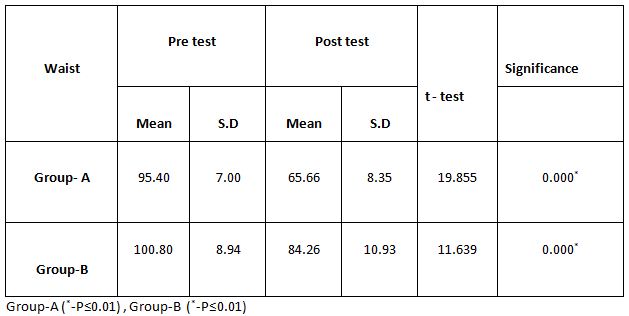
The above table reveals the mean
,standard deviation (S.D),T-test, degree
of freedom(DF) and P-values of the waist circumference between (group A) and
(group B) in pre-test and post-test.
This table shows that there is no significant difference in pre-test values of the waist circumference between group A and group B (*P>0.05). This table shows that statistically significant difference in post-test values of the waist circumference group A and group B (**-P≤0.01)
Graph-2: Comparison of Waist Circumference between Group A and Group B in the pre and post test. Table 3: Comparison of BMI within Group A & Group B between Pre & Post Test Values
The above table reveals the mean,
standard deviation (SD),t-values and P-values of the BMI between pre-test and
post-test within group A and group B.
In BMI there is a statistically highly significant difference in the pre-test and posttest values within group A and group B. (**-P≤0.01)
Graph-3: Comparison of BMI within Group-A and Group-B between pre and post test values Table 4: Comparison of waist circumference within Group-A & Group-B between pre & post test values
The above table reveals the mean,
standard deviation (SD), t-value and p-value of the waist circumference between
pre-test and post-test within group A and group B.
In waist circumference there is a statistically significant difference between the pre-test and post-test values within group A and group B (*-P≤0.01).
Graph 4: Comparison of Waist Circumference within Group A and Group B between Pre and Post- Test Values
RESULT
Pre and Post-test values within Group A
and B, it shows a statistically significant difference in the BMI where P value
is 0.000*. And also in pre and post-test values within Group A and B, it
reveals significant difference on Waist Circumference where P value is 0.000*.
On comparing between the Group A and B
found significant difference of P value 0.000*.
BMI found significant mean difference of 2.75 (27.24-24.49)
and 0.78 (27.40-26.62) respectively.
Waist Circumference also found significant difference with mean
difference of 29.74 (95.40-65.66), 16.54 (100.80-84.26)
respectively.
DISCUSSION
Based on the selection criteria 30
subjects with overweight of 25 to 30 were participated in the study. The
purpose of this study was to compare the effect of plyometric versus high
intensity aerobics among overweight college students.
Aerobic exercise has significant
improvement on waist circumference than plyometric exercises. Outcome measures
used for this study were Body Mass Index and waist circumference 11.
Plyometric burns the maximum amount of
calories in the shortest amount of time while toning the body from head to toe,
reported the importance of Plyometric exercise in fitness. Plyometric exercises
to a High intensity interval training program may be more beneficial than only
High intensity interval training in obese female adolescents 12, 13.
Training at high intensity is superior to
improve cardiopulmonary fitness and to reduce % body fat in adults with obesity
compared to traditional exercises. Another issue is the motivation for an
exercise program in person with overweight depression; a negative body image
and embarrassment are factors that can influence the decision to participate in
an exercise program. Recent evidence suggests that HIIT can be a time-efficient
strategy to promote health in sedentary overweight /obesity individuals 14.
In this review and Meta analysis, the
effectiveness of high intensity training in terms of weight reduction was
compared to plyometric forms of exercise in overweight college students. Based
on the results on this Meta analysis we can conclude that training at high
intensity aerobic is a better method to reduce overweight than plyometric15.
In this study the values of BMI and waist
circumference in centimetres of pre-test and post-test were compared by the
mean difference. When the inter group mean values of BMI were analysed, in
Group A mean for BMI pre-test and post test was BMI 27.24 and 24.49
respectively. The mean values of Group B for pre test and post test was 27.40
and 26.62 respectively from the data analysis. The result shows that the
reduction in body weight is more in Group A (High intensity aerobic exercise)
compare to Group B (plyometric exercise).
When the inter group mean values of waist
circumstance was analysed, Group A pre test mean waist circumstance 96.40 and
post test mean waist circumstance 65.66 .The mean values of group B pre test
mean waist circumstance 100.80 and post test mean 84.26 from the data analysis
it shows that there was reduction in the waist circumstance in group A (High
intensity aerobic exercise).
Ethical Clearance: Ethical clearance has obtained from
Faculty of Physiotherapy, DR.MGR. Educational and Research Institute, Chennai
to conduct this study with reference number: A–033/ PHSIO/IRB/2017-18dated
07/01/2018.
Conflict of interest: There
was no conflict of interest to conduct this study.
Fund for the study: It
was aself financed study.
CONCLUSION
This study concludes that the high
intensity aerobics has considerable effect in reducing the weight among
overweight college students. Therefore the HIAE is considered to be more
effective than plyometric exercise program.
High Intensity Aerobic Exercise can
effectuate weight reduction in a shorter period of time, but also mechanisms
like increased post exercise fat oxidation and a decreased post exercise
appetite could play a role.
Training at high intensity is superior to
improper cardio pulmonary fitness and to reduce body fat percentage in adults
with overweight compared to plyometric exercise.
REFERENCES
Young-Han Park, PhD and Jung-Ho lee, PhD: (2017).The effects of abdominal interferential current therapy on waist circumference and visceral fat distance in obese women., J.Phys Ther.Sci ; 29; 1680-1683.
A Febin jebaraj, Dr C Robert Alexander (2016). Effect of plyometric and aerobic exercise on obesity among school students. International journal of physical education, sports and health, 3 (2); 83-85.
Liye zheng (2016). Influence of aerobic it intensive training on obese college students. Biomedical research, 279 (2); 392-395.
Derrick cetin (2016). Comprehensive evaluation for obesity: Beyond Body mass index., J Am Osteopath Assoc., 116(6); 376-382.
Racil, Ghazi Etal (2015). Plyometric exercise combined with high intensity interval training improves metabolic abnormalities in young obese female more so than interval training alone. Canadian science publishing apnm -0384, R2.
Alberto Carvalho, Paulo Maurao and Eduardo Abade (2014). Effect of strength training combined with specific plyometric exercise on body composition, vertical jump height and lower limb strength development in elite male hand ball players: a case study, Journal of human kinetics volume. 41; 125-132.
Su Reid- St. John (2015). Blast fat with plyometric. Make your body a jiggle –free zone with these fun fat blasting moves. (4); 4422-4438.
KwonHR. Kim HR (2014). Effect of aerobics exercise on abdominal fat, thigh muscle mass and muscle strength, Korean diabetes, 34; 23-31.
Sousa NMendes R., et al (2013). Long –term effects of aerobic training versus combined aerobic and resistance training in modifying cardiovascular disease risk factors in healthy elderly men., Geriatr Gerontol Int; 13; 928-935.
Coquart J.B., lemaire, et al (2010). Intermittent versus continuous exercise: effects of perceptually lower exercise in obese women. Med.Sci.Sports.Exercise.40 (8);1546-1553.
Raquel patricia ataide lime et al (2015). BMI, overweight status and Obesity adjusted by various factors in all age groups in the population of a city in northern Brazil. P: 914-271. 4141/ F: 914- 827- 5308.
Harris (2009). Effect of school based physical activity interventions on body mass index in children, a meta-analysis, 31,180(7); 719-26.
Baker LB, Lang JA, Kanney WL (2009). Change in body mass accurately and reliably predicts change in body water after endurance exercise. Eur J Appl Physiol; 105; 959-967.
Gan SK, Thompson W (2003). Changes in aerobic capacity and visceral fat. Diabetes care, 26; 1706-13.
Owens S, Gutin Allison Riggs Ferguson M, et al (1999). Effect of aerobic training on total and visceral fat in obese children’s., Medicine and science in sports and exercise, 31(1); 143-148.
Citation: Jibi Paul, T.Bhuvaneswari (2020).Plyometric versus high intensity aerobic exercise among over weight college students, ijmaes; 6 (3); 811-824.
2 Student M.P.T Neurology, Hosmat College of Physiotherapy, RGUHS University, Bangalore, Karnataka, India
Corresponding Author:
1Principal of Hosmat college of Physiotherapy, RGUHS U niversity, Bangalore, Karnataka, India Mail id: purnimasingh29@gmail.com
ABSTRACT
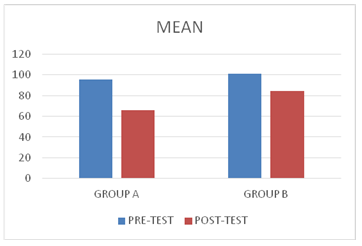
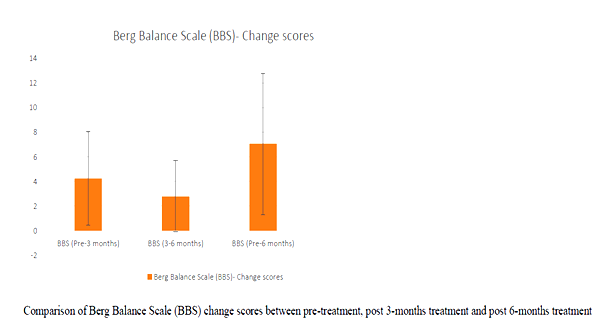
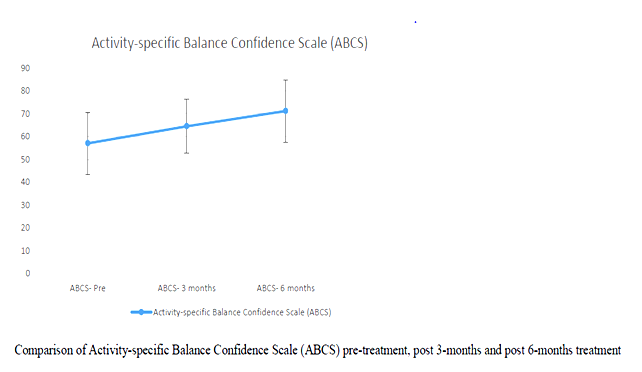
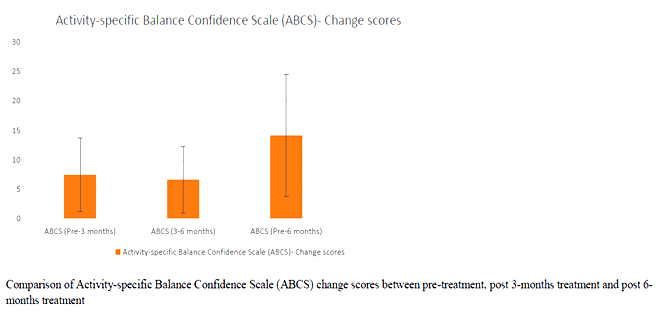
Introduction: Parkinson’s disease is a major concern when the disease progresses to the middle stage of the illness. The typical features of Idiopathic Parkinson’s disease (IPD) are tremors impairment of the muscle tone, involuntary movement and bradykinesia. Improvement in strength and balance of IPD patients has improved their mobility functions. Especially, balancing exercises on uneven surfaces with eyes open and closed help them in gaining confidence to move outdoor independently with lesser risk of fall. Methodology: A total numbers of 30 subjects were considered for the study. All participants underwent two sets of measurement. Pre-test which was done at the beginning of the study & the post-test which was done at the end of 3 & 6 months of the study. 30 patients effectively completed the set of balancing and strengthening exercises with eyes closed & open for the period of 6 months. Results: All the subjects showed significant changes in BBS & ABC scales after 6 months of strength and balance training programs. The mean value of the pre- test scores were BBS – 37.23 ± 10.7 ABC – 57 ± 13.62 and post – test scores were BBS – 44.30 ± 8.78 ABC – 71.17 ± 13.62. Conclusion: From the statistical analysis it is evident that strengthening and balancing training program on uneven surfaces are effective in reducing the risk of fall and increasing the confidence of mobility in patients with PD. keywords: Parkinson’s disease; strengthening exercises; Therabands; balancing exercises.
Received on 15th August 2020, Revised on 27th August 2020, Accepted on 31st August 2020, DOI:10.36678/IJMAES.2020.V06I03.004
INTRODUCTION
Idiopathic Parkinson’s disease [IPD] is a
group of the conditions affecting the motor system hence also called as motor
system disorder. This is resulted due to the loss of dopamine producing in the
brain cells.
Characteristics of Parkinson’s disease are
progressive loss of muscle control, which leads to trembling of the limbs and
head while at rest, stiffness, slowness, and impaired balance. As symptoms
worsen, it may become difficult to walk, talk, and complete simple tasks1.
Most of the movement-related symptoms of
IPD is considered as the second most common neurodegenerative disorders.2
When the amount of dopamine is too low, communication between the substantia
nigra and corpus striatum becomes ineffective, and movement becomes impaired;
the greater the loss of dopamine, the worse the movement-related symptoms.
Other cells in the brain also degenerate to some degree and may contribute to
non-movement related symptoms of Parkinson’s disease.3
The cause of Parkinson’s disease is
unknown but researchers speculate that both genetic and environmental factors
are involved; some genes have been linked to the disease. Although it is well
known that lack of dopamine causes the motor symptoms of Parkinson’s disease,
it is not clear why the Dopamine-producing brain cells deteriorate.
Genetic and pathological studies have
revealed that various dysfunctional cellular processes, inflammation, and
stress can all contribute to cell damage. In addition, abnormal clumps called
Lewy bodies, which contain the protein alpha-synuclein, are found in many brain
cells of individuals with Parkinson’s disease. The function of these clumps in
regards to Parkinson’s disease is not understood. In general, scientists
suspect that Dopamine loss is due to a combination of genetic and environmental
factors2, 3.
Early symptoms of PD are subtle and occur
gradually. In some people the disease progresses more quickly than in
others.
The primary symptoms of Parkinson’s
disease are all related to voluntary and involuntary motor function and usually
start on one side of the body. Symptoms are mild at first and will progress
over time. Some people are more affected than others are. Studies have shown
that by the time that primary symptoms appear, individuals with Parkinson’s
disease will have lost 60% to 80% or more of the Dopamine-producing cells in
the brain. Characteristic motor symptoms include4:
Tremors: Trembling in fingers, hands, arms, feet, legs, jaw, or head.
Usually tremors occur while resting, but not while involved in a task. Tremors
may worsen when a person is excited, tired, or stressed.
Rigidity: Stiffness of the limbs and trunk, which may increase during
movement. Rigidity may produce muscle aches and pain. Loss of fine hand
movements can lead to cramped handwriting (micrographia) and may make eating
difficult.
Bradykinesia: Slowness of voluntary movement. Over time, it may become
difficult to initiate movement and to complete movement. Bradykinesia together
with stiffness can also affect the facial muscles and result in an
expressionless, “mask-like” appearance.
Postural instability: Impaired or lost reflexes can make it difficult
to adjust posture to maintain balance. Postural instability may lead to falls.
Parkinsonian gait: Individuals with more progressive Parkinson’s
disease develop a distinctive shuffling walk with a stooped position and a
diminished or absent arm swing. It may become difficult to start walking and to
make turns. Individuals may freeze in mid-stride and appear to fall forward
while walking.4
While the main symptoms of Parkinson’s
disease are movement-related, progressive loss of muscle control and continued
damage to the brain can lead to secondary symptoms. These secondary symptoms
vary in severity, and not everyone with Parkinson’s will experience all of
them, and may include. Anxiety, stress, confusion, memory loss or dementia,
constipation, depression, difficulty in swallowing, excessive salivation,
increased sweating, erectile dysfunction, skin problem, slowness of speech and
monotone speech, incontinence of urinary or urgency for urination. 5
Several guidelines have been published to
assist in the diagnosis of Parkinson’s disease. These include the Hoehn and
Yahr scale and the Unified Parkinson’s Disease Rating Scale. Tests are used to
measure mental capacity, behaviour, mood, daily living activities, and motor
function. They can be very helpful in the initial diagnosis, to rule out other
disorders, as well as in monitoring the progression of the disease to make
therapeutic adjustments. Brain scans and other laboratory tests are also
sometimes carried out, mostly to detect other disorders resembling Parkinson’s
is disease.
The diagnosis of Parkinson’s disease is
more likely if. At least two of the three major symptoms are present (tremor at
rest, muscle rigidity, and slowness). The onset of symptoms started on one side
of the body. Symptoms are not due to secondary causes such as medication or
strokes in the area controlling movement. Symptoms are significantly improved
with levodopa.
Researchers may disagree on the number of
stages of Parkinson’s disease (range from 3-5 stages). However, they all agree
the disease is a progressive disease with symptoms that usually occur in one
stage may overlap or occur in another stage. The stage increase in number value
for all stage naming systems reflects the increasing severity of the disease.
The five stages used by the Parkinson’s Foundation are:
Stage 1: mild symptoms (tremors
and/or movement symptoms like swinging arm while walking) do not interfere
with daily activities and occur on one side of the body.
Stage 2: Symptoms worsen with walking
problems and both sides of the body affected.
Stage 3: Main symptoms worsen with loss
of balance and slowness of movement.
Stage 4: Severity of symptoms
requires help; usually person cannot live alone.
Stage 5: Caregiver needed for all
activities; patient may not be able to stand or walk and may be bedridden
and may also experience hallucinations and delusions.5,6
Parkinson’s disease cannot be cured
completely but the symptoms can be relieved with the use of various medication
with carbidopa is usually given for the PD treatment, Carbidopa helps in delay
of conversion of levodopa into dopamine. The nerve cells use levodopa for the
production of dopamine and thus replenish the supply deficiency of the brain’s
dopamine7.
Thus, levodopa is very helpful (at least
¾) of Parkinson’s cases. Not all Parkinson’s symptoms respond equally to this
drug. Tremors don’t have much effect but bradykinesia and rigidity is
remarkably reduced. Balance issues and other symptoms may not be alleviated at
all. Anti-cholinergic have a great effect in controlling tremors and rigidity.
Bromocriotine, Pramipexole and ropinirole, mimics the role of dopamine thus
helping the neurons to use it as dopamine.8
An antiviral drug amantadine also helps in
reducing the symptoms. In May 2006, FDA also approved the drug called
Safinamide, which can be used for diminishing the experience of “off” periods
or patients with increasing symptoms of PD. In some cases, surgery can also be
done for the patients not responding well to drugs. Deep brain stimulation
(DBS) is now approved by U.S FDA (Food and Drug administration) where an electrode
is implanted in the brain and is connected to an electrical device called pulse
generator which can be externally programmed.
This process of stimulation reduces the need
of drugs thus decreasing the involuntary movements call dyskinesia which is a common
side effect of these drugs. This procedure of stimulation to brain also reduces
tremors, slowness and gait disturbances. DBS requires careful programming in
order to work correctly3, 8, 9.
Fall is very common in PWP. Gait
impairment, freezing of gait, cognition, loss of postural control is the common
cause of falling. This is not easily managed by medications only
Frequent falls can cause loss of mobility,
restriction in daily living activities, fractures and cost of treatment is
increased 10, 11.
Studies have shown that exercises can be
useful in preventing falls in PwP (patients with Parkinson’s disease).
Physiotherapy along with drug therapy is
the most commonly used procedure for PwP. However, the Cochrane reviews have
supported this procedure with many randomized control trials 7, 8, 12.
Many authors have suggested that balance
impairment in PD and normal old age changes causes decrease in the muscle
strength due to their sedentary lifestyle. It has been noted that strengthening
and balancing rehabilitation programs have reduced the risk of falls, prevent
dysfunction and dependency in the elderly 13, 20, 21.
METHODOLOGY
Study design: An
Interventional Study
Study population: Subjects who
are diagnosed with IPD by their Neurologist
Study setting: The study was conducted (testing &
Intervention) at Outpatient
department of Bethel Medical Mission HOSPITAL.
Study sample size A total of 30 patients
Sampling Method:
Purposive sampling
Study duration: 6
months
Selection criteria
Inclusion criteria:
Diagnosed with IPD by
their neurologist
Ambulatory and able to
follow simple commands
Patient with Unified
Parkinson’s Disease Rating scale score of 35 and above
Patient with a score
of above 40% on the Activities Specific Balance Confidence Scale (ABC).
Exclusion criteria:
Suffering from
unstable cardiovascular disease
Uncontrolled chronic
conditions that might interfere with the safety and conduct of the training and
testing protocol.
Patients participated
earlier in balance and strengthening program
Outcome measures tools used for the study
The Berg Balance Scale
(BBS)
The
Activities-Specific Balance Confidence Scale (ABC)
Material used: Data
collection Sheets, Stop watch,15 ft Walk way, 4-inch Foam Pads, Thera
bands, Chairs, Weight cuffs and Thera
tubes.
Methods: A
total of 30 subjects fulfilling the selection criteria were included in the
study after taking informed consent from each one of them. The Unified
Parkinson’s Disease Rating Scale (UPDRS) Score is used for their eligibility.
The Unified
Parkinson’s disease rating scale (UPDRS) has 4 sections
I-Mentation behaviour and mood
II- ADL activities
III- Motor examination
IV- Complication of therapy
Score – 0 to 147
Higher the score = Worst performance 12,15.
Baseline
evaluation of Balance was be done using The Berg Balance Scale (BBS) Score, The
Activities-Specific Balance Confidence Scale (ABC).
All
participants received the same Balancing intervention and Muscle strength
intervention for 6 months. Outcome
measurements of Balance and Muscle strength were assessed using The Berg
Balance Scale (BBS), The Activities-Specific Balance Confidence Scale (ABC) at
the end of 3 months & 6 months13,17.
Use of outcomes measures tools
All patients
were evaluated at baseline and at the end of 3 months & 6 months of
treatment period by the same examiner using Berg Balance Scale (BBS) 14 items
(0-4 points per task higher score=best performance).
This scale
evaluates balance during activities like sitting, standing and positional
changes.
The Activities specific
balance confidence scale (ABC) is the scale which examines patients perceived
level of balance confidence while doing 16 activity of daily living rated from
0 to 100 each14, 16.
Procedure for intervention
Balancing
exercise s were given thrice a week and strengthening exercises were given on
remaining 3 days a week.
Thus, the
duration for balance training was 30 minutes and strength training was for 15
minutes. Frequency of training – 3 days a week each for 6 days.
Balance
Intervention:
Balance exercise
session lasted for 30 min and was conducted on 3 non- consecutive days, every
week. Balance training programme include standard rehabilitation exercises for
balancing. This training improved balance in older adults with PD15, 16, 20.
Training was in 2 parts :
1.Standing on a 4-6-inch-thick foam pad with feet- shoulder width apart with eyes open and then eyes closed along with neck in neutral followed by neck extension for 20 sec. Repeated for 5 times.
2.Standing with feet – shoulder width apart without the foam pad with eyes open and then eyes closed along with neck in neutral followed by neck extension for 20 sec. Repeated for 5 times.
Muscle strengthening intervention:
Strengthening
exercises were done with weight cuffs, TheraBand & Theratubes. All participants
had undergone progressive strengthening of trunk, hip, knee, and ankle.
The training
protocol used standard principle of rehabilitation of using concentric and
eccentric muscles strength.
RESULTS
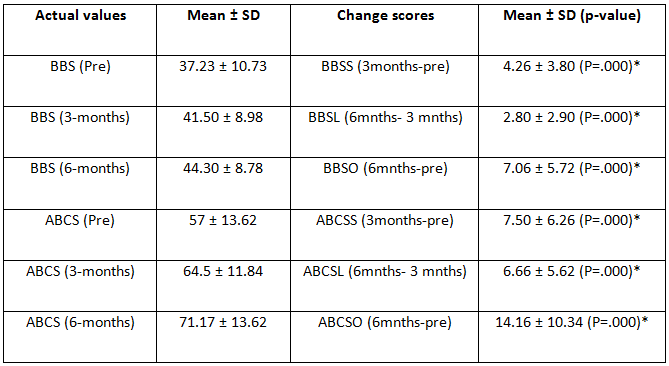
Primary analysis:
Pairwise comparisons were done for scores
of BBS and ABCS using paired t-test.
Secondary
analysis:
Correlation between Age and UPRSD was done
using Karl Pearson’s correlation coefficient.
Comparison of change scores and UPRSD
between gender was done using Independent t-test.
All analyses were done at 95% confidence interval using Statistical package for social sciences (SPSS version 22, Chicago, IL) for Windows software.
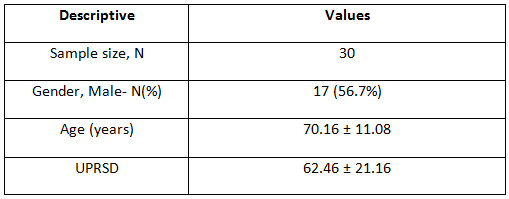
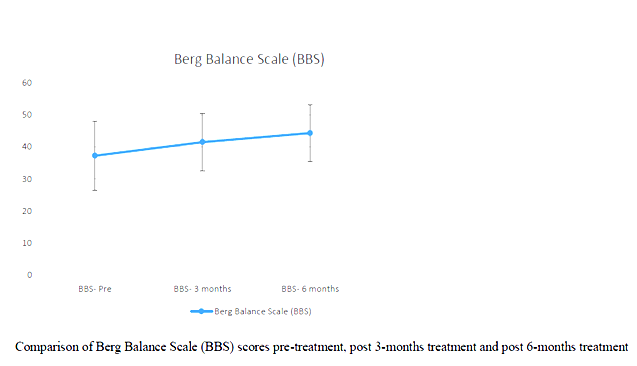
Tables and Graphs:
Table 1. Descriptive analysis Table 2. Pre and post data analysis Graph 1: Comparison of BBS by pre and post presentation Graph 2: Comparison of BBS by pre and post on bar presentation Graph 3: Comparison of activity based confidence scale on pre and post presentation Graph 4: Comparison of activity based confidence scale on pre and post on bar presentation
Correlation between age and UPRSD: Weak negative correlation existed (-.123) which was not statistically significant (p=.518)
Comparison of UPRSD between Genders:
Table 3: Comparison of UPRSD between Genders
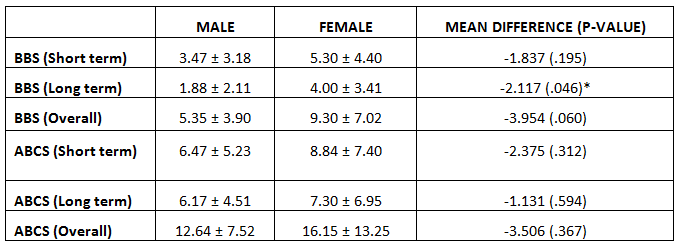
Comparison of BBS and ABCS change scores between Genders:
Table 4: Comparison of BBS and ABCS change scores between Genders
BBS
change score between 3-months and 6-months was better amongst women than men,
statistically significant at p=.046. All other change scores were not
influenced by gender (p>.05).
DISCUSSION
The main aim of the study was to evaluate
disease specific and balance related measure in the given population. The
clinical scales used in the study are sensitive in the evaluation of the risk
of fall in patients with Idiopathic Parkinson’s Disease. Cut-off scores of
these scales are very useful in clinical practice as it provides detailed
description about impaired functional activities and balance related activities
& can also be used to evaluate treatment outcomes.
The present study shows that balance and
strengthening exercises together help in reducing risk of fall and improves
functional mobility in patients with Idiopathic Parkinson’s disease.
In the study BBS and ABC pre and post test
scores were analysed. It has been noted than all of the participants improved
in their BBS and ABC scores.
BBS
change score between 3-months and 6-months was better amongst women than men,
& statistically significant at p=.046. All other change scores were not
influenced by gender (p>.05). Similar study was done in the year 2003 &
2015 where they studied the Effect of balance
and resistance training using computerized dynamic posturography (sensory
orientation test) SOT for balance and muscle strength in 15 patients with IPD.
Authors concluded that balance and strength of muscles can be improved in
patient with PD by training programmes of balance and high intensity resistance
12, 19.
A systematic review study reported the
evidence of resistance training on the strength and function in patients with
PD. The study demonstrated that moderate intensity training for 2-3 times per
week over 8-10 weeks can result in significant improvement in strength, balance
and others motor symptoms in patients with early to moderate stage of PD18,20,21.
Another randomized control trial of 210
patients with PD were divided into 3 groups and were educated for balance
training movement strategy training and strength training programs. The study
concluded that rehabilitation training reduces the risk of falls in patients of
mild to moderate stage of PD 19, 20
The present study results provide
validation and best combination of outcome measures used in PD. With these
scales risk of recurrent falls too can be determined. Although the patients
performed well according to the scales, but an independent validation of sample
is important in order to use into clinical practice.
Ethical clearance: The ethical approval was granted by the ethical
committees of the Hosmat College of Physiotherapy, Bangalore.
Conflict
of interest: There was no conflict of
interest to conduct this study.
Fund
for the study: It was self-financed study.
Limitations:
Small sample size, smaller time period of
study, Frequent follow up.
Recommendations:
Early stages of Parkinson’s and larger study size
CONCLUSION
The study result showed that Strengthening
and balancing exercises have a great effect on patients with Parkinson’s
disease. It delays the progress of the Disease and helps the patients to regain
their confidence in mobility and become more active and independent. According
to the statistical analysis female patients showed better response to the
training as compared to the male patients.
REFERENCES
Parkinson’s disease information page (January 18, 2019). National Institutes of Neurological Disorders and Stroke website. ninds.nih.gov/disorders/All-Disor ders/ Parkinsons Disease Information-Page. Updated June 12, 2108.
Kalia L V. et al.(August 2015). Parkinson’s disease; 386(9996); 8; 96-912. PMID 25904081.
Sveinbjornsdottir. S (Oct 2016). Quit;”The clinical symptoms of Parkinson’s disease” ; Journal of Neurochemistry.139 Suppl 1; 318-324; Bibcode: 2006JNeur. 26.9606G.
Braak, H et al. (1998). Staging of brain pathology related to patients with Parkinson’s disease. C. An algorithm (decision tree) for the management of Parkinson’s disease. Neurology; 50 Suppl 3; S157.
Poewe W (December 2006). “The natural history of Parkinson’s disease”. Journal of Neurology. 253 Suppl 7 (Suppl 7); VII2–6.
Marchese R, Bove M, Abbruzzese G. (2003).Effect of cognitive and motor tasks on postural stability in Parkinson’s disease: a posturographic study. Mov Disord., 18; 652 658.
Deane KHO, Jones D, Ellis-Hill C, Clarke CE, Playford ED, Ben-Shlomo Y. (2001). Physiotherapy for Parkinson’s disease: A comparison of techniques. Cochrane Database Syst Rev. : CD002815.
Deane KHO, Jones D, Playford ED, Ben-Shlomo Y, Clarke CE. (2001). (Physiotherapy versus placebo or no intervention in Parkinson’s disease. Cochrane Database Syst Rev. 3):CD002817.
Olanow CW, Koller WC. (1998). An algorithm (decision tree) for the management of Parkinson’s disease. Neurology, 50 Suppl 3; S157.
Chung CL, Thilarajah S2, Tan D3. (2016 Jan). Effectiveness of resistance training on muscle strength and physical function in people with Parkinson’s disease: a systematic review and meta-analysis. Clin. Rehabil., 30(1); 11-23.
Morris ME, Menz HB, McGinley JL, Watts JJ, Huxham FE, Murphy AT, Danoudis ME, Iansek R. (2015 Sep). A Randomized Controlled Trial to Reduce Falls in People With Parkinson’s Disease.Neurorehabil Neural Repair. 29 (8); 777-85.
Conradsson D, Löfgren N, Nero H, Hagströmer M, Ståhle A, Lökk , Franzén E. (2015 Oct). The Effects of Highly Challenging Balance Training in Elderly With Parkinson’s Disease: A Randomized Controlled Trial. Neurorehabil Neural Repair., 29(9); 827-36.
Corcos DM, Robichaud JA, David FJ, Leurgans SE, Vaillancourt DE, Poon C, Rafferty MR, Kohrt WM, Comella CL.(2013 Aug). A two-year randomized controlled trial of progressive resistance exercise for Parkinson’s disease. Mov Disord. 28(9); 1230-40.
Olanow CW, Wunderle KB, Kieburtz K. (2011 May). Milestones in movement disorders clinical trials: advances and landmark studies.MovDisord.,26(6); 1003-14.
Glendinning DS1, Enoka RM. (1994 Jan). Motor unit behavior in Parkinson’s disease. Phys Ther., 74(1); 61-70.
Smania N, Corato E, Tinazzi M, Stanzani C, Fiaschi A, Girardi P, Gandolfi M. (2010 Nov-Dec). Effect of balance training on postural instability in patients with idiopathic Parkinson’s disease. Neuro-rehabil Neural Repair.,24(9); 826-34.
Qutubuddin AA, Pegg PO, Cifu DX, Brown R, McNamee S, Carne W. (2005 Apr). Validating the Berg Balance Scale for patients with Parkinson’s disease: a key to rehabilitation evaluation.Arch Phys Med Rehabil., 86(4); 789-92.
Hirsch MA, Toole T, Maitland CG, Rider RA. (2003 Aug). The effects of balance training and high-intensity resistance training on persons with idiopathic Parkinson’s disease. Arch Phys Med Rehabil., 84(8); 1109-17.
Inkster LM1, Eng JJ, MacIntyre DL, Stoessl AJ. (2003 Feb). Leg muscle strength is reduced in Parkinson’s disease and relates to the ability to rise from a chair. MovDisord. 18(2); 157-62.
Scandalis , T , et al. (2001).Resistance Training and Gait function in patients with Parkinson’s disease. Am J Phys Med Rehabil. 80; 38.
Glendinning, D: (2001). A rationale for strength training in patients with Parkinson’s disease. Neurology report (now JNPT); 21; 132.
Citation: Purnima Singh, Panomootil Blessy Varghese (2020).effects of balance training and strengthening exercises on individuals with idiopathic parkinson’s disease, ijmaes; 6 (3); 799-810.
2Faculty of Pharmacy,
AIMST University, Semeling, 08100 Bedong, Kedah Darul Aman, Malaysia
3Professor,Faculty of
Physiotherapy, DR.MGR.Educational and Research Institute, Deemed to be
University, Velappanchavadi, Chennai, India
Corresponding Author:1*Professor, Rajarajeswari College of Physiotherapy, Kambipura, Mysore Road, Bangalore, Karnataka, India, Mail id: vijayrrc@yahoo.com
ABSTRACT
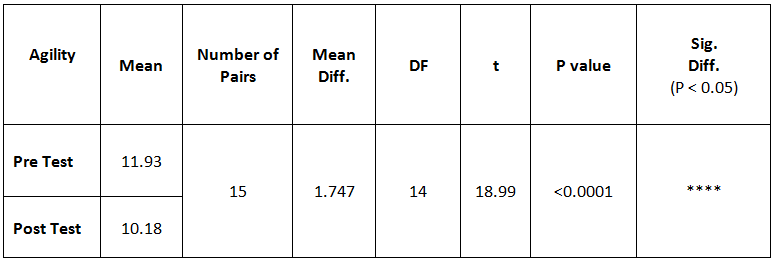
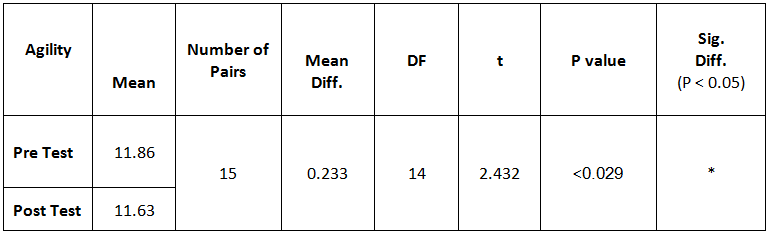
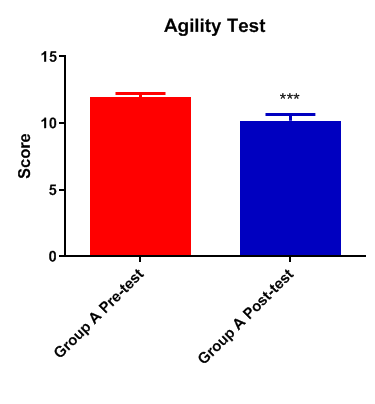
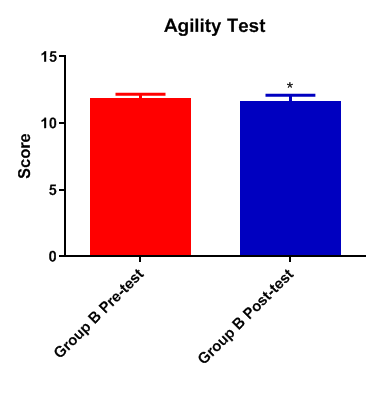
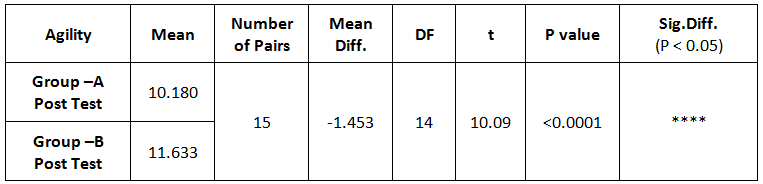
Background and objectives: The Cricket is known as “the gentleman’s game” which places physical demand on the players. This demand creates lot of stress on muscles leading to injuries if they lack fitness. Star excursion balance training (SEBT) programme forms a core component of the training among young men cricket players in improving their agility. The less research evidence on 6 weeks of SEBT program has led to design this study to identify whether there is any effect on agility in enhancing the physical performance and prevent the occurrence of injuries among young men cricket players. Method: This was a comparative experimental study conducted on thirty young men cricket players (n=30) of age group ranged between 18 and 22 years. They were randomly selected for two groups as star excursion balance training (SEBT), Group A and conventional exercises training (CET), Group B with fifteen (n=15) subjects in each group. The Group A underwent Star excursion balance training programme and the Group B underwent conventional exercises training programme. The training for both groups was administered for 6 weeks with three sessions per week. Result: The result shows that there is significant improvement with P<0.0001 in agility T test score on performance in Group A and significant improvements in Group B, with P<0.0290. Comparative study between the group shows significant difference between the groups with P<0.0001, with mean difference of 0.060 and -1.453 respectively on Group A and B. So Group A is better than Group B. Conclusion: Six weeks of star excursion balance training programme can be recommended for young men cricket players to improve the agility in enhancing their physical performance and preventing injuries.
Keywords: Star excursion balance training, Agility T Test, Agility, Young men cricket players.
Received on 14th August 2020, Revised on 24th August 2020, Accepted on 31st August 2020, DOI:10.36678/IJMAES.2020.V06I03.003
INTRODUCTION
Cricket is one
of the popular and oldest non-contact bat and ball sport which engages the
players in running, throwing and catching during bowling, fielding, wicket
keeping and batting. This leads to overuse and impact injuries to the upper
limb, lower limb, head and back1. Cricket is one of the sports
characterized by many of the basic and variable skills, which is played in
several versions, such as long format and short format. The long format is
played over for five consecutive days as test matches and the short format
includes one day and 20-20 matches.
The demand on
the players due to various formats of cricket sport causes physiological
overload, which depends heavily on the player’s ability to move quickly and
powerfully. This greater stress on the cricketers demands an extreme physical
fitness, not only for the performance, but also to prevent injuries. These
larger demands are the reflections of frequent touring for the test matches,
one day matches and 20-20 matches per season. The sprinting and turning within
the wickets , running-up and delivering the ball when fast bowling , causes
rapid acceleration and deceleration load on the lower limb musculature2,3.
The cause of stress in cricket players is due to sudden starting and stopping
nature of sprinting between the wickets, fast bowling and fielding which
contributes to onset of fatigue in overtime, resulting with impact of negative
performance and increase in the risk of injuries. These intermittent activity
in cricketers during bowling, fielding and batting, places them on demand on
the physiological and neuromuscular system4,5.
The bat and ball
sport led the players to, overuse and impact injuries , at various anatomical
sites with the region most vulnerable to injury accounting with 44.9 % in the
lower limb, followed by upper limb at 29.4%, the trunk at 20.0% and head and
neck at 5.7%. The range of injuries in cricketers varied between 22.8 % to 50.0
% in lower limb among other anatomical sites of injuries6,7.The
functional testing of balance and proprioception, strength, range of motion and
agility determines whether a patient is able to return to play following an
ankle injury8.
Due to the complex
skills and rules in cricket, the players require a good physical fitness,
skills and efficient strategies for an effective motor task performance in
maintaining the body positions during sudden location and directional changes
in activities of acceleration and deceleration which demands good balance. This
task performance of sudden acceleration and deceleration rapidly with good
balance and the ability to change direction or body position rapidly and to
proceed with another movement is the ability defined as “Agility”9.
The agility is the ability of a player to change position in space or to change
direction quickly and effectively. And it is thought to be a reinforcement of
programming through neuromuscular conditioning and neural adaptation of muscle
spindle, golgi tendon organ and joint Proprioceptors10. The agility
is a complex ability depending on coordination, mobility of joint system,
dynamic balance, strength and speed. The balance training is effective in
improving static postural sway and dynamic balance through neuromuscular
control and performance enhancement11. This ability to enhance the
maintenance or control of body positions while quickly changing the direction
during a series of movements should improve “Agility”12.
The injuries can
be an adverse outcome of participation in sports and recreational activities.
The impact of injuries during these activities is most associated with cricket
players at a value of 242/ 1000 injuries among other sport players. And it is
recommended for injury prevention program, aiming at team ball sports (Cricket,
soccer and netball) because of their comparatively high rate of both, overall
and significant injury13.
Training with
rapid stretching of a muscle (eccentric action) immediately followed by a
concentric or shortening action of the same muscle produces more force than the
force produced by a concentric action alonebecause of the stored
elastic energy within the muscle14, 15. The components of stopping,
starting and changing direction in the training programs assists in developing
agility10,16,17. Training the
above components through Star Excursion Balance Training (SEBT) among young men
cricket players may be effective in improving the agility by increasing the
balance and control of body positions during movements by neuromuscular
conditioning and neural adaptation of the Proprioceptors10. But
there are less scientific evidences in proving its effect. Therefore the
purpose of this study is to determine whether there is any effect of SEBT
program for 6 weeks on Agility among young men cricket players.
METHODS
This was an
experimental and comparative study. Young men cricket players between the age
group of 18 to 22 years, who were undergoing professional cricket training
volunteered to participate in this study from the cricket academy at Bangalore.
They were screened for selection criteria to include in this study. A total of 30 participants who satisfied the inclusion criteria were
incorporated for the study after explaining the procedure and obtaining the
signed written consent form. This study was a randomized controlled trial and
the selected subjects were randomly allocated into two groups by paper and chit
system, Group A (N=15) the training group and Group B (N=15) the control group.
Inclusion criteria: Young
men cricket players of age group between 18 – 22 years, participants with
agility T score of more than 11.5 seconds, and subjects with stroke balance
stand test score of more than 40 seconds.
Exclusion criteria: Subjects
withany limb length discrepancy,
spinal or lower limb deformities, history of surgery of spine or lower limb or
upper limb, history of injury of spine or lower limb or upper limb, history of
neurological dysfunction in the lower limb or upper limb, vestibular
dysfunction and any visual impairment were excluded from the study.
Materials: Measuring tape, White athletic tape, Four (4)
agility cones, Stop watch, Paper and pencil were the materials used to conduct
this study.
Measurement
tools:
Agility T test used to measure the performance of cricket players
Intervention: Star excursion balance
training (SEBT) and Conventional
exercises training (CET).
Procedures:
This study was
designed with a pre and post intervention randomized control trial. Those
subjects in training group (Group A) received star excursion balance training
(SEBT) programme, while the subject in control group (Group B) received conventional exercises training program. The subject in both the groups were permitted to continue
their regular cricket practice, but were not permitted to start any other
extremity strengthening and balance training program during this course of
study. Rather, they were permitted to perform only the approved training
program of this study.
The subjects in
both the groups were instructed to come in shorts and barefoot, one week before
commencement of the study. They were explained and demonstrated to learn about
the variables which have to be executed in the study and were made to practice
in a correct manner. The Agility T-test was used as an outcome measure for
Agility. On day one of the study, subjects in both the groups underwent a
baseline testing as a pretest score and then a posttest score was measured on
the last day of 6th week.
Dependent
Variable Testing:
The
agility T test is a reliable and valid measure for leg speed and secondarily of
leg power and agility in lower limb20. The outcome measure was
measured using agility T test. Before starting the test, four cones were taken
and arranged on the track in the shape of “T”. The four cones A, B, C, & D
were arranged perpendicular in the shape of “T”. The cones A and B were
arranged perpendicular to Cones C & D. The point between Cone A and B was
arranged in 9.14 meters and the point of arrangement between Cone C and D from
Cone B was 4.57 meters. After the arrangement of cones the subject was made to
stand with both the feet behind the starting point (Cone A) facing towards Cone
– B. Then on getting a start signal and by starting the stopwatch, the subject
ran from Cone – A towards Cone – B and touched the base of cone – B with the
right hand. After touching Cone –B the subject ran towards Cone – C and touched
the base of Cone – C with the left hand. Then the subject shuffled towards Cone
– D to touch its base with the right hand. After this moment the subject
shuffled back towards Cone –B and touched its base with the left hand followed
by running towards Cone – A to finish. After crossing Cone – A, immediately the
stopwatch was stopped and the total duration of time taken to complete the run
between the cones was documented.
Group A: Star
Excursion Balance Training (SEBT) group:
Prior
to starting of the training program, the preparation for Star Excursion Balance
training was performed, initially by selecting a flat and non-slippery surface.
Then Four (4) strips of white athletic tapes of 6 feet in length were cut. In
order to form the star grid shape on the floor, two strip were pasted in the
form of “+” and the other two strips pasted across on the top in the form of
“x”. It has to be assured that the stripes pasted are arranged to each other
from a center point at angle of 45 degrees with each other. This star shaped
grid arrangement involves a series of single-leg squats with the stance limb
and a dynamic maximal reach using the non-stance limb to touch a point as far
as possible along eight designated lines radiating from a central point at an
angle of 45°18,19.
The subjects in
the training group were informed to come in shorts and barefoot. To start with
each training session the subjects were made to perform 3-minute of warm up
followed by Star excursion balance training (SEBT) and conventional exercise
training continued with 2-minute of cool down The warm up and cool down
included dynamic movements and static stretches.
The
subjects from the SEBT group performed the Star Excursion Balance training
initially by standing in bilateral stance with barefoot on the middle of the
star grid. The weight bearing leg is the stance limb and the unsupported leg is
the reaching limb. Then the subjects were instructed to balance their body
weight on the stance limb on the middle of the star grid where the strips of
tapes are placed at an angle of 45 degrees. By keeping the hands on the pelvis,
the subjects were made to reach a distance of 2 feet marked on the tape in all
the 8 directional tape positions with the tip of toe of the reaching limb
without shifting weight on the reaching limb. The 8 directional tape positions
are anterior, anteromedial, medial, posteromedial, posterior, posterolateral,
lateral, anterolateral. After each directional reach the subject returns the
reaching limb to the start position at the middle of the grid, resuming a
stable bilateral stance with 3 seconds of rest between each tape direction. The
training with SEBT program was done with 12 rounds in clockwise and 12 rounds
in counterclockwise reach. During each session, the subjects were given with a
period of 30 seconds rest, to perform the same exercises by changing the stance
limb and the reaching limb. The training was administered for 6 weeks with the
frequency of three sessions per week.
Group B:
Conventional Exercises Training (CET) group:
The subject in
the conventional exercise training group performed the following exercises with
2 sets of 10 repetitions per day under the supervision. To start with each
training session the subjects were made to perform 3-minute of warm up follow
by Conventional Exercises Training
(CET) continued with 2-minute of cool down. The warm up and cool down
included dynamic movements and static stretches.
Two legs straight knees heel
raise – Facing the wall: The
subject was made to stand facing the wall with both knees in extended position.
Both the feet’s were placed away by shoulder width and in front of a wall away
by 6 inches with hands place on the wall at the level of the shoulder. The
subject was instructed to raise the heel up on toes as high as possible and
hold for a period of 10 seconds and relax for 10 seconds.
Two legs bent knees heel raise
– Facing the wall: The
subject was made to stand facing the wall with both knees in mild flexed
position by placing the patella on the wall. Both the feet’s were placed away
by shoulder width and in front of a wall away by 6 inches with hands place on
the wall at the level of the shoulder. The subject was instructed to raise the
heel up on toes as high as possible and hold for a period of 10 seconds and
relax for 10 seconds.
Two legs straight knees heel
raise- Facing away the wall: The subject was made to stand facing away from the wall with both knees
in extended position. Both the feet’s were placed away by shoulder width and in
front of a wall away by 12 inches. The subject was instructed to lean on the
wall with the upper back and head supported and to raise the heel up on toes as
high as possible while pushing the shoulder back into the wall and hold the
heel raise for a period of 10 seconds and relax for 10 seconds.
Two legs bent knees heel raise-
Facing away the wall: The
subject was made to stand facing away from the wall with both knees in mild
flexed position both the feet’s were placed away by shoulder width and in front
of a wall away by 12 inches. The subject
was instructed to lean on the wall with the upper back and head supported and
to raise the heel up on toes as high as possible while pushing the shoulder
back into the wall and hold the heel raise for a period of 10 seconds and relax
for 10 seconds.
One leg straight knee heel
raise – Facing the wall: The
subject was made to stand in unilateral stance facing the wall with the stance
knee in extended position and foot in front of a wall away by 6 inches.
Opposite foot is kept unsupported with hands place on the wall at the level of
the shoulder. The subject was instructed to raise the stance heel up on toes as
high as possible and hold for a period of 10 seconds and relax for 10 seconds.
One leg bent knees heel raise –
Facing the wall: The
subject was made to stand in unilateral stance facing the wall with the stance
knee in mild flexed position by placing the patella on the wall and foot in
front of a wall away by 6 inches. Opposite foot is kept unsupported with hands
place on the wall at the level of the shoulder. The subject was instructed to
raise the heel up on toes as high as possible and hold for a period of 10 seconds
and relax for 10 seconds.
One leg straight knees heel
raise- Facing away the wall: The subject was made to stand in unilateral stance facing away from the
wall with the stance knee in extended position and feet in front of a wall away
by 12 inches. Opposite foot is kept unsupported. The subject was instructed to
lean on the wall with the upper back and head supported and to raise the heel
up on toes as high as possible while pushing the shoulder back into the wall
and hold the heel raise for a period of 10 seconds and relax for 10 seconds.
One leg bent knees heel raise-
Facing away the wall: The
subject was made to stand in unilateral stance facing away from the wall with
the stance knee in mild flexed position and feet in front of a wall away by 12
inches. Opposite foot is kept unsupported. Lean on the wall with the upper back
and head supported. The subject was instructed to lean on the wall with the
upper back and head supported and to raise the heel up on toes as high as
possible while pushing the shoulder back into the wall and hold the heel raise
for a period of 10 seconds and relax for 10 seconds.
Forward and Reverse lunge: The subject was made to stand on the ground with your
feet hip-width apart from each other. The both hands of the subject were on the
side by holding 1kg dumbbells. Then the subject moved the left leg 1 foot
forward simultaneously lowering the body until both the front and back legs
comes to 90 degrees angle. Here it was instructed that the left leg should not
go in front of your toes and at the same time, and also the back leg should not
bend down the floor to touch it. Hold this position for 2-3 seconds. Rise above
and take your left leg back to complete one rep. Repeat the same with the Right
leg. To perform reverse lunges the subject was made to take the foot backward
and then bend both legs down to get into a 90 degree angle. Repeat the same
with the opposite leg.
RESULTS
The results of this study were
analyzed in terms of the total time taken to complete the agility “T” test as
an outcome measure indicated by improvement of agility by the enhancement of
physical performance and thereby preventing injuries through efficient leg
power, balance and speed of activity in the lower limb. The comparison was done
between pretest and posttest data.
A
total of 30 young male cricket players with age group between 18 to 22 years
were included into two groups of SEBT group and CET group with 15 subjects in
each. So as to evaluate the effectiveness of agility under this present study,
both the intra group and inter group analysis (Group A and Group B) was done
among the subjects who underwent star excursion balance training programme
(Group A) and conventional exercises programme (Group B).
Within group analysis the improvement in agility T test score value for Group A on agility has reduced with mean difference of 1.747, with significant difference of P value > 0.0001, while in Group B agility has reduced with mean difference of 0.233, with significant difference of P value < 0.029.
Table 1: Statistical analysis of Agility T test score Values in improving agility among subjects within Group A (SEBT group) Table 2: Statistical analysis of Agility T test score Values in improving agility among subjects within Group B (CET group) Graph 1: Presentation of the Agility T test score Values in the improvement of agility in subjects within Group A Graph 2: Presentation of Agility T test score Values in the improvement of agility in subjects within the Group B
In between group Comparison of Group A and Group B, it has shown no significant difference on the pre- test agility score value with mean difference of 0.06000 and P value of < 0.561. However there was high significant difference in the improvement of post-test agility score value on agility with mean difference of -1.453 and P value of < 0.0001.
Table 3: Statistical analysis of pre Agility T test score values on agility in subjects between Group A and B
The above table 3 shows no significant difference in the pre-test agility score on agility among subjects between Group A and B with P value < 0.5914.
Graph 3: Presentation of Agility T test score on agility between pre-test score among subjects between Group A and B Table 4: Statistical analysis of Agility T test score in the improvement of agility between post-test score among subjects between Group A and B
The above table 4 shows statistically significant difference in the post-test agility score in the improvement of agility among subjects between Group A and B with P value < 0.0001.
Graph 4: Presentation of Agility T test score Values in the improvement of agility between post-test score value of Group A and B
DISCUSSION
This present
study was conducted to compare the effects of star excursion balance training
(SEBT) programme versus conventional exercises training programme, in improving
agility among young men cricket players. Our current study demonstrated that
star excursion balance training (SEBT) administered for 6 weeks with the
frequency of three sessions per week has showed statistical significant result
in SEBT group and CET group on agility. On comparison between the groups, there
was no statistical significant difference between the pre-test score values of
agility T test but there was significant difference in effectiveness on agility
between the post test score values between the groups. Here it is demonstrated
with more effective on the mean difference among the SEBT group when compare
with the mean difference on CET group.
This agility
T-test is a reliable test for agility which is stated by Pauole et al., (2000)20
that, the agility T-test appears to be a reliable and valid measure of leg
speed, leg power and agility which can be benefited as a field test to assess
the lower extremity movement in ground based sports and discriminate between
low and high levels of sport participation and also supported by Hermassi et al., (2011)21
concluded that total time of agility T-test is significantly associated with
explosive muscular power of lower limbs, vertical jump performance and
acceleration ability and its result suggest total time of agility T-test has an
unique fitness quality to considered as field test that is relevant to be used
in training prescription and talent identification.
Our
data confirmed that there is improvement on the agility in the subjects of SEBT
group through 6 weeks of star excursion balance training programme and less
significant improvement on the agility with conventional exercise training
programme as measured through Agility T test, which is similar to the
previously reported finding by Rogers
et al., (2012)22 stating that agility and perturbation are
effective than resistance training to reduce and improve function postural
control. The Inter group analysis of our study has shown with statistical significance, in improving
the agility between the groups with more mean difference in SEBT group. This significant finding suggests
that by performing star excursion balance training
programme, there is associated contribution of training strength, training ability of
balance, training ability of dynamic performance and training compressive
loading over the joint in improving the functional performance with good Static
and dynamic balance, efficient and quick change in direction of movement, skill
to quickly stops and resume the movements which are the core components of
agility.
The lesser improvement in agility
among the subject in the conventional exercise training programme group may be
due to less sensory input programme by dynamic
loading on the limb while performing the conventional exercises. We therefore
hypothesis that star excursion balance training (SEBT) programme is better than conventional exercises training programme (CET) and may contribute in
improving agility among young men cricket players for an efficient performance and prevention
of injuries. Studies have adduced evidence by Rogers,
Rogers, & Takeshima, 200523
who examined the effect of the ability to balance and stated that this effect of
balance is entirely depended on sensory input and muscle strength .The sensory
input occurs through visual, vestibular, and somatosensory systems. The visual
system contributes to balance, by providing information about the environment,
location, and the direction and speed of movement within the environment,
whereas the vestibular system, give information about the position and movement
of the head. The somatosensory system rules the position of the body and limb
through information from receptors and muscle receptors and is similarly
supported by Hasegawa et.al (2010)24
stated that the mechanoreceptors respond to any compression or tension during
of loading over the limb and the afferent impulse are carried from periphery to
central nervous system via spinal level, were it generates motor activity for
protective mechanism of the respective joint.
These findings are similar to the
findings of Matthews P B (1982)25
that proprioception is used for the regulation of total posture (postural
equilibrium) and segmental posture (joint stability), as well as initiating
several conscious peripheral sensations (“muscle senses”). This “muscle sense”
sensations correspond to the contemporary terms joint position sense (posture of segment), kinesthesia (active and
passive), and the sense of resistance or heaviness. Thus, proprioception
correctly describes afferent information arising from internal peripheral areas
of the body that contribute to postural control, joint stability, and several
conscious sensations.
Furthermore, the statistical significance in star excursion balance training (SEBT) group on agility in our study could probably be due to the improvement in the components of postural control strategies. Indeed it has shown significant difference in improvement on agility among SEBT group rather than CET group. Similarly, Chiung-Ling Chen (2014)26 stated that, in the initial phase, rotational perturbation induced earlier ankle movement and in faster and larger vertical center of mass displacement, while translational and forward/toe up perturbations induced larger head and trunk angular change and faster and larger horizontal center of mass displacement. In the reversal phase, balance reaction was attained by multi-joint movements. Translational and forward/toe up perturbations that induced larger upper body instability evoked faster muscle activation as well as faster and larger hip or knee joint movements.
Balance training, the amplitude, velocity and direction of perturbations can be varied to practice in-place or stepping reaction and normal strategy used to respond to an external perturbation can be trained to the patients to offer visions for selecting appropriate support surface perturbations for assessment and for designing methods for training postural control. These findings are similar to findings by Ogaya (2011)27that balance training in elderly people using wobble boards is effective to improve their standing balance by improving their standing time on a wobble board, on a balance mat, and maximum displacement distance of anterior-posterior center of pressure by which they frequently control their center of gravity and maintain a standing posture on unstable surface conditions. And the training on tilt board or uneven surfaces improves the ability to stabilize in an upright stance position. These postural exercises strategy restores body’s center of mass to stabilize through body movement centered primarily on the ankle joints and has significant impact on functional improvements in knee joint.
The result of this study was in compliance with the
finding of the study conducted by Sporis
et. al.,28 stated that agility training can be used
effectively as a training method for improving explosive leg power and dynamic
athletic performance. Hence in addition to the well-known method of training
such as resistance training and plyometric training, strength and conditioning,
athletes may incorporate agility training as well into an overall conditioning
programme of athletes striving to achieve a high level of explosive leg power
and dynamic performance. This is supported by Miller et al., 200629 that agility is the ability which
makes it possible for an athlete to change direction, make quick stops and
perform fast, smooth, efficient and repetitive movements and similarly a study
conducted by Mayhew, et al. (1989)30
states that agility is highly dependent on coordination and movement control
but apart from coordination there is a substantial number of factors that
affect the level of agility such as mobility of joints, dynamic balance, power
and flexibility, level of energy resources, strength, speed and optimal
biomechanical structure of movement.
In an another study conducted by Islam (2004)31, analyzed the effect of an exercise training program challenging the sensory and muscle systems in older adults on Static balance, dynamic balance, maximum excursion, and strength and concluded that there is significant improvement in balance, lower body strength and function. Boeer (2010)32 assessed the changes in balance capacities by recording the total center of pressure excursion with 1-legged stance on the oscillatory Posturomed platform after a 12-week sensory-motor training program for older adults with osteoarthritis and recommended that this training program improves balance abilities and reactions to sudden disturbances and displacements.
Ethical
clearance: The ethical approval was granted by the
ethical committees of the RRF cricket academy, Bangalore.
Conflict of interest: There was no conflict of
interest to conduct this study.
Fund for the
study: It was
self-financed study.
CONCLUSION
The
results of this study indicates that there is improvement on agility among
young cricket players with Star excursion balance training (SEBT) program as
assessed by the level of dynamic performance and functional tasks in different
positions through agility T test. Ultimately, our study stresses the importance
of improving the agility through efficient postural swaying strategies, rapid
change of direction, explosive leg power, quick stopping and resuming smooth
and repetitive movements.
Furthermore,
this improvement in agility through SEBT can be a beneficial training programme
in demanding the physiological and neuromuscular system among young men cricket
players, in improving leg power, balance and speed in lower limb with the
ability to sprint suddenly, quickly, powerfully and stop suddenly between the
wickets with less impact on the risk of injuries. Therefore, conducting a
planned SEBT programme can be recommended for cricket players to improve their
agility for an efficient performance and less impact on the risk of injuries.
REFERENCES
Dinshaw N. Pardiwala, Nandan N. Rao, Ankit V. Varshney. (2017). Injuries in Cricket. Sports Health.10:217-222.
Noakes, TD. & Durandt, JJ. (2000). Physiological requirements of cricket. Journal of Sports Sciences, 18:919-929.
Christie, CJ, Barford, G., Sheppard, B. (2011). Concentric and eccentric strength changes in the lower limb musculature following repeated sprints between the wickets. Proceedings of the 4th World Congress on Science and Medicine in Cricket. 31 March–01 April, 2011: 82.
Davis .R, Du-Randt.R, Venter D, Stretch R.Cricket. (2008). Nature and incidence of fast bowling injuries at an elite junior level and associated risk factors. South African journal of sports medicine. 20(4): 115-119.
Bartlett RM. (2003). The science and medicine of cricket: An overview and update. Journal of Sports Science. 21: 733-752.
Stretch RA. (1993). The incidence and nature of injuries in first league and provincial cricketers. South African medical journal. 3: 339-342.
Stretch R.A. (2003). Cricket injuries: A longitudinal study of the native of injuries in south Africa cricketers. British journal of sports medicine. 37: 250-253.
Clanton, T. O., Matheny, L. M., Jarvis, H. C., & Jeronimus, A. B. (2012). Return to play in athletes following ankle injuries. Sports Health, 4(6), 471-474.
Gabbard, Carl, Leblance, Elizabeth and Susan, (1987). Physical education for children. New Jersey: Prentice Hall, Inc. p. 120-124.
Chaig.BW. (2004). What is the scientific basis of speed and agility? Strength and conditioning journal. 26 (3): 13-14.
Zech, A., Hübscher, M., Vogt, L., Banzer, W., Hänsel, F., & Pfeifer, K. (2010). Balance training for neuromuscular control and performance enhancement: a systematic review. Journal of athletic training, 45(4), 392-403.
Twist P.W., Benicky D. (1996).Conditioning lateral movements for multi-sport athletes: Practical strength and quickness drills. Strength and Conditioning 18(5):10-19
Finch, C., & Cassell, E. (2006). The public health impact of injury during sport and active recreation. Journal of Science and Medicine in Sport, 9(6), 490-497.
Baechle T.R., Earle R.W. (2000) Essentials of strength training and conditioning. 2nd edition Champaign, IL: National Strength and Conditioning Association.
Miller M.G., Berry D.C., Bullard S., Gilders R. (2002). Comparisons of land-based and aquatic-based plyometric programs during an 8-week training period. Journal of Sports Rehabilitation 11, 269-283.
Miller, J.M., Hilbert, S.C. and Brown, L.E. (2001). Speed, quickness, and agility training for senior tennis players. Strength and Conditioning 23(5): 62-66.
Young W.B., McDowell M.H., Scarlett B.J. (2001). Specificity of spring and agility training methods. Journal of Strength and Conditioning Research 15: 315-319.
Gray, G. W. (1995). Lower extremity functional profile. Wynn Marketing, Incorporated.
Gribble PA. (2003). The Star Excursion Balance Test as a measurement tool. Athl Ther Today. 8(2):46–47.
Pauole K, Madole K, Garhammer J, Lacourse M, and Rozenek R. (2000). Reliability and validity of the T-test as a measure of agility, leg power, and leg speed in college-aged men and women. J Strength Cond Res 14: 443–450,
Hermassi, S., Fadhloun, M., Chelly, M. S., & Bensbaa, A. (2011). Relationship between agility T-test and physical fitness measures as indicators of performance in elite adolescent handball players. Pedagogics, Psychology, Medical-Biological Problems of Physical Training and Sports. 1 (5)125-130.
Rogers, M. W., Tamulevicius, N., Semple, S. J., & Krkeljas, Z. (2012). Efficacy of home-based kinesthesia, balance & agility exercise training among persons with symptomatic knee osteoarthritis. Journal of sports science & medicine, 11(4), 751.
Rogers, M.E., Rogers, N.L., & Takeshima, N. (2005). Balance training in older adults. Journal of Aging and Health. 1: 475–486.
Hasegawa, R., Islam, M. M., Nasu, E., Tomiyama, N., Lee, S. C., Koizumi, D., & Takeshima, N. (2010). Effects of combined balance and resistance exercise on reducing knee pain in community-dwelling older adults. Physical & Occupational Therapy in Geriatrics, 28(1), 44-56.
Matthews P B. (1982) .Where does Sherrington’s “muscular sense” originate? Muscles, joints, corollary discharges? Annual Review of Neurosciences. 5:189–218.
Chiung-Ling Chen, Shu-Zon Lou, Hong-Wen Wu, Shyi-Kuen Wu, Kwok-Tak Yeung & Fong-Chin Su. (2014). Effects of the type and direction of support surface perturbation on postural responses.50,2-12.
Ogaya, S., Ikezoe, T., Soda, N., & Ichihashi, N. (2011). Effects of balance training using wobble boards in the elderly. The Journal of Strength & Conditioning Research, 25(9), 2616-2622.
Sporiš, G., Milanović, L., Jukić, I., Omrčen, D., & Sampedro Molinuevo, J. (2010). The effect of agility training on athletic power performance. Kinesiology: international journal of fundamental and applied kinesiology, 42(1), 65-72.
Miller, M.G., Herniman, J.J., Ricard, M.D., Cheatham, C.C., & Michael, T.J. (2006). The effects of a 6-week training program on agility. Journal of Sports Science and Medicine. 5: 459-465.
Mayhew, J.L., Piper, F.C., Schwegler, T.M., & Ball, T.E. (1989). Contributions of speed, agility and body compositionto anaerobic power measurements in college football players. Journal of Applied Sports Science Research. 3(4): 101-106.
Islam, M. M., Nasu, E., Rogers, M. E., Koizumi, D., Rogers, N. L., & Takeshima, N. (2004). Effects of combined sensory and muscular training on balance in Japanese older adults. Preventive medicine, 39(6), 1148-1155.
Boeer, J., Mueller, O., Krauss, I., Haupt, G., Axmann, D., & Horstmann, T. (2010). Effects of a sensory-motor exercise program for older adults with osteoarthritis or prosthesis of the hip using measurements made by the Posturomed oscillatory platform. Journal of geriatric physical therapy, 33(1), 10-15.
Citation: Pushparaj Vijayakumar, Rajavel Varatharajan, Jibi Paul (2020). Effect of star excursion balance training program on agility among young men cricket players , ijmaes; 6 (3); 784-798.
1MSc Nursing Candidate, College of
Nursing, Dr. M.G.R Educational and Research Institute, ACS Medical College and
Hospital Campus, Maduravoil, Chennai, Tamil Nadu, India
3Associate Professor, College of Nursing, Dr. M.G.R Educational and Research Institute, ACS Medical College and Hospital Campus, Maduravoil, Chennai, Tamil Nadu, India
Corresponding Author:
2*Vice Principal & Research Scientist, College of Nursing, Dr. M.G.R Educational and Research Institute, ACS Medical College and Hospital Campus, Maduravoil, Chennai, Tamil Nadu, India Mail id: hepsibah.srs@drmgrdu.ac.in
ABSTRACT
Introduction: Practice of mothers is crucial to seek prompt medical attention especially for their under five years of aged children and it reduces the mortality rate of the children with severe acute respiratory tract infection. The aim of this study was to determine health care seeking practice of the mothers and to analyze the factors influencing mothers choice in seeking care for there under five children. Methodology: A cross sectional study was conducted at A.C.S Medical College at the three associated community health centers in Nasarathpettai, Meppur, Meppurthangal located at in Chennai. 251 mothers of under five children participated in the study. Result: The study revealed that only 61.59% of children where promptly taken to the used to GP clinic for acute respiratory tract infection and 48.34% children were treated with home remedy, 29.14% used to take to general physician. It was found that 19.21% used old prescription given for the same child and 7.95% mothers seek over the counter drugs from medical shop. Conclusion: Practice of health seeking behavior for acute respiratory infection among mothers of under five years children cannot be under estimated. It is the responsibility of the nurses and other healthcare people to create understanding on the management of acute respiratory tract infection to reduce further hazardous complication related to acute respiratory tract infection.
Keywords: Under five children, acute respiratory infection, practice of mother, health care
Received on 12th August 2020, Revised on 22nd August 2020, Accepted on 30th August 2020, DOI:10.36678/IJMAES.2020.V06I03.002
INTRODUCTION
Acute respiratory infection (ARI) causes 20 %
of the mortality among under five children1. However, ARI can be
preventable and the intensity of the infection can be reduced if prompt medical
care is sorted. ARIs causes more death and disease prevalence in children of
under five years. More studies are proving that burden of ARI is present in
both urban and rural area there are affect the low class and high class
children’s in equally.
In the world under five
deaths due to acute respiratory infection is the fifth leading cause. Globally,
about 2 to six million (16%) ARI deaths are occurring in under five children.
In India 1, 58,176 under five children’s are dies in acute respiratory infection
(NHFWS 2018). The medical team gives priority care for children affected with
ARI especially under five children. Because most of them under five children
died in ARI disease burden is high. In India the major morbidity and mortality
of children under five years deaths is caused by Acute Respiratory Tract
infection. In India children under five years death due to acute respiratory
infection in the year of 2018 is 882,000 which is 37 per 1000 live births 2, 3.
Acute respiratory infection is divided in to two category upper
respiratory infection and lower respiratory infection. The upper respiratory
indicates from the nose to larynx associated with the paranasal. The lower
respiratory tract is at end of the upper respiratory to alveoli (trachea,
bronchi, bronchioles and alveoli). Many studies have reported that appropriate
care seeking behaviors is the is the best practice. Prompt care seeking behavior
is reducing the 20% of the child death rates due to acute respiratory
tract infection. The mother and other to give a proper time care that should be
reduce the child mortality rate.
Objectives
of the Study : To assess the care seeking behaviour and practice of mothers for children
with acute respiratory infection, also to associate the socio-demographic
variables with mother’s care seeking behaviour
on under Five children with Acute Respiratory Infection
METHODOLOGY AND METHODS
This was a community based cross–
sectional study carried out in the three rural community health centers namely
Nasarephpettai, Meppur and Meppurthangal which are affiliated to the tertiary
level hospital at the local regions of Chennai in the state of Tamil Nadu,
India. These Community health centers are located across 10 km radius away from
ACS medical college. The community health centers
affiliated to the tertiary level hospital are
also located
within 10 km between metropolitan regions of Chennai to rural land.
The setting has been chosen on the basis of feasibility of adequate sample and
cooperation. Population is the entire aggregation of cases which meet the
designated set of criteria (Polit and Beck 2004).
The overall population of the total
Nasarathaipettai population is 8409 under five children population 156. The
Meppur and Meppurthangkal total population is 2182 under five children 83 the
entire aggregation of cases which meet the designated set of criteria.
All the children, under five years of
age belonging to the study area were included as study subjects. The mothers of
the children were the respondents. Care was taken to ensure that the family of
the particular under five was a permanent resident of the area and not a
frequent migrant. Those who could not be contacted during the first visit were
given two more visits. The research protocol was approved by the ethical
committee at the ACS Medical College and Hospital and informed consent was
obtained from each subject prior to inclusion in the study. A predesigned and
pretested structured questionnaire was used to collect the data. The mothers
were interviewed for detail information regarding socio-demographic details and
acute illnesses especially ARI in last two weeks prior to the visit as these
are the main contributors to child morbidity. The health care seeking behavior
for such diseases including the place and person consulted for disease, the
treatment availed, the money spent and the distance travelled were also
enquired. Records were analyzed whenever available. Proportions and percentages
were used for analysis.
Sample Size Calculation
4pq/L2 = 90 (+10 – 20%)
(Prevalence (6%), q= 1-p, L = allowable
error (.05)
The Study sample comprised of 2512 under five mothers
Sampling Technique: Purposive sampling technique was used to select the sample
Selection Criteria: The Study includes mothers of less than five children; Mother’s who have already treated the acute respiratory infection for their children, Mother’s who are willing to participate and Mother’s who can speak and write Tamil and English.
Exclusion Criteria: Pilot study samples and children with other genetic problem and comorbidity.
RESULT
The analysis is a process of
organizing and synthesizing the data in such a way that the research questions
can be answered and the hypotheses are tested. The analysis and interpretation of the data collected from 251
mothers of under five children to assess the care seeking behaivour of mothers
of less than five children with acute respiratory infection. The data was
organized, tabulated and analyzed according to the objectives. Data analysis begins with description that
applies to the study in which the data are numerical with some concepts.
Descriptive statistics allows the researcher to organize the data and to
examine the quantum of information and inferential statistics is used to
determine the relationship.
Organization
of the Data: Data organized under the following sections.
Section A:
Description of the demographic
variables of mothers of under five
children.
Section B:
Assessment of care seeking behaviour
of mothers of less than five children with acute respiratory infection.
Section C:
Association of care seeking behaviour
with selected demographic variables.
Section A:
Description of the demographic variables of mothers of less than five children.
Table 1: Demographic variables of mothers of under five children (Continue…) Table 1: Demographic variables of mothers of under five children (Continue…) Table 1: Demographic variables of mothers of under five children
The table 1 shows that the demographic variable number of living
children had shown statistically significant association with level of care
seeking behaviour among mothers of under five children with ARI at p<0.01
level and the other demographic variables had not shown statistically
significant association with level of care seeking behaviour among mothers of
under five children with ARI.
The table 1 depicts that regarding age of the child, most of them
117(46.61%) were aged 1 year to 3 years, 105(41.83%) of children were aged 3
years to 5 years, 25(9.96%) were aged 1 month to 1 year and 4(1.50%) were aged
less than 1 month. Considering the sex of the child, most of them 135(53.78%)
were male and 116(46.22%) were female. With respect to mother’s age, most of
them 186(74.10%) were in the age group of
21 – 30 years, 63(25.10%) were aged 31 – 40 years and 2(0.60%) were in
the age group of less than 20 years. Regarding the order of the child, most of
them 132(52.59%) were 1st baby, 107(42.63%) were 2nd born
baby and 12(4.78%) were 3rd born baby. With regard to number of
living children, most of them 166(66.14%) had two living children, 57(22.71%)
had one child and 28(11.16%) had three and above living children. Considering
the religion, most of them 234(93.23%) were Hindus, 15(5.98%) were Christians
and 2(0.80%) were Muslims.
Regarding the place of living, all
251(100%) were living in rural area. The total family income per month revealed
that most of them 146(58.17%) had an income of 20000 -30000, 89(35.46%) had an
income of 10000 and 16(6.37%) had an income of above 30000. With respect to family structure,
161(64.14%) were single parent family, 70(27.89%) belonged to nuclear family,
18(7.17%) belonged to extended family and 2(0.80%) belonged to joint family.
With regard to mother’s education level, most of them 194(77.29%) had basic
schooling, 33(13.15%) were graduates and 24(9.56%) were illiterates. Regarding
the mothers occupation, most of them 239(95.22%) were housewives and 12(4.78%)
were daily wages. Considering the culture, all 251(100%) belonged to Tamil
culture. Preferred food choice revealed that most of them 239(95.22%) were
non-vegetarian and 12(4.78%) were vegetarian. Regarding the awareness of ARI, most
of them 193(76.89%) had the awareness of ARI and 58(23.11%) were not aware of
ARI.
Considering the source of information, all 251(100%) received information through Health Worker. With respect to how often your child get’s ARI, most of them 182(72.51%) responded as less often (once in few month), 65(25.90%) responded as very often (every month) and 4(1.59%) responded as rarely (once a year). Regarding who takes care of ARI child, most of them 247(98.41%) responded as mother and 4(1.59%) responded as grandparent. Considering the foods (diet) given to the child during ARI, most of them 152(60.56%) had not at all given food, 70(27.89%) had given all fruits, 21(9.16%) had given fiber diet and only 6(2.39%) had given citrus fruits.
Graph 1: Percentage distribution of awareness about ARI among mothers of under five children with ARI. The 193 mothers are aware of ARI. 58 mothers are not aware of ARI
Section B: Assessment of care seeking behavior of mothers of under five children with acute respiratory infection.
Table 2: Frequency and percentage distribution of care seeking behaviour precursor for children with ARI
The table 2 shows that with regard to
source of ARI, most of them 89(35.46%) don’t know about the source of ARI,
59(23.51%) responded as direct contact, 41(16.33%) responded as oral,
32(12.75%) responded as Vector C, 20(7.97%) responded as formite and 10(3.98%)
responded as droplet. Considering the reason for not seeking medical help for
ARI, most of them 173*68.92%) not at all seek medical help for ARI, 75(29.88%)
used to try with home remedy like ginger/ honey/steam inhalation and only
3(1.20%) has not considered ARI is not a serious disease. Regarding the food
choice you commonly give for ARI child, most of them 142(56.57%) used to give
vegetarian and non-vegetarian food, 61 (24.50%)
used to
give only vegetarian food, 44(17.53%)
used to give milk only, 3(1.20%) used to give only non-vegetarian and only one
(0.40%) used to give no mild food.
The table 3 depicts that most of them 209(80.5%) had fever / increased body temperature i.e., 34% of the total responses, 202(80.5%) had irritation which constitutes 32.9% of the total responses, 130(51.8%) has nasal congestion / blocked nose i.e., 21.2% of the total responses, 30(12%) had difficulty in breathing which constitutes 4.9% of the total responses, 28(11.2%) had not able to drink or breast feed i.e., 4.6% of the total responses and 15(6%) had difficulty in breathing i.e., 2.4% of the total responses.
Table 3: Frequency and percentage distribution of symptoms of ARI among under five children Table 4: Choice of care for mothers of under five children with ARI Graph 2: Percentage distribution of where the ARI child be taken first by the mothers of under five children with ARI
The table 5 depicts that most of them 93(61.59%) used to take to the child specialist, 73(48.34%) used to try home remedy, 44(29.14%) used to take to general physician, 29(19.21%) used to follow old prescription of same child and 12(7.95%) used to take to medical shop. The table 3 depicts that most of them 209(80.5%) had fever / increased body temperature i.e., 34% of the total responses, 202(80.5%) had irritation which constitutes 32.9% of the total responses, 130(51.8%) has nasal congestion / blocked nose i.e., 21.2% of the total responses, 30(12%) had difficulty in breathing which constitutes 4.9% of the total responses, 28(11.2%) had not able to drink or breast feed i.e., 4.6% of the total responses and 15(6%) had difficulty in breathing i.e., 2.4% of the total responses.
Table 5: Frequency and percentage distribution of health seeking behaviour by mothers of under five children with ARI
The table 5 depicts that most of them 93(61.59%) used to take to the child specialist, 73(48.34%) used to try home remedy, 44(29.14%) used to take to general physician, 29(19.21%) used to follow old prescription of same child and 12(7.95%) used to take to medical shop. The table 6 shows that most of them 122(48.61%) had no effective health seeking behaviour, 66(26.29%) had taken prompt care and 63(25.10%) had taken delayed care.
Graph 3: Percentage distribution of health seeking behaviour by mothers of under five children with ARI Table 6: Multiple regression analysis to assess the influencing factors of care seeking behaviour among mothers of under five children with ARI with demographic variables.
The table 7 shows the binary logistic regression analysis to find
out the association of demographic variables with health seeking behaviour. The
table depicts that income had shown statistically significant association with
health seeking behaviour with chi-square value of (c2=4.790,
p=0.029)and with an odds of 1.764.
This clearly infers that income influences 1.7 times the health seeking
behaviour of mothers of under five children with ARI.
The table depicts that
awareness about ARI had shown statistically significant association with health
seeking behaviour with chi-square value of (c2=4.940,
p=0.026)and with an odds of 2.14.
This clearly infers that awareness response of ‘Yes” influences 2.14 times the
health seeking behaviour of mothers of under five children with ARI. The other
demographic variables had not shown statistically significant association with
health seeking behaviour of mothers of children with ARI.
DISCUSSION
Health seeking behavior for mothers for their child with ARI is
vital. Various studies have shown that early health seeking prevents
complications and equally reduces the rate of death. Studies from developing
countries have reported that delay in seeking appropriate care and not seeking
any care, contributes to the large number of child’s deaths4.
Improving parents/caretakers health seeking behavior could contribute
significantly to reducing child mortality in developing countries. The World
Health Organization estimates that seeking prompt and appropriate care could
reduce child’s deaths due to acute respiratory infections by 20%5. Early
health seeking behavior for child’s acute health problem could reduce
morbidity, short and long term complications of the child health problem, this
is seen in the integrated management of childhood illness (IMCI) strategy,
besides improving providers skills in managing childhood illness also aims to
improve parents/caretakers health care seeking behavior. The health workers are
trained to teach the mothers about danger signs and counsel them about need to
seek care promptly if these signs occur6 .
Epidemiologists and social
scientist have devoted increasing attention to studying health-seeking behavior
associated with the leading causes of child mortality, include respiratory
infection. Health interview surveys conducted in different countries report
varying results about the determinants of health seeking behavior during
childhood illnesses (Thind & Cruz 2003). Various factors have been
implicated as determinants of health seeking behavior of parents. Some studies
have reported that care seeking behavior is predicted by house hold size, age
and education of parents. Lack of access to health care due to high cost is
perhaps the most common deterrent to optimal health care seeking in both rural
and urban communities. Some studies have also shown that perceived illness
severity, maternal recognition of certain signs and symptoms of childhood
illness were critical factors determining health care seeking behavior7.
Mothers and Guardians as caretakers may also not seek for help or
abstain from seeking care for their child health if they fail to recognize
symptoms or do not consider them dangerous.
In addition, once a caretaker or parents has recognized illness and
decide to seek care, house hold responsibilities and long distances to health
units may still delay care seeking. When health care are sought, the quality of
treatment or care received might not be adequate and may cause delay in
subsequent seeking for the same health care. It is to this regards to reduce
respiratory infection mortality, three crucial steps in management have been
suggested by UNICEF8:
recognize, seek and treat. These steps are equally important. Many child deaths
could be averted if timely recognition of symptoms was followed by prompt care
seeking at a place where accurate diagnosis would lead to administration of
right drugs in correct doses9.
In this present study the binary logistic regression analysis to
find out the association of demographic variables with health seeking practice.
The table depicts that income had shown statistically significant association
with health seeking behaviour with chi-square value of (c2=4.790,
p=0.029) and with an odds of 1.764. This clearly infers that income influences
1.7 times the health seeking behaviour of mothers of children under five years
with ARI. The table depicts that awareness about ARI had shown statistically
significant association with health seeking behaviour with chi-square value of
(c2=4.940,
p=0.026) and with an odds of 2.14. This clearly infers that awareness response
of ‘Yes” influences 2.14 times the health seeking behaviour of mothers of under
five children with ARI. The other demographic variables had not shown
statistically significant association with health seeking behaviour of mothers
of children with ARI. Infants (0–11 months) are more commonly cared by care
takers rather than the parents and boys more than girls. Mothers below 35 years
of age, who completed secondary education and those who marry at a young age,
present with the good in
terms of caring for their sick children. Mothers who received
professional antenatal care have an advantage of bearing healthy children less
prone to infections. Previous Studies found that maternal age has effect on
care given to children in families in term of health. For rural residents,
younger mothers aged between 15–34 years are said to be more active in seeking
health care than for older mothers over 35 years of age. In urban residents,
mothers less than 25 years old present with more health seeking behavior than
those over 25 years of age. It is also reported that younger families are more
exposed to media communications than older families due to a higher education
level, which might contribute to broad information received on health issues
leading to better health seeking behaviors by those young mothers. According to
Mukandoli 10, young
mothers and males were found to be associated with prolonged delay in seeking
health care. Previous study also revealed that the health seeking behavior of a
community determines how health services are used and in turn the health outcomes
of populations.
Factors that determine health behavior may be physical,
socio-economic, cultural or political. Indeed, the utilization of a health care
system may depend on educational levels, economic factors, cultural beliefs and
practices. Other factors include environmental conditions, socio-demographic
factors, knowledge about the facilities, gender issues, political environment,
and the health care system itself11. However,
it is observed that socioeconomic, socio-cultural and demographic factors are
often ignored while formulating health policies or any schemes for providing
health care facilities to people. As a result, new schemes for providing health
care services could not achieve its goal. Thus, health seeking behaviour is
directed by socioeconomic, socio-cultural, and demographic factors, influence
the health behaviour. In addition, according to Okwaraji et al12 in effect
of geographical access to health facilities on child mortality in rural Rwanda:
a community based cross sectional study, small sized families thought more
about their children’s medical attention for respiratory infection in rural and
urban residence as opposed to large families. Families with more than 4
children suffer more not only economically but also in regards to concentrated
and time spent with their sick child. This reason was more pronounced with
urban residences perhaps due to difference in average family members. In urban
households average 3.7 persons compared to rural households with 4.9 persons.
Ethical clearance: The institution review committee of ACS Medical College and
Hospital, DR MGR Educational and Research Institute, Chennai, has granted
ethical clearance for the study with reference number 19/2019/IEC/ACSMCH dated
09/10/2019.
Conflict of interest: There was
no conflict of interest to conduct this study.
Fund for
the study: It was self-financed study.
CONCLUSION
The study concluded that most of them 93(61.59%) used to take to
the child specialist, 73(48.34%) used to try home remedy, 44(29.14%) used to
take to general physician, 29(19.21%) used to follow old prescription of same
child and 12(7.95%) used to take to medical shop.
The results can help the health seeking behavior on acute
respiratory infection among under five mothers understand various aspects of
self-management and other health care personal managements of under-five
mothers and follow up13, 14. It is
the responsibility of the nurses15 to create
understanding on the management of acute respiratory tract infection of to reduce further complication related to
acute respiratory tract infection.
REFERENCES
1. Dagne, H., et al., (2020). Acute respiratory infection and its associated factors among children under-five years attending pediatrics ward at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia: institution-based cross-sectional study. BMC pediatrics,20(1): p.1-7.
2. Krishnan, A., et al., (2015). Epidemiology of acute respiratory infections in children-preliminary results of a cohort in a rural north Indian community. BMC infectious diseases, 15(1): p. 1-10.
3. Imran, M., et al., (2019). Risk factors for acute respiratory infection in children younger than five years in Bangladesh. Public health, 173: p. 112-119.
4. Sreeramareddy, C.T., et al., (2006). Care seeking behavior for childhood illness-a questionnaire survey in western Nepal. BMC international health and human rights, 6(1): p. 7.
5. Källander, K., et al., (2008). Delayed care seeking for fatal pneumonia in children aged under five years in Uganda: a case-series study. Bulletin of the World Health Organization, 86: p. 332-338.
6. Stewart, M.K., et al., (1993).Acute respiratory infections (ARI) in rural Bangladesh: perceptions and practices. Medical anthropology,. 15(4): p. 377-394.
7. Ferdous, F., et al., (2014). Mothers’ perception and healthcare seeking behavior of pneumonia children in rural Bangladesh. ISRN family medicine.
8. Mathew, J.L., et al., (2011). Acute respiratory infection and pneumonia in India: a systematic review of literature for advocacy and action: UNICEF-PHFI series on newborn and child health, India. Indian pediatrics, 48(3): p. 191.
9. Williams, B.G., et al., (2002). Estimates of world-wide distribution of child deaths from acute respiratory infections. The Lancet infectious diseases, 2(1): p. 25-32.
10. Mukandoli, E., (2017). Health seeking behaviors of parents/caretakers of children with severe respiratory infections in a selected referral hospital in Rwanda. University of Rwanda.
11. Francis Jebaraj, H.S., (2015).Stopping the run-around: addressing Aboriginal community people’s mental health and alcohol and drug comorbidity service needs in the Salisbury and Playford local government areas of South Australia.
12. Okwaraji, Y.B., et al., (2012). Effect of geographical access to health facilities on child mortality in rural Ethiopia: a community based cross sectional study. Plos one, 7(3): p. e33564.
13. Hepsibah S Francis, Unit 4; (2020). Guidance and Counciling in Essentials of Commun-ication and Educational Technology for BSc Nursing, K.C. Gopichandran. L, Editor. CBS Publishers and Distributors Pvt. Ltd. : Delhi.
14. Sharmil, H., (2019).Health Information Technology Media by Nurses in Patient Care. International Journal of Linguistics, Literature and Translation, 2(2): p. 290235.
15. Sharmil,S.H.,(2011). Awareness of Commu- nity Health Nurses on Legal Aspects of Health Care. International Journal of Public Health Research,(Special issue): p. 199-212.
Citation: E. Usha, S Hepsibah Sharmil, R. Ruth Saranya (2020). Practice of mothers to seek medical attention for their children with acute respiratory infection, ijmaes; 6 (3); 770-783.
Background: Low back pain was the most common case in musculoskeletal disorders. Non-specific low back pain (NSLBP) described as low back pain with no clear causal relationship between the symptoms, physical findings, and imaging findings. This study aimed to briefly review the evidence the evaluation and intervention for NSLBP in physiotherapy practice. Methods: In this study, the library research method was used, which took online and offline data sources referring to books, journals, articles related to the topic of evaluation and physiotherapy intervention in NSLBP conditions as a data source to answer research objective Results: Some researchers commonly assess the pain, range of motion (ROM), functional ability and quality of life. As a regular treatment for non-specific low back pain, some study recommended general therapeutic exercise and manual therapy to reduce the problematic of non-specific low back pain. Conclusion: Physiotherapist can evaluate patients with NSLBP based on the patients complains like pain using VAS or NPRS, Lumbar ROM using schober method, functional disability using ODI or RMDQ and Quality of life. For the physiotherapy intervention of non-specific low back pain, we can summarize that the first-line management of NSLBP is self-management exercise. Furthermore, physiotherapist can use any method of therapeutic exercise and manual therapy to reduce pain, improve lumbar ROM, increase functional ability and quality of life.
Keywords: Non-specific Low Back Pain, Evaluation, Intervention, Physiotherapy
Received on 08th August 2020, Revised on 22nd August 2020, Accepted on 29th August 2020, DOI:10.36678/IJMAES.2020.V06I03.001
INTRODUCTION
Low back
pain was the most common case in musculoskeletal disorders 1. The
challenge when managing the low back pain was diagnosing the low back pain and
choose the treatment 2. In general, the low back pain consists of
two types, which is specific and non-specific low back pain (NSLBP). Low back
pain with specific type can be divided into low back pain that related to
vertebrae and non-vertebrae. In the other hand, NSLBP described as low back
pain with no clear causal relationship between the symptoms, physical findings,
and imaging findings 3. In addition, NSLBP is classified into low
back pain, which is not related to the neurological problem and degenerative
syndrome 4.
Previously,
some research showed that NSLBP mainly affected the young population. Non-specific
low back pain has also increased in the general community, which have affected
the adolescents and middle-aged worker 5. Nordin et al. reported
that the incidence of NSLBP among undergraduate student in health sciences
programs was 40.3%, the incidence was associated with the age, years of study,
physical fitness, and hours they spent sitting in the classroom 6.
Another research by Anggiat et al. showed a similar result that students in a
university experience NSLBP with 74.6% 7. Also, a community-based
program revealed that teachers also experience low back pain with more than
half of the teacher population 8.
Numerous
research already conducted to evaluate the non-specific low back pain. The most
common evaluations were pain assessment, trunk flexibility, functional ability
and quality of life 9,10,11. Those evaluations seem to be correlated
with the population which experienced NSLBP because the NSLBP mainly causes
pain, reduced flexibility of trunk movement, functional limitation and
sometimes also affected to quality of life 12. Furthermore, most
studies also conducted in the physiotherapy intervention for NSLBP.
Physiotherapy was the first line care to give intervention in person who
experienced NSLBP 13. Some research was done resulting recommendation
of using home exercise program, manual therapy and general exercise therapy 2,
14, 15.
From the
background, this study aimed to briefly review the evidence the evaluation and
intervention for NSLBP in physiotherapy practice. In addition, with this
article, the physiotherapist will easily use the evidence to treat the
non-specific low back pain.
METHOD
In this study, the library research method was used,
which took online and offline data sources referring to books, journals,
articles related to the topic of evaluation and physiotherapy intervention in
NSLBP conditions to answer research objective. The use of books is focused on
basic science such as evaluation and applied anatomy. In the intervention,
articles in journals and clinical guidelines were used that recommend
physiotherapy in NSLBP conditions. The searching strategy was conducted a
literature search using the online database in google scholar for
‘‘physiotherapy for non-specific low back pain’’ The bibliographies of
particularly relevant articles were searched as well.
RESULT AND DISCUSSION
Applied
anatomy and contributing factor of NSLBP: Non-specific low back pain mainly
related with posture or poor body mechanic. There are several other factors
caused the NSLBP with anatomical problem. Some anatomical related factors can
be contributed to the incidence of NSLBP. Lumbar flexion motion is performed by
rectus abdominis, external and internal oblique. For extension motion is
performed by illiocostalis, longissimus, semi spinalis, multifidus. For lateral
flexion motion, performed by quardatus lumborum and also assisted by
illiocostalis, longissimus, spinalis. For rotation motion, the prime mover is
tranversus abdominis, and multifidus work contralateral for every rotation
motion 16. Some muscles of the back that related with the low back
pain are tranverse abdominis, internal obliques, erector spinae and multifidus.
Those muscles will indicate low back pain problem if the muscle has poor
muscular endurance, which is related with, prolonged posture activity 17.
Currently, multifidus muscle dysfunction is being implicated as a contributory
factor in the development or recurrence of sub-acute and chronic back pain 18.
In general,
NSLBP has two classifications; an acute stage, which pain lasts less than 12
weeks and chronic stage, which pain lasts more than 12 weeks 19.
According to Taguchi, chronic NSLBP was due to physiological structural
fragility in lumbar region, and often caused by improper posture, which can be
called a living functioning impairment 4. A research showed that
mobility of the spine reduced causing disorders in muscle synergies and
consequently increased the energy cost of maintaining postural ability 14.
One of the causes of NSLBP is
postural pain caused by prolonged sitting activity for about 2 hours a day,
which causes increased discomfort in the body 20,21. Sitting in a
slumped position is also associated with fatigue in the internal oblique
muscles and/or transverse abdominis which keeps the spine in one position so
that it makes these muscles prone to injury and can also be caused by atrophy
of the multifidus and para-spinal muscle 21.
Another
study also reported that sitting in a position such as the excessive kyphotic
posture with frequent lumbar flexion or the excessive lordotic posture with too
much extension can result in low back pain 22. A study in Japan, it
was reported that 22% of the population aged 20-85 years had NSLBP 23.
In line with several other studies, it also reported that students, office
workers and teachers also experience NSLBP due to prolonged sitting for at
least 3 hours a day 6,7,8. The pain produced by NSLBP in a
population of both students, teachers and office workers can affect
physiological and psychological stress and sometimes cause secondary
disturbances in the form of decreased quality of life 4, 5.
Evaluation
for NSLBP: To assess the effect of low back pain to
individual life, the physiotherapist will carry out several assessments to
evaluate low back pain and its impact. Some researchers commonly assess the
pain, range of motion (ROM), functional ability and quality of life 9,10,15,24.
Physiotherapist
commonly uses the visual analogue scale (VAS) to assess the pain perception of
low back pain 15, 25. In a study by Hawker et al. shouted that the
VAS is self-completed by the respondent.
They also
mentioned that the VAS is widely used due to simplicity and adaptability to a
broad range of population and settings 26. As a subjective
measurement of pain, VAS consists of a 10 cm line with two end-points
representing ‘no pain’ and ‘worst imaginable pain’. Patients will have asked to
rate their pain by placing a mark on the line corresponding to their current
level of pain 27.
The VAS is a
well-known assessment tool for pain and recommended as a means of rating the
subjective pain 20. Another version with the same meaning of VAS,
physiotherapist can use Numeric Pain Rating Scale (NPRS) which consist of
number 0 for no pain until 10 which worst worst imaginable pain.
Physiotherapists can use either of these pain evaluations because those pain evaluation
tool have the same validity and reliability 26.
As the pain was assessed in the
non-specific low back pain, another assessment that related with pain was the
flexibility of the lumbar spine, where the pain will affect the flexibility of
lumbar spine 28. Furthermore, a study by Wong and Lee describes that
there is a correlation between patients with LBP and the decreased lumbar ROM 29.
The flexibility of the lumbar spine is related to the lumbar range of motion
(ROM). They also conclude that the lumbar ROM should be evaluated after the
treatment of LBP to know the effects of the treatment. Previously, some
researcher decided to use a measuring tape to evaluate the lumbar ROM 10,30.
Tape measurements were the least expensive method to measure spinal movement
and perhaps the easiest to use 31. In order, to measure flexion and
extension of lumbar, the modified Schober method can be used by the
physiotherapist 32. Some studies also reported that the Schober
method was one of the good methods to assess the lumbar flexibility 32, 33.
In order, to measure lateral
flexion, the fingertip-to-floor method can be used as an additional measurement
of lumbar ROM 31. However, flexion and extension were the most
commonly used as the main evaluation of the lumbar range of motion in low back
pain cases 10, 34.Clearly, the flexion and extension movement is the
main segmental movement of the lumbar spine 35.
The risk of people with NSLBP
who have high pain score may also develop functional disability 36.
Furthermore, to evaluate disability, should to use disability measurement along
with pain measurement. In other studies, it was reported that pain was also
associated with impaired functional activity, which in this case could cause
disability, where a high rate of disability was associated with high pain rates
37. Activity disorders that can occur in patients with NSLBP are
activities indoor and outdoor activity such as on travelling, climbing and
descending stairs, walking, wearing clothes, eating, using the toilet, using
public transportation and other social activities 38.
Several studies provide
recommendations using the Oswestry Disability Index (ODI) for assessment of
functional disability caused by LBP 39,40,41. The Oswestry
disability index (ODI) is aimed specifically at LBP conditions and is the best
standard in evaluating the functional activity of people with NSLBP both before
and after the intervention 39. Furthermore, research from Fairbank
and Pynsent stated that ODI has been translated into several languages
including English and can then be used validly and reliably for examining
conditions of back pain related to disability evaluation 42.
On the other hand, other
evaluation related to functional activities, the physiotherapist can use the
Rolland-Morris Disability Questionnaire (RMDQ) 43. In general, RMDQ
also has similar validity and reliability to ODI, but in detail, ODI is still
superior in evaluating NSLBP patients 44, 45.
Furthermore, the RMDQ is still
considered a very useful evaluation tool in evaluating the condition of NSLBP
patients. Similar to ODI, RMDQ also evaluates the patient’s status in terms of
pain, dysfunction and disability 43. Thus, evaluation before and after
the intervention can be carried out using the questionnaire to see the changes
that occur before and after the intervention.
Non-specific
low back pain with a long period of time can affect the quality of life. Pain
that is quite severe has contributed to reducing the quality of life of an
individual 46. Furthermore, in their study, it was concluded that
the LBP condition was quite severe and reduced activity was also associated
with physical functional disorders and even caused mental disorders and individual
productivity.
Followed by
other research by Tsuji et al. also reported that the condition of pain was
quite high and disturbances in quality of life affected the decrease in
productivity of workers with NSLBP 47. Furthermore, they also
suggested to be able to evaluate the quality of life of individuals who have
NSLBP as an essential examination. In field of education, Kennedy et al. also
reported that students with LBP affect their quality of life by decreasing
psychosocial aspects such as experiencing sadness, being overwhelmed and
exhausted 48.
Evaluation
of quality of life generally uses the Health-related quality of life (HRQoL)
questionnaire. The questionnaire in the quality of life examination is
generally classified into generic, condition specific, or patient specific. In
evaluating the HRQoL in low back pain population, the condition-specific
instrument of HRQoL can be used.
The HRQoL is
a multidimensional concept that refers to function and well-being on various
dimensions of health, including physical, emotional, social and spiritual
aspects of life 49. Some of the HRQoL instruments that can be used
to assess the quality of life on low back pain patient is the Short Form
36-items Health Survey (SF-36) or with other short versions such as SF-12 or
SF-8 50.
Physiotherapy
Intervention: As a regular treatment for non-specific low back pain, some study
recommended general therapeutic exercise to reduce the impairment of NSLBP 51, 52. The type of general
exercise for low back pain mainly is an active stretching, which easily
performed by the patient 53. A study by Gawda et al. revealed that
the stretching therapy that done by the patients could be effective to reduce
the low back pain 14. In their study, the physiotherapist gives some
example to do the stretching until the patients can do the stretching by
themselves. Some guidelines, also reported some educational exercise that can
be done by the low back pain patient to manage the low back pain 19,54.
In 2016, National Institute for Health and Care Excellence (NICE) produce an
assessment and management guideline for the low back pain. In that guidelines,
described that the self-management was the first management for low back pain 13.
A review study by Bardin, King
and Maher also recommended self-management exercise along with hot-pack as the
first line care for NSLBP 2. The use of hot packs considered as a
pain relief that provides analgesia effect and muscle relaxation 2,55.
Self-management exercise or educational home exercise program with hot packs
also recommended by a health care guideline as a management of low back pain
patient 54. A research by Taguchi stated that the therapeutic
heating is often conducted by physiotherapy for the chronic NSLBP, despite the
effectiveness in not clear, however, from the viewpoint of relaxation, the
purpose of therapeutic heating is reducing the pain 4.
Furthermore, several clinical
guidelines provide recommendations for interventions in the management of LBP
in clinical practice. In America, the clinical practice guidelines made by the
American Physical Therapy Association (APTA) recommend several interventions
that can be used in general in LBP patients 43.
The first recommendation is to
use manual therapy with joint mobilization or thrust manipulation to reduce
pain and disability. Then, for therapeutic exercise intervention is recommended
using back-specific strengthening, coordination and endurance exercises. Those
two recommendations are based on strong recommendations. In addition, it is
also recommended to use patient education/counseling for disruption of
activities due to LBP and increase endurance with fitness and endurance
activity based on moderate and strong recommendations.
Another clinical recommendation
in the United Kingdom also provides several options in physiotherapy
intervention in LBP conditions 13. In addition to using
self-management exercises, physiotherapists are also recommended to use
exercise therapy such as exercises based on biomechanics, aerobics or in
combination with other types of exercise. Just like in APTA guidelines, in the
next recommendation, physiotherapy is also recommended using manual therapy
such as mobilization or spinal manipulation and also soft tissue manipulation.
Besides, they also recommend using psychological therapy such as the
cognitive-behavioral approach in combination with exercise therapy or manual
therapy.
In a study by Oliviera et al.
that reviewed clinical practice guidelines for the management of NSLBP,
recommended several suggestions related to physiotherapy interventions in NSLBP
56. In general, in the types of physiotherapy interventions, they
recommend exercise therapy for the management of both acute and chronic NSLBP.
Although the types of exercise therapy are still considered inconsistent,
physiotherapists can use various types of exercise therapy according to the
therapist’s ability. Subsequently, manual therapy with spinal manipulation has
also become a recommended intervention in the management of both acute and
chronic NSLBP.
In manual therapy, the
physiotherapist can choose to use spinal mobilization or manipulation, however,
exercise therapy has several types of methods that can be used according to the
physiotherapist’s ability to perform the methods 13,43. Exercise
therapy that can be recommended is the motor control exercise approach and core
stability exercises 57,58. Exercises using a flexion and extension
approach as known as the directional preference of McKenzie method or the other
name is Mechanical Diagnosis and Therapy (MDT) can be used as well 59.
Furthermore, exercise therapy
with a proprioceptive approach such as Proprioceptive Neuromuscular
Facilitation which is rarely used in musculoskeletal cases, can be used in
NSLBP patients as well. All types of exercise therapy have a beneficial effect
in reducing pain, increasing lumbar ROM and improving functional activity and
quality of life with no superiority among each other methods 41,60.
This study is a simple short
review study in the evaluation and intervention of physiotherapy in NSLBP
conditions. There are still many limitations in this research, so that, in the
future, a more comprehensive review study method should be carried out.
CONCLUSIONS
Numerous
research has been able to provide very useful information to the
physiotherapist to evaluate and treat the patients with NSLBP. Based in this
present study, we can conclude that physiotherapist can evaluate patient with
NSLBP based on the patient’s complaints such as pain using VAS or NPRS, Lumbar
ROM, functional disability using ODI or RMDQ and quality of life questionnaire.
For the
physiotherapy intervention of NSLBP, we can summarize
that the first-line management of NSLBP is self-management exercise.
Furthermore, physiotherapist can use any method of therapeutic exercise and
manual therapy to reduce pain, improve lumbar ROM, increase functional ability
and improve the quality of life.
Conflict of interest:
The
author has no conflict of interest to declare.
Funding of study: This study has no funding or sponsorship was received.
It is
self-financed study.
Compliance
with Ethics: This study based on review of
previous conducted studies with does not contain any studies with human or
animals.
REFERENCES
Maher, C., Underwood, M., Butchbindee, R. (2017). Non-specific low back pain. Seminar, Lancet 389: 736-47
Bardin L, D., King P., Maher C, D. (2017). Diagnostic triage for low back pain : a practical approach for primary care. The Medical Journal Australia 206 (6), 268-273.
Balagué, F., Mannion, A. F., Pellisé, F., & Cedraschi, C. (2012). Non-specific low back pain. The lancet, 379(9814), 482-491.
Taguchi, T. (2003). Low back pain in young and middle-aged people. Journal of Japan Medical Association. JMAJ, 46(10): 417-423.
Aziz, S., Ilyas, S., Imran S., Yamin F., Zakir A., Rehman A., Adnan S., Khanzada S. (2016). Effectiveness of McKenzie Exercise in Reducing Neck and Back Pain Among Madrassa Student. International Journal Physiotherapy 3 (1), 78-85.
Nordin, N. A., Devinder, A. S., & Kanglun, L. (2014). Low Back Pain and Associated Risk Factors among Health Science Undergraduates. Sains Malaysiana, 43(3), 423–428.
Anggiat, L., Hon, W. H. C., & Baait, S. N. (2018). The incidence of low back pain among university students. Pro-Life, 5(3), 677-687.
Budhyanti, W., Anggiat, L., & Juwita, C. P. (2020). Pencegahan dan penanganan nyeri leher dan punggung bawah dengan peregangan mandiri pada pegawai sekolah menengah kejuruan negeri 10 cawang. Jurnal Fisioterapi dan Rehabilitasi, 4(1), 79-89.
Dhaliwal, M. K., Amandeep, Jagmohan., Manjeet. (2014). To compare the effect of proprioceptive neuromuscular facilitation program versus core stabilization exercise for decreasing pain and improving function in patients with low back pain. IOSR Journal of sport and physical education 1. PP 29-35.
Park, K.Y., Seo, K.Y. (2014). The Effects on the pain index and lumbar flexibility of obese patients with low back pain after PNF Scapular and PNF pelvic patterns, Journal of Physical Therapy Scienes 26 : 1571-1574.
Anggiat, L., Hon, W. H. C., & Sokran, S.N.B.B.M. (2018). Comparative effect of proprioceptive neuromuscular facilitation and mckenzie method on pain in non-specific low back pain among university population. International Journal of Medical and Exercise Science, 4(3), 475-485.
Pergolizzi, J. V., & LeQuang, J. A. (2020). Rehabilitation for Low Back Pain: A Narrative Review for Managing Pain and Improving Function in Acute and Chronic Conditions. Pain and Therapy, 1-14.
National Institute for Health and Care Excellence (NICE). (2016). Low back pain and sciatica in over 16s: assessment and management. United Kingdom : NICE Guidelines. nice.org.uk.
Gawda P, Dmoszyńska-Graniczka M, Pawlak H, Cybulski M, Kiełbus M, Majcher P, Buczaj A, Buczaj M. (2015). Evaluation of influence of stretching therapy and ergonomic factors on postural control in patients with chronic non-specific low back pain. Annals of Agricultural and Environmental Medicine 22(1): 142-146.
Waqqar, S,. Rehman S, S., Ahmad, S. (2016). McKenzie treatment versus mulligan sustained natural apophyseal glides for chronic mechanical low back pain. Pakistan Journal of Medical Sciences 32(2):476-479.
Cael, C. (2010). Functional Anatomy: musculoskeletal anatomy, kinesiology, and palpation for manual therapists. Lippincott Williams & Wilkins, a Wolters Kluwer business. Philadelphia, PA.
Kisner, C., Colby, L.A. (2012). Therapeutic Exercise: Foundation and techniques 6th edition, F.A. Davis Company. USA
Danneels, L., Dickx, N and Cagnie, B.(2010) Low Back and Pelvic Pain, 7th Interdisciplinary world congress, Proceedings. p.186-195.
Hussein A.M.M., Singh D., Mansor, M., Kamil, O.I.M., Choy, C.Y. Vijayan, R.(2009). Malaysian Low Back Pain guideline. First Edition. Malaysian Association for the Study of pain and Spine society Malaysia
Casser HR, Seddigh S, Rauschmann M. (2016). Acute lumbar back pain-investigation, differential diagnosis and treatment. Deutsches Ärzteblatt International, 113: 223-34.
Waongenngarm, P., Rajaratnam, B. S., & Janwantanakul, P. (2016). Internal Oblique and Transversus Abdominis Muscle Fatigue Induced by Slumped Sitting Posture after 1 Hour of Sitting in Office Workers. Safety and Health at Work 7(1): 49-54.
Dankaerts W., O’Sullivan P., Burnett, A., Straker, L. (2006). Differences in sitting posture are associated with nonspecific chronic low back pain disorders when patients are subclassified. SPINE 31 (6), pp 698-704.
Suzuki H, Kanchiku T, Imajo Y, Yoshida Y, Nishida N, Taguchi T. (2016). Diagnosis and Characters of Non-Specific Low Back Pain in Japan: The Yamaguchi Low Back Pain Study. PLoS ONE 11 (8): e0160454.
Longo G, Loppini M, Denaro L, Maffulli N, Denaro V. (2010). Rating scales for low back pain. British Medical Bulletin, 98 ; 81-144.
Hosseinifar M., Akbari M., Behtash H., Amiri M., Sarrafzadeh, J. (2013). A Comparison between the Effects of Stabilization and Mckenzie’s Exercises on the Pain, Disability, and Lumbo-Pelvic Stability in Patients with Non-Specific Chronic Low Back Pain” Life Sciences Journal ,10(10s); 298-302.
Hawker G.A., Mian, S., Kendzerka, T., French, M. (2011). Measures of Adult Pain. American College of Rheumatology. Arthritis Care & Research 63 (11): pp S240–S252,.
Huskisson EC. (1974). Measurement of pain. Lancet, 2(7889):1127-31.
Lee A, S., Cholewicki, J., Reeves N, P, Zazulak B,T., Mysliwiec, L, W. (2010). Comparison of Trunk Proprioception Between Patients With Low Back Pain and Healthy Controls. Archives of Physical Medicine and Rehabilitation 91 (9):1327-1331.
Wong, T, K, T and Lee, R, Y, W. (2004). Effect of low back pain on the relationship between the movements of lumbar spine and hip. Human Movement Science 23 : 21-34. doi:10.1016/j.humov.2004.03.004.
Franklin, C.V.J., Kalirathinam, D., Palekar T., Nathani N. (2013). Effectiveness of PNF Training for Cronic Low Back Pain. IOSR Journal of Nursing and Health Science (IOSR-JNHS) 2 :41-52.
Reese, N., Bandy, W. (2002). Joint Range of Motion and Muscle Length Testing. Saunders Company. Philadelphia, USA.
Sihawong R., Sitthipornvorakul, E., Paksaichol, A., Janwantanakul P. (2016). Predictors for chronic neck and low back pain in office workers: a 1-year prospective cohort study. Journal of Occupational Health 58: 6-24.
Chhaya, V., Renuka D., Vijaya K., Amol B. (2015). Lumbar range of motion : Reliability between schober’s test and modified schober’s test. Romanian Journal of Physical Therapy 21/ Issue 35/ may/ pp
Kumar A., Zutshi K,. Narang N.(2011). Efficiacy of Trunk Propioceptive Neuromuscular Facilitation Training on Chronic Low Back Pain. International Journal of Sports Science and Engineering 5 (3): pp. 174-180.
Key, J., Chaitow L. (2010). Back Pain: A Movement Problem, A Clinical Approach incorporating relevant research and practice. 1st Edition, Churchill Livingstone, Elsevier. UK.
Melton, B, L., Moqbel, M., Kanaan, S., Sharma, N, K. (2016). Structural Equation Model of Disability in Low Back Pain, Spine, 41(20), 1621.
Davis, D, S., Mancinelli, C, A, Petronis, J, J., Bensenhaver, C., Mcclintic, T., Nelson, G. (2013). Variables associated with level of disability in working individuals with nonacute low back pain: a cross-sectional investigation. Journal of orthopaedic & sports physical therapy 43 (2), 97-104.
Di Iorio, A,.Abate, M,. Guralnik, J,M., Bandinelli,S,. Cecchi, F,.Cherubini,A., Corsonello, A., Foschini, N., Guglielmi, M., Lauretani, F., Volpato, S., Abate, G., Ferrucci, L. (2007). From Chronic Low Back Pain to Disability, a Multifactorial. Spine (Phila Pa 1976). 32(26): E809–E815.
Seif, H.E., et al. (2015) The Effect of Stretching Hamstring, Gastrocnemius, Iliopsoas and Back Muscles on Pain and Functional Activities in Patients with Chronic Low Back Pain: A Randomized Clinical Trial. Open Journal of Therapy and Rehabilitation 3: 139-145.
Vincent, J.I., MacDermit, J.C., Grewal, R., Sekar, V.P., Balachadran, D. (2014). Translation of Oswestry Disability Index into Tamil with cross cultural adaptation and evaluation of reliability and validity. The Open Orthopedic Journal 8: 11-19.
Anggiat, L., Hon, W. H. C., Sokran, S. N. B. B. M., & Mohammad, N. M. B. (2020). The changes of functional disability in non-specific low back pain among university population after proprioceptive neuromuscular facilitation and mckenzie method. International Journal of Medical and Exercise Science, 6(1), 656-667.
Fairbank J, and Pynsent P. (2000). The Oswestry Disability Index. SPINE, Lippincott Williams & Wilkins, Inc 25(2) : 2940-2953.
Delitto, A., George, S., van Dillen, L., Whitman J., Sowa G., Shekelle P. Godges, J, J. (2012). Low back pain : clinical practice guidelines linked to the international classification of functioning disability, and health from the orthopaedic section of the American Physical Therapy Association. Journal of orthopaedic and sport physical therapy. 42 (4).pp
Yi, H., Ji, X., Wei, X., Chen, Z., Wang, X., Zhu, X. & Li, M. (2012). Reliability and validity of simplified Chinese version of Roland-Morris questionnaire in evaluating rural and urban patients with low back pain. PLoS one, 7(1), e30807.
Stevens, M. L., Lin, C. C., & Maher, C. G. (2016). The roland morris disability questionnaire. Journal of physio-therapy, 62(2), 116.
Montgomery, W., Vietri, J., Shi, J., Ogawa, K., Kariyasu, S., Alev, L., Nakamura., M, (2016), The relationship between pain severity and patient-reported outcomes among patient with chronic low back pain in Japan, Journal of Pain Research 9:337-344.
Tsuji T., Mastudaira K., Sato H., Vietri J. (2016). The impact of depression among chronic low back pain patients in Japan. BMC Musculoskeletal Disorders. Biomed Central. 17:447.
Kennedy C, Kassab O, Gilkey D., Linnel, S., Morris D.(2008) Psychosocial Factors and Low Back Pain Among College Students. Journal of American College Health, 57:2, 191-196.
Younsi, M., (2015), Health-related quality of life measures: Evidence from Tunisian population using the SF-12 Health Survey. International Society of Pharmaco-economics and Outcome Research (ISPOR). Elsevier, 7C: 55-66.
Resnik, L., and Dobrzykowski,E. (2003).Guide to outcome measurement for Patient with Low Back Pain syndromes, Journal of Orthopedic and Sport Physical Therapy 33: 307-318.
Gordon, R., Bloxham, S. (2016). A Sytematic review of the effects of exercise and physical activity on non-specific cronic low back pain, Healthcare journal 4(22): 10.3390.
Scharrer M, Ebenbichler G, Peiber K, Crevenna, Gruther W, Zorn C, Grimm- Steiger, Herceg M, Keilani M, Ammer K.(2012). As ystematic review on the effectiveness of medical training therapy for subacute and chronic low back pain. European Journal Physical Rehabilitation Medicine 48: 361-70.
Sihawong, R., Janwantanakul, P., & Jiamjarasrangsi, W. (2014). A prospective, cluster-randomized controlled trial of exercise program to prevent low back pain in office workers. European Spine Journal 23(4): 786–793.
Goertz M, Thorson D, Bonsell J, Bonte B, Campbell R, Haake B, Johnson K, Kramer C, Mueller B, Peterson S, Setterlund L, Timming R. (2012). Adult Acute and Subacute Low Back Pain. Institute for Clinical Systems Improvement.
Arya, R.K. (2014). Low Back Pain-Sign, symptoms, and management, Journal, Indian Academy of Clinical Medicine 15 (1), 30-41.
Oliveira, C. B., Maher, C. G., Pinto, R. Z., Traeger, A. C., Lin, C. W. C., Chenot, J. F.,& Koes, B. W. (2018). Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. European Spine Journal, 27(11), 2791-2803.
Areeudomwong, P., & Buttagat, V. (2019). Comparison of Core Stabilisation Exercise and Proprioceptive Neuromuscular Facilitation Training on Pain-related and Neuromuscular Response Outcomes for Chronic Low Back Pain: A Randomised Controlled Trial. The Malaysian Journal of Medical Sciences: MJMS, 26(6), 77.
Niederer, D., & Mueller, J. (2020). Sustainability effects of motor control stabilisation exercises on pain and function in chronic nonspecific low back pain patients: A systematic review with meta-analysis and meta-regression. PloS one, 15(1), e0227423.
Sanchis-Sánchez, E., Lluch-Girbés, E., Guillart-Castells, P., Georgieva, S., García-Molina, P., & Blasco, J. M. (2020). Effectiveness of mechanical diagnosis and therapy in patients with non-specific chronic low back pain: a literature review with meta-analysis. Brazilian Journal of Physical Therapy.
Areeudomwong, P., & Buttagat, V. (2019). Proprioceptive neuromuscular facilitation training improves pain-related and balance outcomes in working-age patients with chronic low back pain: a randomized controlled trial. Brazilian Journal of Physical Therapy, 23(5), 428-436.
Citation: Lucky
Anggiat (2020). A brief review in Non-Specific
Low Back Pain: Evaluation and physiotherapy intervention, ijmaes; 6 (3); 760-769.
2BPT Intern, School of Physiotherapy, D.Y.Patil, Deemed to be University, Mumbai, Maharashtra, India
Corresponding Author :
1Associate Professor, School of Physiotherapy, D.Y.Patil, Deemed to be University, Mumbai, Maharashtra, India , Mail id: drsathyagp@gmail.com
ABSTRACT
Introduction: Text neck syndrome refers to overuse syndrome or repetitive stress injury, in which you have your head hung forward or down looking at your mobile or any other electronic device for a longer period of time. This eventually leads to tightness of the shoulder muscles and soreness in the neck muscles or even chronic headaches. The purpose of this study was to find out the prevalence of text neck syndrome in young adult population using Neck Disability Index (NDI) questionnaire.
Methodology: A cross sectional study was conducted among 100 Physiotherapy students of the age group from 18 to 25 years from D.Y. Patil University, Navi Mumbai. Demographic data was collected and the students were asked to fill the Neck Disability Index questionnaire and the data was further analysed to check which gender and age group was affected the most.
Results: Females were most affected with 80% and the age group which was most affected was 22 years (34%).
Conclusion: This study concluded that prevalence of text neck syndrome is 32%. The major component affected according to neck disability index out of all the components is headache followed by sleeping, concentration and reading.
1Jomi John, MPT Musculoskeletal and Sports-student, CPAS School of Medical Education,
Gandhinagar, Kottayam, Kerala, India, Mail id: jomijohn333@gmail.com
Co Author:
2Associate Professor of Physiotherapy, CPAS School of Medical Education, Gandhinagar, Kottayam, Kerala, India
ABSTRACT
Background and objectives: Plantar fasciitis is a commonly confronted orthopedic problem due to inflammation of the plantar fascia and the perifascial structures. The literature attributes plantar fasciitis is due to pathologic biomechanics such as excessive pronation, high arched foot, windlass mechanism and low back disabilities. Current evidences suggest that faulty biomechanics that lead to plantar fasciitis may be started from gluteal muscles weakness. The purpose of the study is to find out the effectiveness of gluteal muscles strengthening exercises to reduce pain and improve lower limb function in patients with plantar fasciitis.
Methods: 30 subjects those satisfying the inclusion criteria were recruited for the study. Subjects were then allocated to two groups- Group A (control group) and Group B (experimental group), 15 in each group. Subjects in group A received conventional treatment and subjects in group B received experimental treatment of gluteal muscle strengthening exercises with conventional stretching exercise. Pain was measured using Numeric Pain Rating Scale (NPRS) and lower limb functions was measured using Star Excursion Balance Test (SEBT).
Results: The post test score of SEBT and NPRS of control and experimental group were analysed using two sample t test and paired t test. The data analysis showed statistically significance difference in the post test scores of SEBT and NPRS of experimental group over control group at 5% level.
Conclusion: This study concluded that gluteal muscles strengthening exercises helps in improving lower limb function and reduction in pain in patients with plantar fasciitis.
1Professor, Faculty
of Physiotherapy, DR MGR Educational and Research Institute, Deemed to be
University, Chennai, India
Corresponding Author:
2Physiotherapist, Ergon Physiotherapy and fitness lifestyle, Thiruvanmiyur, Chennai, India, Mail id: marsanirudh80@gmail.com
ABSTRACT
Background and objective of the study: Cricket is the most popular team sport in Indian subcontinent. Hand grip strength plays a vital part in all roles of cricket which may be associated with Body Mass Index. Grip strength is the force applied by the hand to pull or suspend from objects and is a specific part of hand strength. BMI is an attempt to quantify the amount of tissue mass (muscle, fat and bone) in an individual to categorize a person as underweight, normal weight, overweight or obese based on values. Objective of the study was to find out the association between BMI and hand grip strength in university level cricketers.
Methodology: This was an experimental and cross-sectional type study carried out at Faculty of physiotherapy, Dr. M.G.R. Educational and research institute, Chennai. Total 30 male cricketers, with age group of 18 to 25 years were included in this study. Cricketers with upper limb fractures or dislocations within one year were excluded from the study. Hand grip dynamometer, weighing machine and inch tape were the materials and measurement tools used for the study. 30 University level cricketers were divided into 4 groups, Group A, Group B, Group C and Group D based on BMI level. Body Mass Index and Hand grip strength are the outcome measures. Body mass index were calculated by measuring the height and weight of the individuals. Hand grip strength was measured for their dominant side by using the hand grip dynamometer.
Result: There is a positive association and strong correlation between Body Mass Index and Hand Grip Strength between the Groups at (r = 0.523) & (P ≤ 0.05).
Conclusion: The study concluded that cricket players with Obese Body Mass Index have more Hand Grip Strength. The study also reported a strong association of Hand Grip Strength with Body Mass Index.
Keywords: Body Mass Index (BMI), Hand grip strength, Cricketers, Hand grip dynamometer.
Received on 22nd April
2020, Revised on 22nd May
2020, Accepted on 29th May 2020