| Izham Zain1, Nabilah Ahmad2, Nanthenii M.K2, Asyiqin3 Authors: 2Physiotherapy Department, School of Health Sciences, KPJ Healthcare University College, 71800 Nilai, Negeri Sembilan, Malaysia. 3Physiotherapy Department, KPJ Seremban Specialist Hospital, Seremban, Malaysia. Corresponding Author: 1Physiotherapy Department, School of HealthSciences, KPJ Healthcare University College, 71800 Nilai, Negeri Sembilan, Malaysia. Email: izham@kpjuc.edu.my |
| ABSTRACT |
Background and objectives:The Anterior cruciate ligament (ACL) is one of a pair of ligaments in knee which provides stabilization and guiding of joints. There are varieties of graft sources have been used for ACL reconstruction over the past 30 years. Studies shows that ACL reconstruction and rehabilitation is widely conducted in other Asia countries and none were done in KPJ Seremban Specialist Hospital. Hence, this study is to determine the outcome of physiotherapy rehabilitation on ROM, pain level and muscle strength following ACL reconstruction patient in KPJ Seremban Specialist Hospital.Methods: Cross-sectional retrospective study, secondary data collection whereby studies are carried out at one time point or over a short period.Checklist form was used to determine the physiotherapy assessment and interventions. Results: A total of 122 subject were involved in this study. 88.3% male and 11.7% females undergone ACL reconstruction. Most common physiotherapy intervention used are IT and cryotherapy (90%) and combination of strengthening and mobility exercises (94.5%) and there is no significant difference in both intervention groups (p>0.05). Conclusion: Studies conducted shows there is no significant difference in the evaluation of range of motion of knee, pain scale and muscle strength could be due to the intervention used were not particular and commonly used.
Keywords: Anterior Cruciate Ligament, Physiotherapy Rehabilitation.
| Received on 23rd November 2019, Revised on 30th November 2019, Accepted on 9th December 2019 |
DOI:10.36678/ijmaes.2019.v05i04.005
INTRODUCTION
The anterior cruciate ligament (ACL) is a key structure in the knee joint, as it resists anterior tibial translation and rotational loads1. It is one of the most frequently injured structures during high impact or sporting activities. The ACL does not heal when torn, and surgical reconstruction is the standard treatment especially in the field of sports medicine2. The ligament is inserted medially to the anterior intercondylar of the tibia attaching partially with anterior lateral meniscus way up posteriorly, twisting on itself and spreading out to posterior medial aspect of the lateral femoral condyle1,3.Injuries to the ACL is one of the most common and annihilating knee injuries primarily derived as the result of sports involvement apart from normal lifestyle. Studies reported, 50 to 80% of ACL injury are non-contact type are divided into four categories, namely the environmental, anatomical, hormonal as well as the biomechanical4.These injuries usually lead to excess accumulation of synovial fluid in or around the knee joint which commonly known as joint effusion. Based on previous study,ACL injury also contributes in weakness of quadriceps muscle and reduce functional performance. Evidence shows that surgically advances in fixationmethods and graft construction techniques have dramatically improved the outcomes of anterior cruciate ligament (ACL) reconstruction.Success rate of primary ACL reconstruction has been reported to range from 75% to 93% with excellent results on relief symptoms, restoration of functional stability, and early return to normal activity levels5,6,7,8. Assortment of graft sources like autografts, allografts and synthetic have been used for ACL reconstruction to improve function and ACL deficient knee4,7,8. Physiotherapy rehabilitation on post operative ACL reconstruction is vital and crucial in order to regain functional abilities. Restore joint range of motion, regain muscle strength and reduce pain are the physiotherapy objectives on post operative ACL reconstruction5,6,8. There are numerous intervention used to ensure the successful of post operative rehabilitation. Electro physical agents were used to manage the pain and active muscle contraction were introduced immediately in order to gain muscle strength, restore knee function and gaining maximum capabilities. The interventions usedmay be adapted depending on the equipment availability at each facility, the progression outcomes of an individual’s. Therefore, the plan of treatmentis best to be individualized for optimal return to activity. Hence, the objective of this study is to determine the outcome of physiotherapy rehabilitation on ROM, pain level and muscle strength of patients following ACL reconstruction.
METHODOLOGY
This was a cross-sectional study assessing secondary data kept at the Record Department of KPJ Seremban Specialist Hospital. The data collection is using a set of structure checklist consists of 3 section. Section A is about the demographic data includes age, gender and race.Section B, pertaining to physiotherapy pre and post assessment on Range ofMotion (ROM) of knee in a numerical form (0 degree to 135 degree), pain score using Numerical Rating Scale (NRS of 0 to 10) and Manual Muscle Testing (MMT grade 0 to 5)10,11,12. Section C is regarding types of physiotherapy intervention that used in managing post operative ACLpatients. The data was descriptively analyzed to determine the frequency of demographic data, types of physiotherapy intervention. The one way ANOVA was used to determine any significant difference between physiotherapy outcomes and treatment interventions. This study obtained the approval of study ethics from KPJ Healthcare University Research &Ethical Committee and KPJ Seremban HospitalResearch & Quality Innovation Committee.
RESULTS
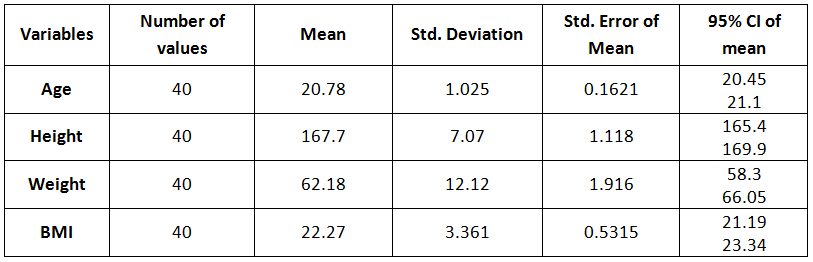
A total of 111treatment card were involved in this study. Most of treatment card assessed were male (88.3%) and the remaining 11.7% was females. The highest number of subject underwent ACL reconstruction were between 25 – 29 years old (56.7%) and 43.3% were 30 – 35 years of age category (Table 1).
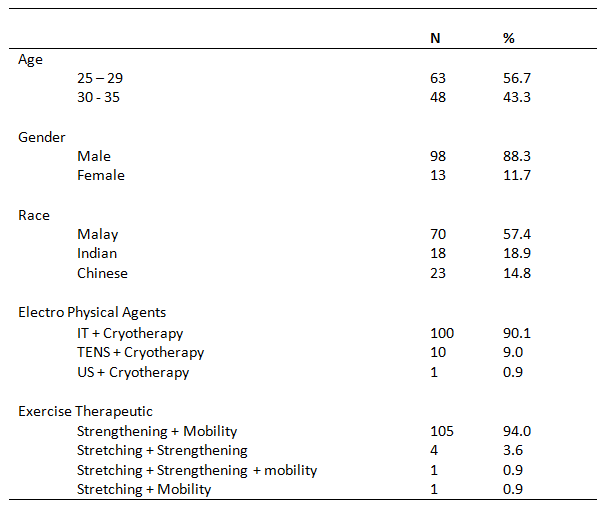
Most of the evidence available on usage of electro physical in post ACL reconstruction was inconclusive5,10. However, the utilization of electro physical agents in managing the post surgery pain indicate a positive outcome 5,10. An increase in local blood circulation has beneficial effects of electrotherapy on post-surgical acute pain and swelling10. The choice of type electro physical agents was merely on therapist clinical experience and availability of equipment. The types of electro physical agents used varies and the utmost choice of treatment were a combination of Interferential Therapy (IT) & Cryotherapy, TENS & Cryotherapy, Ultra Sound (US)& Cryotherapy representing 90.1%, 9.0% and 0.9% respectively. There is no statically difference between all electro physical agent groups but relatively, there is an improvement of post intervention pain score regardless the type of electro physical agents used (Table 2).
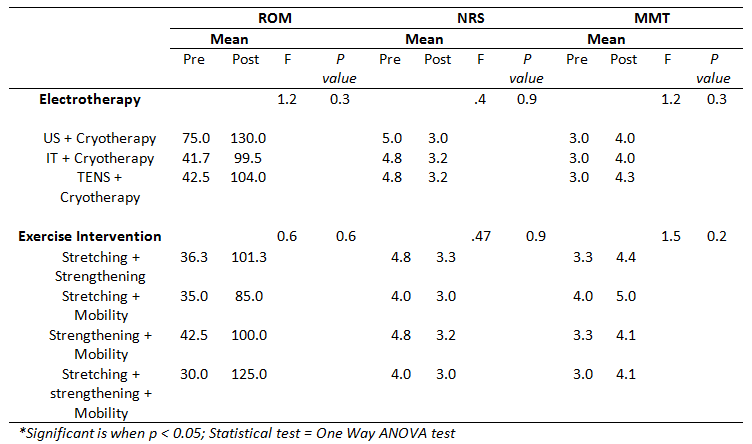
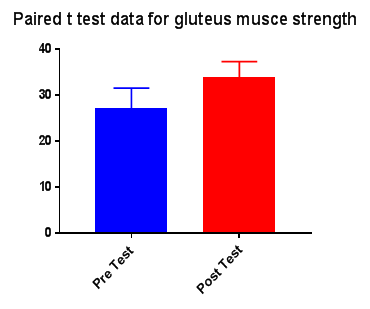
The usage of electro physical agents and exercise intervention has been in tandem for post ACL surgery5. There were numerous available evidence suggest such combination and it offered comfort and faster recovery. The combination of strengthening and mobility exercises werethe commonest (94.5%) active approach used in KPJ Seremban Specialist Hospital. Statically, there’s no significant difference between exercise groups but relatively all groups indicate an increase of strength and joint range motion at post surgery (Table 2).
DISCUSSION
Anterior Cruciate Ligament (ACL) injury occurs not only among athletes but also among sedentary adults and reconstruction has been evolved over the pass thirty years recommended for patients with functional instability either with sporting activity or activities of daily living. Interventions used in treating post-operative ACL patient in KPJ Seremban Specialist Hospital are electro physical agents and exercise therapy.Electro physical agents has an important role in physiotherapy interventions.
The basic principles on which electrotherapy function is remain simple through a wide range of applications that can be derived in acute patient care.Previous study has proven that the application of an external energy to the tissues can result in the activation, stimulation or enhancement of physiological activity in particular tissues and seems suitable to be used for acute condition5,10.Exercise interventions are widely used and belief able to restore functional capabilities and ensure faster return to work. The current ACL rehabilitation emphasizeson the importance of immediate muscle contraction, gaining joint motion and early weight bearing in order to ensure early return to functional abilities.Most of the available evidence indicate significantresults of exercise intervention following early reconstruction procedure conducted 5,6,9,10,. The appropriate graft choice for ACL reconstruction remains controversial however it has no significant effects on the rehabilitation outcomes. An early active rehabilitation seems crucial and aides the faster recovery and shorten the duration return to daily life6,7,8.
The tools used to measure the outcomes seems to be subjective in nature but the reliability of such measurement is acceptable and appropriate10,11,12. The results of this study were not comparable in gender due to small number of ACL reconstruction among female. Furthermore, it is not the scope of study to determine the difference of outcome among gender group.
Ethical Clearance: An initial application was addressed to Research Ethics Committee, KPJ Healthcare University College, Nilai, Malaysia and approval received for conduct of this study with reference number KPJUC/RMC/BPT/EC/ 2018/139, Dated 21/05/2018.
Conflict of interest: There was no conflict of interest on conduct of this study.
Fund for the study: The fund for the study was granted by KPJ Healthcare University College, Nilai, Malaysia.
CONCLUSION
The rehabilitation intervention conducted by rehabilitation department of KPJ Seremban Specialist Hospital is consistent with previous available evidence. A standardized outcome measured with more objective measurement should be introduced in order to have a more accurate reading. Future study using clinical trial should be conducted in order to determine the effectiveness of physiotherapy rehabilitation on ACL reconstruction.
REFERENCE
- Kiapour, A., & Murray, M. (2014). Instructional Review : Knee Basic science of anterior cruciate ligament injury and repair ;3(2) : 20-31.
- Duthon, V. B., Barea, C., Abrassart, S., Fasel, J. H., Fritschy, D., & Menetrey, J. (2006). Anatomy of the anterior cruciate ligament. Knee Surgery, Sports Traumatology, Arthroscopy ; 14 (3) : 204 – 213.
- Markatos, K., Kaseta, M., Lallos, S., Korres, D., & Efstathopoulos, N. (2013). The anatomy of the ACL and its importance in ACL reconstruction : 747 – 7.
- Allen F. Anderson, MD, Robert B. Snyder, MD, and A. Brant Lipscomb, Jr., MD. (2001). A Prospective Randomized Study of Three Surgical Methods. The American Journal of Sports Medicine; 29 (3): 272 – 279.
- Tovin, B. J., Wolf, S. L., Greenfield, B. H., Crouse, J., & Woodfin, B. A. (1994). Comparison of the effects of exercise in water and on land on the rehabilitation of patients with intra-articular anterior cruciate ligament reconstructions. Physical Therapy ; 74 (8) : 710 – 719.
- Heijne, A. & Werner, S. (2010). A 2-year follow-up of rehabilitation after ACL reconstruction using patellar tendon or hamstring tendon grafts: a prospective randomized outcome study. Knee Surg Sports Traumatol Arthrosc : 18: 805.
- Allen F. Anderson, MD, Robert B. Snyder, MD, and A. Brant Lipscomb, Jr., MD. (2001). A Prospective Randomized Study of Three Surgical Methods. The American Journal of Sports Medicine; 29 (3): 272 – 279.
- Freedman K.B., Damato M.J., Nedeff D. (2003). Arthroscopic Anterior Cruciate Ligament Reconstruction: A Meta analysis Comparing Patellar Tendon and Hamstring Tendon Autografts. The Americal Journal of Sports Medicine: 13 (1); 2 – 11.
- Holsgaard-Larsen, A., Jensen, C., Mortensen, N. H. M., & Aagaard, P. (2014). Concurrent assessments of lower limb loading patterns, mechanical muscle strength and functional performance in ACL-patients – A cross-sectional study. Knee; 21(1) : 66 -73.
- Reid, A., Birmingham, T. B., Stratford, P. W., Alcock, G. K., & Giffin, J. R. (2007). Hop Testing Provides a Reliable and Valid Outcome Measure During Rehabilitation After Anterior Cruciate Ligament Reconstruction. Physical Therapy ; 87 (3) : 337 – 349.
- Hartrick, C. T., Kovan, J. P., & Shapiro, S. (2003). The Numeric Rating Scale for Clinical Pain Measurement: A Ratio Measure? Pain Practice; 3(4) : 310 – 316.
- Moisala A.S., Jarvela T., Kannus P., Jarvinen M. (2007). Muscle Strength Evaluations after ACL Reconstruction. Int J Sports Med; 28(10) : 868 – 872.
| Citation: |
Izham Zain, Nabilah Ahmad, Nanthenii M.K, Asyiqin (2019). The outcome of physiotherapy rehabilitation following ACL reconstruction at KPJ Seremban Specialist Hospital , International Journal of Medical and Exercise Science, 5 (4); 651-655.