2,5Assistant Professor, Madha College of Physiotherapy, MadhaNagar, Kundrathur, Chennai, T N, India.
3,4Professor, Faculty of Physiotherapy, Dr.M.G.R.Educational and Research Institute, Maduravoyal, Chennai, Tamil Nadu, India.
6BPT Student, Faculty of Physiotherapy, Dr. M. G. R. Educational and Research Institute, T N, India.
Corresponding Author
1Assistant Professor, Faculty of Physiotherapy, Dr. M. G. R. Educational and Research Institute, Maduravoyal, Chennai, Tamil Nadu, India. E-mail: sathyaraja.physio@drmgrdu.ac.in
ABSTRACT
Introduction: Trapezitis is an inflammation caused in the Trapezius Muscle which further leads to pain and spasm in the neck. It increases commonly among people who are work at desk and computers, drivers, tailors, painters who uses their neck muscles a lot. MET is an active muscle based treatment approach that involves the voluntary contraction of a muscle in a controlled direction against the counterforce provided by the therapist.
Methodology: This is a comparative experimental study conducted at physiotherapy OPD, ACS Medical College and Hospital. Study duration was 2 weeks with 4 session .Patient aged between 20-45 years. The sampling was chosen on purposive sampling. The pre and post test were Visual Analogue Scale (VAS), Neck Disability Index (NDI) and cervical lateral flexion ROM. In this study, 30 subjects are characterised into 2 groups of 15 subject each .Group A received post isometric relaxation technique and Group B received post facilitation stretching technique.Both pre and post test were measured using VAS,NDI and cervical lateral flexion ROM.Inclusion criteria are age of patient 20-45 years,pain,muscle spasm and tenderness.Exclusion criteria are patient age below 20 years,any cervical injury,recent surgery over cervical region.
Result: On comparing pre and post test for both group on VAS,NDI and cervical lateral flexion ROM,post facilitation streching technique show better result than post isometric relaxation technique in reducing pain,neck disability and improve neck ROM.
Conclusion: The study concluded that post facilitation stretching technique was more effective than post isometric relaxation technique for patient with Trapezitis.
2Saji. V.T, Professor and Principal, Cooperative Institute of Health Sciences, Thalassery, Kannur, Kerala, India.
Corresponding Author:
1Akhila K, MPT Student, Cooperative Institute of Health Sciences, Thalassery, Kannur, Kerala, India. Email Id: akhilasuresh1997@gmail.com
ABSTRACT
Background of the study: Osteoarthritis is one of the most common disease causing disability and functional problems. Exercise therapy has recently become popular. It can improve the general function of the body and activities of daily living by enhancing the range of motion (ROM) and muscle strength of patients having osteoarthritis. Objective of the study was to establish or review existing studies evaluating the effectiveness of exercises performed on unstable surfaces on pain, lower extremity function, balance and strength in post-menopausal female patients with tibiofemoral osteoarthritis.
Methodology: Various articles from databases like Pub Med, Google scholar, science direct, research gate has been collected for analysis. It has retried through search by using keywords of osteoarthritis, post menopausal women, manual muscle test, pain and balance. Total 20 articles were included in the study and based on their findings a review was made.
Result: Strengthening of the hamstring in addition to strengthening of the quadriceps is beneficial for improving subjective knee pain, range of motion, and decreases the limitation of functional performance of patients with knee osteoarthritis.
Conclusion: The present literature review concludes that exercise using unstable surface improved the symptoms of patient with osteoarthritis
Keywords: Osteoarthritis; Range of motion; Lower extremity function; Balance
1MPT Student, Faculty of Physiotherapy, A.C.S. Medical College and Hospital Campus, Dr. MGR. Educational and Research Institute, Deemed to be University, Chennai,Tamil Nadu, India
2Assistant Professor, Faculty of Physiotherapy, A.C.S. Medical College and Hospital Campus, Dr. MGR. Educational and Research Institute, Deemed to be University, Chennai, Tamil Nadu, India
ABSTRACT
Background of the Study: Low back pain is common condition during the pregnancy. The increased Lordosis of pregnancy combined with the effect of relaxin on the joint of the pelvis and the weight of gravid uterus results on anterior shift in the center of gravity which all together contributes to complain of low back pain during pregnancy. The main objective of the study is to find out the effects of sitting pelvic tilt exercise and pelvic floor exercise during third trimester in Primigravida on low back pain.
Methodology: This was an experimental study with pre and post intervention. The study setting was done in ACS medical college and hospital. Total 30 Primigravida women aged between 20-35 years selected by random sampling method. The selected women followed sitting pelvic tilt exercise and pelvic floor exercise for 8 weeks. Three sets per day with 10 repetitions per set. The outcome measures were determined by Numerical Pain Rating Scale (NPRS). Primigravida (third trimester) Numerical pain rating scale score (4-6).
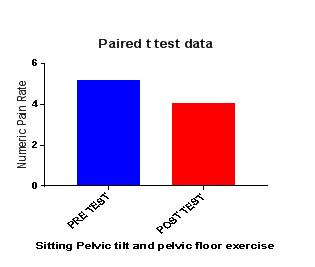
Result: The study revealed that sitting pelvic tilt and pelvic floor exercise shows better reduction in pain on comparing the pre-test and post-test values in low back pain on Primigravida women. It showed a significant difference in mean value (1.13) at p value < 0.0001.
Conclusion: The study concludes that sitting pelvic tilt exercise and pelvic floor exercise was effective on reducing pain intensity. Hence sitting pelvic tilt exercise and pelvic floor exercise is effective therapeutical option for the management of low back pain among Primigravida on third trimester.
Keywords: Primigravida; Third trimester; Sitting pelvic tilt exercise; Pelvic floor exercise; Low back pain.
Received on 04th January 2022, Revised on 12thFebruary 2022, Accepted on 25thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.001
INTRODUCTION
Pregnancy is a time of tremendous
musculoskeletal, physical and emotional changes, but yet a condition of
wellness. Low back ache is one of the most common complaints during gestation,
affecting 48-90 per cent of women1,2,3. During pregnancy lot of
physiological and musculoskeletal changes takes place for the development of
fetus 4. In pregnant women, it is most common and significantly affecting
their daily activities5. As the fetus grows, a women’s abdominal
wall stretches to accommodate the expanding womb. Abdominal muscle stretched to
the point of their elastic limit by end of pregnancy6.
The center of gravity shifts
upward and forward because of enlargement of the uterus and breast. This
requires postural compensation for balance and stability during pregnancy, the
hormone relaxin is present ten times more than its normal concentration in
female body. Relaxin also causes abnormal motion in many other joints of body,
causing inflammation and pain 7, 8.
Lumbar Lordosis that develops at later
stages of pregnancy, gravity shifting, postural changing, and workload lead
towards pregnancy related low back pain1. Increased Lordosis of
pregnancy combined with the effect of relaxin on the joint of the pelvis and
the weight of the gravid uterus which results anterior shift in the center of
gravity.
All contribute to complaint of
low back pain during pregnancyHormonal changes that occur during
pregnancy causes softening of ligaments and the joints, particularly of the
pelvis, to enable the fetus to pass through the birth canal more easily9.
This results in increased joint looseness and decreased stability. This, in
conjunction with lengthening of the abdominal muscles, compromises the
stability of the spine and results in excess mobility of the joints. This may
be the cause of pain in the lower back and posterior pelvis. Low back pain
during pregnancy was most frequently reported in the third trimester of
pregnancy (40.7%) and was often reported to be in lower back area (71.2%). One
third of them will suffer from severe pain which will reduce their quality of
life10, 11.
The majority of women affected
are Primigravida 80% of pregnant women suffering from low back pain 12,13
, Pelvic floor muscles training is safe and effective technique that restore or
develop pelvic floor muscles strength and help women control this musculature
during pregnancy14. The sitting pelvic tilt exercise is one of the
mobility exercise which seems to strengthen or increases the flexibility of
muscles needed to compensate for increase abdominal mass an thereby maintaining
normal posture. The pelvic floor exercise is used in this study was designed to
coactive superficial and deep core muscles thus, results in significantly
better improvement in pain15.
There are two simple exercise
that can be safely given to women during pregnancy- pelvic floor and pelvic
tilt exercise. This study was performed to assess the effect of sitting pelvic
tilt exercise and pelvic floor exercise on low back pain during the third
trimester in Primigravida. Exercise is given in sitting position is called
sitting pelvic tilt exercise, the pelvic floor exercise is also given in
sitting position during third trimester.
Aim of the study: To
investigate the effects of sitting pelvic tilt exercise and pelvic floor
exercise during third trimester in Primigravida on low back pain.
Need of the study:
Pregnancy related low back pain has become the common issue for women in the
last trimester which affect the quality of life during pregnancy. Sitting
pelvic tilt exercise and pelvic floor exercise which approaches for low back
pain during the third trimester. So this study is done to find out the effects
of these exercises in reducing low back pain.
METHODOLOGY
This was an Experimental study
with Comparative Pre and Post type.
Study Setting: done at A.C.S Medical College and hospital,
Velappanchavadi, Chennai-77.Sample Size for this study was 30 Primigravida and
intervention duration was 8 Weeks.
Inclusion Criteria for this study
were Primigravida women third trimester with low back pain, Age 20-35 Years,
Numerical pain rating scale (4-6), Subjects willing to participate. Material
Used for this study were hard chair, scoring sheet. Outcome Measure for the
study was Numerical Pain Rating Scale.
Procedure: Subjects would be selected based on selection criteria.
Numeric pain rating scale consists of 10 scores. The women should choose
corresponding score according to their level of pain. The intervention included
sitting pelvic tilt exercise and pelvic floor exercise for low back pain in
participants respectively.
Intervention
Sitting pelvic tilt exercise: Subjects will be asked to sit in
chair with a straight backrest with feet flat on the floor at hip’s width
distance. Subjects will be asked to tilt the pelvis back and draw in umbilicus.
Holding time is three to ten seconds. Duration of the program was three sets
per day. Each set consist ten repetitions.
Pelvic floor exercise: Sit and lean slightly forward with straight back. Squeeze and lift the muscles in gentle manner then hold the squeeze for 8 seconds. Duration of the program was three sets per day. Each set consist ten repetitions.
Data Analysis: The collected data were tabulated and analyzed using both descriptive and inferential statistics. All the parameters were assessed using statistical package for social science (SPSS) version 24. Paired t-test was adopted to find statistical difference within the groups.
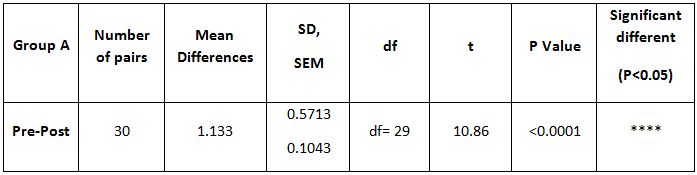
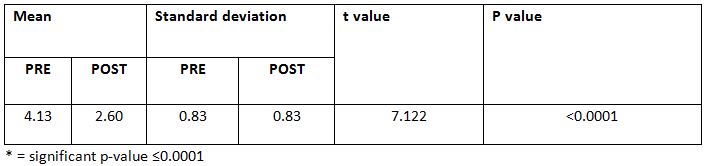
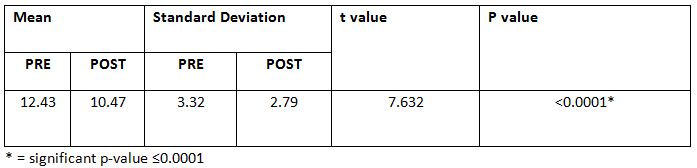
Table-1 Comparison of numeric pain rating scale (NPRS) score within the group in pre and post test
The above table reveals the mean difference, standard deviation (S.D), t-value and p- value of the low back pain between the pre-test and post-test within the group. Based on low back pain, it shows that there is statistically significant difference between pre-test and post-test value within the group p<0.0001.
Graph-1: Graphical representation of comparison on numeric pain Rating scale within the group between pre and post test
RESULT
A total sample of 30 subjects was
included in the study with the age group between 20 to35 years. The patients
were selected from A.C.S. Medical College & Hospital, Chennai-77. These
patients were inquired about the characteristics of pain and functional
activity. The study revealed that sitting pelvic tilt and pelvic floor exercise
showed better reduction in pain intensity. On comparing the pre-test and
post-test values in low back pain on primigravid women shows significant
difference in mean value (1.133) at p value < 0.0001.
DISCUSSION
The present study was designed to investigate the efficacy of two
exercise for Primigravida women with low back pain during third trimester. The
sitting pelvic tilt exercise and pelvicfloor exercise snows effectiveness in
reducing pain and have improvement in functionalability. Low back pain commonly
occurs during pregnancy. Both sitting pelvic tilt exerciseand pelvic floor
exercise is very simple and effective exercise. In our study we are
improvingthe strength or lower back region and thereby reducing pain in women
with low back pain.30 primigravida were selected by random sampling method.
The pain is measured using Numerical Pain Rating Scale. This study
supports the finding on Yana Richens et
al, (2015) 16 reported back ache first developing during the
5th-7th month of pregnancy. Symptoms are often reported
by women to be worse in the evening and in third trimester and suggested that
pelvic tilting and pelvic floor exercise which can be safely given during
pregnancy. Areerat s et al., (2002)3
reported the sitting pelvic tilt exercise during third trimester in
primigravida could decrease pain intensity without incidence of preterm labor,
low birth weight or neonatal complication.
A study reported that
sitting pelvic tilt exercise during third trimester in Primigravida did not
only reduce pain in numerical pain scale and also decrease episodes of insomnia
and sleep disorders. Another study stated that on comparing non exercised
pregnant women with prenatal exercised pregnant women decreases the severity of
low back pain16,17.
Low back pain intensity was increased in control group. The exercise
group shows significant reduction in the intensity of low back pain after
exercise. Exercise during second half of the pregnancy significantly reduced
the intensity of low back pain. Physical activity and exercise during pregnancy
promotes physical fitness and may prevent excessive weight gain18.
Exercise may reduce the risk of gestational diabetes, preeclampsia and
cesarean deliveries and exercise
offers significant benefits in women reducing low back pain and pelvic pain,
specifically beneficial effects in severity of pain and thus on functional
abilities and quality of life of the women affected. The sitting pelvic tilt
exercise and pelvic floor exercise has been suggested as his management for low
back pain in pregnancy 19, 20.
The statistically report reveals there is a significant difference in
Numeric pain Rating scale scoring (P<0.0001) in subjects who undergone
sitting pelvic tilt exercise and pelvic floor exercise. Finally the sitting
pelvic tilt exercise and pelvic floor exercise can be used as simple and
effective treatment on reducing low back pain among third trimester
Primigravida.
Ethical
clearance: There
was no risk of conducting this study.Ethical clearance was
obtained from the ethical Institutional Review Board of
Faculty of Physiotherapy, Dr.
MGR. Educational and Research Institute, Chennai with reference No. A23/PHYSIO/IRB/2018-2019 approval letter dated 08/01/2019.
Conflicts
of Interest: There is no conflict of
interest to conduct this study.
Fund for the study: This is self-funded study.
CONCLUSION
The study revealed that sitting pelvic tilt Exercise and pelvic floor
exercise was effective reducing pain intensity, hence concluded that sitting
pelvic tilt exercise and pelvic exercise is effective therapeutical option for
the management of low back pain for exercise among Primigravida in third
trimester.
REFERENCE
Singh N, Desai OP. Prevention and management of low backache in pregnant women through the use of exercise program and education booklet. Indian Journal of Occupational Therapy 2008; 39(3):65‐72.
Kristiansson P Back pain during pregnancy: a prospective study, Spine (1996); 15; 702-709.
Areerat S Effect of the sitting pelvic tilt exercise during the third trimester in Primigravida on back pain. J Med Association Thailand, (2002); 85:107-10.
Osgaard HC, Zetherstrom G Reduction of back & post pelvic pain inpregnancy spine (1994); 19:984-900.
Kashanian M, Akbari Z, Alizadeh MH. The effect of exercise on back pain and lordosis in pregnant women. International Journal of Gynecology & Obstetrics 2009; 107(2): 160‐1.
Mogren IM, Pohjanen Al. Low back pain and pelvic pain during pregnancy: prevalence and risk factor.Spine:2005;30: 983-91.
MacEvilly, M., Buggy, D., (1996). Back pain and pregnancy: a review. Pain, 64(3), 405-414.
Calguneri et al., 1982; Szlachter et al., 1982; Brynhildsen et al., 1998 Changes in joint laxity occurring during pregnancy.
Sahota PK, Jain SS, Dhand R (2003) Sleep disorders in pregnancy. Curr Opin Pulm Med 9: 477-483.
Ming WS (2004) Low back pain during pregnancy: prevalence, risk factors and outcomes. Obstetrics and gynecology 4: 65-70.
Sabino J, Grauer JN (2008) Pregnancy and low backpain, Current reviews in musculoskeletal medicine 1:137-141.
Pennick VE Interventions for preventing and treating pelvic and back pain in prenancy. Cochrane Database of systematic Reviews 2013 Aug 1; (8): CD0011391: D001139.
Saz HMT, Zadeh NK, Shamseldini A,Hosseini M (2007) Prevalence of low back pain in gnant women who are attended to Baqitallah hospital. J Army Uni med Sci lR ran 5: 1293-1297.
Salvesen KA, Morkved S. Randomised controlled trial of PFMT during pregnancy BM); 2004: 329:378-80.
Ayanniyi O, Sanya A.O, Ogunlade S.O, Prevalence and Pattern of Back Pain among Pregnant Women Attending Ante-Natal Clinics in Selected Health Care Facilities, African Journal of Biomedical Research, Vol. 9 (2006); 149-156.
Yana Richens et al Lower back pain during pregnancy: advices and exercise for women. British Journal of Midwifery, (2015), Vol. 18, No. 9.
Deepthi et al., Does Sitting Pelvic Tilt Influence Quality of Pain in Low Back Pain and Quality of Sleep among Primigravida Indian Mothers. J Women’s Health Care 2016, 5:5.
Margie H Davenport et al Exercise for the preventing and treatment of low back, pelvic girdle and Lumbo pelvic pain during pregnancy: a systemic review and meta- analysis(2019), Br J Sports Med, 2019 Jan; 53(2):90-98.
Garshasbi et al. The effect of exercise on the intensity of low back pain in pregnant women, Int J Gynaecol Obstet .2005 Mar; 88(3):271-5.
Iva Sklempe Kokic 1, Marina Ivanisevic, Melita Uremovic,et al Effect of therapeutic exercises on pregnancy-related low back pain and pelvic girdle pain: Secondary analysis of a randomized controlled trial J Rehabil Med. 2017 Mar 6; 49(3): 251-257.
Citation: Indhu.K, Jayabharathi.R.Effects of sitting pelvic tilt exercise and pelvic floor exercise during third trimester in primigravida on low back pain, International Journal of Medical and Exercise Science, March 2022; 8(1); 1165-1171.
1AssistantProfessor, East Point College of Physiotherapy, Bangalore, Karnataka, India Mail id: prachijphysio@gmail.com
Co-Authors:
2,3Professor, East Point College of Physiotherapy, Bangalore, Karnataka, India
ABSTRACT
Background of the study: This examination clarifies about the normal weight an understudy needs to convey to school. The pinnacle development happens during pubescence and the development of the affixed skeletal framework stops around 16 – 18 years for guys. The greater part of the investigations on the impact of burden carriage has been centered around patches and climbers fully intent on working on the strategies of burden carriage.
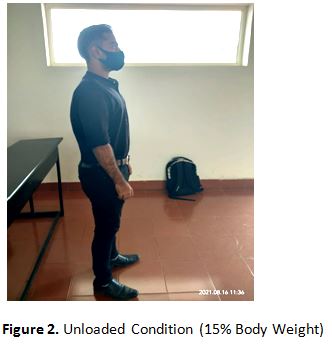
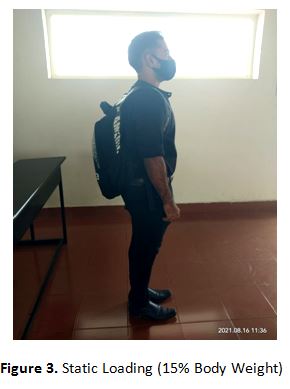
Methodology: This is an observational investigation with 50 male subjects included. With static and dynamic stacking with 15% body weight and changes in stride design in the two circumstances were caught. Subjects were on their own control where gauge or dumped pose is contrasted and act under two distinctive trial stacking conditions. Subjects were weighed with and without their school packs on the one set off aligned electronic scale.
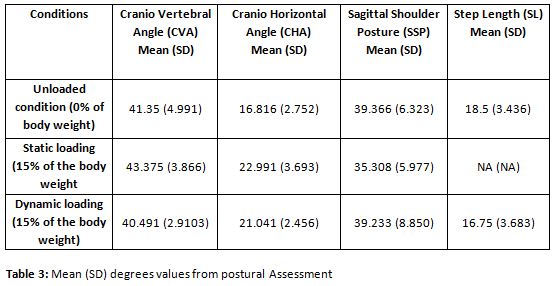
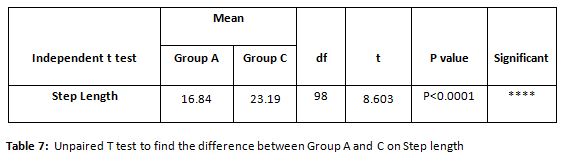
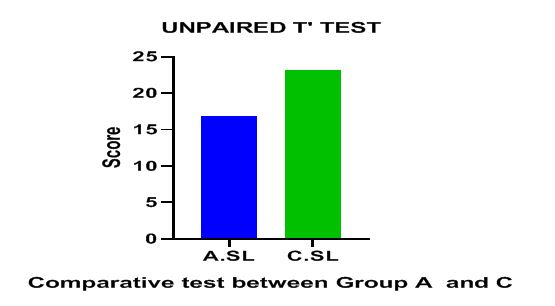
Result: The mean upsides of Craniovertebral Angle (CV), Craniohorizontal (CH) point and Sagittal Shoulder act expanded in all trial load conditions in examination with dumped state. The mean upsides of Step Length (SL) decreased in unique stacking when contrasted with dumped condition while it was not appropriate if there should arise an occurrence of static stacking. No huge contrasts were found in CH Variance between the dumped condition and conveying school sacks weighting 15% body weight while in static stacking the CH Variance was expanded to practically twofold when contrasted with no heap and dynamic burden condition.
Conclusion: This experimental study supports that dynamic loading of the student with 15% of body weight, leads to significant change in cervical and shoulder posture compared to static loading with 15% of body weight and unloaded condition.
Received on 12th July 2021, Revised on 18th August 2021, Accepted on 26th August 2021, DOI:10.36678/IJMAES.2021.V07I03.003
INTRODUCTION
The word rucksack was begat in the U.S. in 1910’s. Rucksack is a proper method of conveying load of spine, intently and evenly while keeping up with dependability. The Backpack is one of the few from of manual burden carriage that gives flexibility and is frequently utilized by climbers, hikers and troopers, just as school kids. However, there is developing public worry that over-burden youngsters and juvenile’s knapsacks might prompt the improvement of back torment and other musculoskeletal wounds. Data got from these investigations may duplicate to school kids. Stance in juvenile can be influenced by both inward and outer impacts, which might make young adult more vulnerable to injury. Contemplating postural reactions to burdens will help us to understanding the effect of conveying school packs on kids. At the point when burden is situated back to the body as knapsack it changes pose on account of changes to focus of gravity1, 2.
The body attempts to keep the focal point of gravity between feet, so with a bag, the storage compartment is in a more forward position, putting unusual power on the spine, load conveyed in a backpack shift the focal point of gravity behind the body to equalize, the focal point of the gravity of the body in addition to the load is moved back over base of the feet. The specialists demonstrated that conveying backpack lead protrusion of head to the forward direction. These progressions in arrangement of the neck can produces strain of cervical joints 3, 4.
Conveying back loads by youngsters has been connected with spinal agony, and the measure of postural change created by load carriage has been utilized as a proportion of the possibility to cause tissue harm. Back torment in kids gives off an impression of being more normal than was recently suspected. Studies have shown that 10% to 30% of sound youngsters experience back torment by their teen. Consequently examination to postural reactions to stack conveying will assist us with understanding the effect of school knapsack on youngsters5-7.
To decrease the event of musculoskeletal agony a proactive, preventive methodology utilizing ergonomics mediation has been proposed by certain scientists. For instance, school packs plan, school spot, furniture, and apparatuses. Managerial controls are choices made by school staff, medical care experts and others (specialists, school overseers, and guardians or parental figures) to lessen the term, recurrence and seriousness openness to existing risks. They additionally pass on the dangers set up however endeavors to decrease the impacts on the young (for example ensuring the heaviness of the rucksack doesn’t surpass 15% of the body weight, checking the adolescent stance when wearing the knapsack). Work practice controls are self-guided, self-started systems utilized by understudies to guarantee protected and legitimate methods while doing exercises (for example utilizing the two ties, affixing the lashes yet not very firmly). This load of methodologies or controls target decreasing the weight on musculoskeletal framework8, 9.
The limitation of the most extreme load to 15% of the body weight is one of the fundamental controls. Anyway some different creators have suggested that sack weight ought not to surpass 15% of the body weight. In this investigation we are attempting to decide if the heaviness of the rucksack (15% of body weight), its situation on the spine or time conveyed influenced youths cervical and shoulder act. None of the scientists till date have examined reactions of cervical and shoulder act after static stacking and after unique exercises with 15% of body weight. In addition, attributable to anthropometrical contrasts among western and Indian offspring of comparable examination done there are not straightforwardly appropriate to Indian kids 10.
Purpose of the Study: There is need of this investigation so it can give us data about the normal weight a kid needs to convey to school. Subsequently if preventive measures can be acquaint now with the respect with safe burden carriage in undergrads, it won’t just serve to item youngsters while they are as yet growing, yet will likewise guarantee, that the standards they adapt now are brought through to work place as grown-ups and to address the very example deviations which happen in the youngsters because of weighty burden.
Aim & Objectives : Objectives of the study were to examine the changes in Cervical Lumber & Shoulder posture in college children with Dynamic Loading (15% of body wt.); also, to examine the changes in cervical Lumber & Shoulder posture in college children with static Loading (15% body wt.). And to analyses the gait pattern after back loading in college children.
Growth: Growth applies powers to the spine, the extent of which differs with the pace of development. Since the development speed is most elevated in newborn child and youths, it is normal that the subsequent powers applied to the spine are most noteworthy at these ages. Despite the fact that they are not more noteworthy, the powers that outcome from development might change spinal design since they are applied throughout extensive stretches of time. In ordinary spinal development, foremost and back development and side to side development are adjusted. The outcome is stretching of the spinal segment with moderately little change in its gross forms. Assuming, nonetheless, a pathology condition causes deviated development, the power vectors change and cause deformation.
Adaptability The pediatric spine can adjust to applied anxieties substantially more promptly than can the grown-up spine. “This is identified with development potential, the lower modulus of flexibility, and unmistakable rebuilding capacity.
Malleability: as well as being versatile, which suggests in dynamic interaction, the pediatric spine likewise is generously pliable. Pliability, a uninvolved interaction, suggests that the spine might be disfigured with the use of powers outside to the spinal segment.
Hypermobility: The physiologic scope of movement of the pediatric spine is extensively more noteworthy than that of the grown-up spines. This is the consequence of contrasts in ligamentous limitations and direction of the feature joint.
Weak Growth Plate: The development plate is the most fragile connection in the hub skeleton when it is exposed to tractable powers. This has significant ramifications for the sorts of injury probably going to happen in the pediatric spine. Odontoid wounds typically happen through the actual plate, situated close to the foundation of the odontoid cycle.
METHODOLOGY
Total 50 students aged between 17-20 years of BPT First Year was participated in the study. Participants with fever, systemic illness, cervical injuries, scoliosis or Kyphosis or congenital deformity were excluded from this study. Participants with complaint of pain were stopped for testing procedure.
Inclusion Criteria: Students should be aged between 17-20 yrs. Height, Body Weight should almost be similar, weight of the bag should be equal, lifestyle variation.
Exclusion Criteria: Scoliosis or Kyphosis, Injury, Fever, Systemic illness, any congenital deformity.
Study Procedure: Participants were weighed with and without their school packs on the one set off adjusted electronic scale (Beurer scale, precise to be inside 0.1 kg to 120 kg). Standing stature was estimated against an estimating tape got to divider. One school pack was utilized for every one of the exploratory conditions. The school sack had two movable cushioned shoulder ties, two compartments and no midriff or chest pressure lashes. Scopes of loads of 2 kg, 1 kg, 500 gm, 100gm, and 50 gm were utilized for the exploratory burden conditions.
The element of loads repeated regular instruction material. One Cannon 7.1 Mega pixels advanced camera was utilized to take actually photos of subject’s sagittal stance. Stand remain with a soul meter level was utilized for mounting the camera. Proportions of cervical and shoulder act were determined structure advanced photos utilizing the digitizing programming (Image Tool UTHCSA variant 3.0 University of Texas Health Service Center, San Antonio, TX).
Design of the study: This was an observational study to compare 2 test load conditions in static and dynamic stage with 15% body weight and were tried noticing the progressions in step design in the two conditions. Subjects were their own control where benchmark or dumped act is contrasted and act under two distinctive exploratory stacking conditions.
Techniques: Clothing was reworked so that shoulders were uncovered. With the subjects in standing stance cement markers were put on four physical tourist spots.
Spinous process of the seventh cervical vertebrae, Midpoint between greater tuberosity of humerus bone, back part of acromion of the scapula, Outer canthus of right eye and right tragus, were noted and were approached to stand serenely with their arms close by in ordinary standing stance.
They were approached to put their weight equitably on the two feet. The horizontal malleoli were put between equal lines, which are opposite to the front facing planes. The subjects gazed straight ahead. Camera was put two meters from the subject’s right side. Photo was taken inside 5 second of taking on the position.
The photos of the subjects were taken without school bag; it was 0% body weight, 15% body weight applied for Static loading and for dynamic activities. Information was examined by advanced programming Image Tool UTHCS version 3.0, University of Texas Service Center, San Antonio.
Data Analysis: Examination of postural points after powerful exercises is finished with static loading with 15% body weight and with 0% body weight. The meaning of changes in information was assessed utilizing rehashed measure examination of difference on each point with which arranged differentiation were made of the dumped condition with every one of two other stacked condition. The study was considered as significant with if p<0.05. The Gait was observed at carrying school bag more than two shoulders comparable to 15% body weight with static and dynamic exercises.
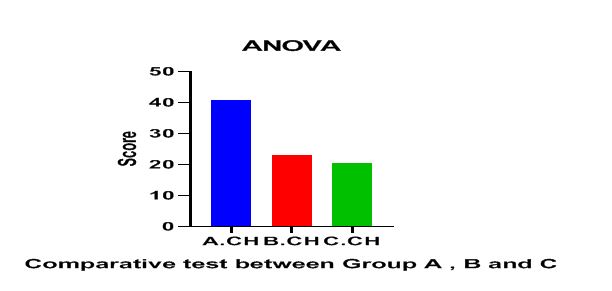
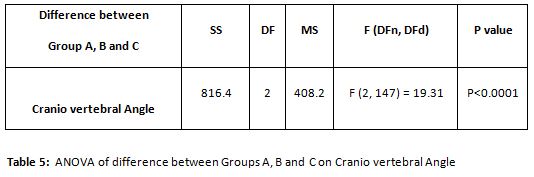
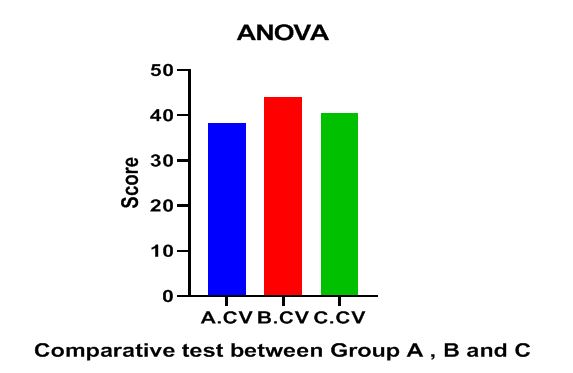
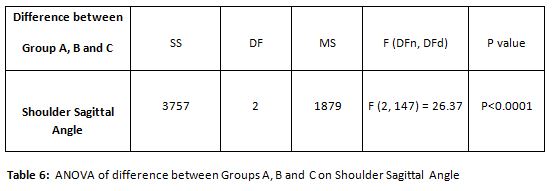
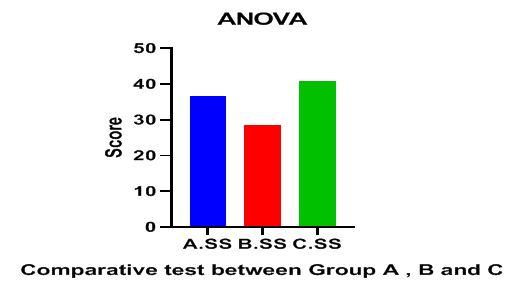
Graph 1: The Cranio-horizontal angle increases in the Group A i.e. Without static loading and it reduces gradually once it is loaded and further more it reduces in the dynamic loading subjects when they start walking.Graph 2: Cranio vertebral angle increases in static loading comparatively more than unloaded group and dynamic loading.Graph 3: Shoulder sagittal angle increases in static loading comparatively more than unloaded group and dynamic loadingGraph 4: The step length (SL) changes in group C than group A, which is unloaded static group.
RESULT
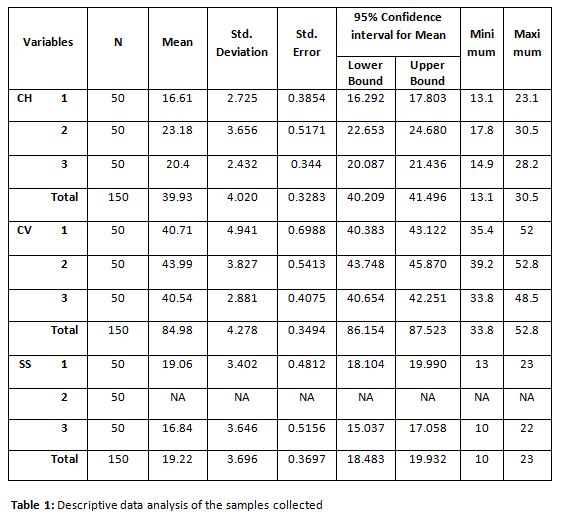
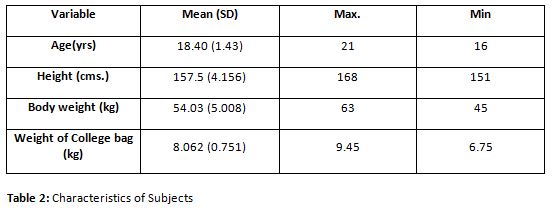
The mean stature and mean load of the subjects enlisted were 157.5cms, 54.34 kg separately. The mean load of the bag which kid conveyed to school was observed as 8.151 kg which was 15% of their body weight. Benchmark esteems were got ten by estimating Craniovertebral Angle, Craniohorizontal Angle, Sagittal Shoulder stance and step length on the dumped condition with 0% of their body weight.
The mean upsides of craniovertebral point diminished in a trial loaded condition in examination with dumped condition. The mean worth of CVA in the dumped state was 40.718 = 4.991, though the mean upsides of CVA while static stacking with 15% of body weight and after unique exercises with 15% of body weight were 43.994= 3.866 and 40.542=2.910 individ-ually. Huge contrasts were found by rehashed proportion of difference (ANOVA) in the CVA between dumped state, static stacking and after powerful exercises with p esteem 0.018 which is more than 0.0001.
Pair insightful correlation was between loaded state and static loading with 15% body weight shows that there is contrast with p esteem 0.0001 and furthermore critical distinction between dumped state and after powerful exercises act with p esteem 0.034. There was no critical contrast was found between static stacking states and after unique stacking exercises pose with 15% body weight load for CVA as p esteem is more noteworthy than 0.0001.
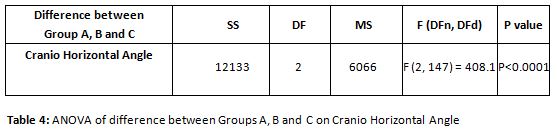
The mean upsides of Craniohorizontal point expanded in every one of the two trial load conditions in examination with dumped state. The mean worth of CHA in the dumped state was 16.61 = 2.75, though the mean upsides of CHA while static stacking and after unique exercises with 15% body weight were 23.186 = 3.693 and 20.4 = 2.456 individually. No huge contrasts was found in CHA between the dumped condition and conveying school sacks weighting 15% body weight while static stacking and after powerful exercises act.
The mean worth of sagittal shoulder act increments in every one of the two trial loads conditions in correlation with dumped state. The mean worth of sagittal shoulder act in the dumped state was 38.324 = 6.323, though the mean upsides of sagittal shoulder pose while static stacking and after unique exercises with 15% body weight were 34.68 = 5.977 and 40.75 = 8.850 separately.
The mean worth of step length diminishes in all trial loads conditions in examination with dumped state. The mean worth of step length in the dumped state was 19.06 = 3.436, though the mean upsides of step length while static stacking isn’t pertinent and after powerful exercises with 15% body weight was 16.84 = 3.683.
DISCUSSION
Shruti. R. Iyer in their examination tracked down that Indian youngsters convey school bags gauging 18.5% of their body weight. Pascoe et al7 in their examination done in America tracked down that mean load of school bag conveyed by school kids in the age gathering of 11-13 years was 17% of their body weight11.
Likewise Negrini et al in their examination done in Italy tracked down that normal burden conveyed by school kids matured 11.29=0.33 was 9.3 kg, which was determined to 22% of their body weight. Conversely, the heaviness of school pack communicated in level of body weight in this examination was observed to be heavier than detailed by Forjuoh SN et al in their investigation done in Texas (6.2% among kindergarteners and 12% among fifth graders)12.
The consequence of this examination uncovered that the greater part of the Indian kids in the age gathering of 17-20 years conveyed school pack weighing between 15% – 18% of their body weight. The mean worth of weight of the school pack conveyed by youngsters was observed to be 8.151 kg which is observed to be 15% of their body weight. The heaviness of the school pack communicated in level of body weight was observed to be reliable with studies done by Shruti. R. Iyer5 and Pascoe et al13.
Likewise J.K Whitefield et al in their examination done in New Zealand College detailed 13.2% of body weight for 3rd grade and 10.2% for 6th grade. Craniovertebral point gives an assessment of head on upper back. A little point shows more forward head position. It has been tracked down that more modest the CVA point is related with migraines in females51. Additionally change in arrangement of neck can deliver strain of cervical joints and delicate tissues just as imbalanced muscle execution. Head act immediately affects the situation of mandible and can prompt temporo-mandibular joint brokenness, and gulping difficulties14.
Ethical clearance: There was no risk of conducting this study.Ethical clearance was obtained from the ethical committee of Institute of Applied Medicine and Research, under the Chaudhary Charan Singh University, Meerut with approval letter dated 15thApril 2011.
Conflicts of Interest: There is no conflict of interest to conduct this study.
Fund for the study: This is self-funded study.
CONCLUSION
The consequence of the investigation upholds the exploratory theory that powerful stacking the understudy with 15% of body weight prompts huge change in cervical and shoulder pose when contrasted with static stacking with 15% of body weight and dumped condition, Significant change in cervical and shoulder showed by decline in craniovertebral point and expansion in sagittal shoulder act was found in unique stacking and static stacking when contrasted with dumped act.
We have likewise tracked down that 5 minutes of dynamic exercises with 15% of body weight produce huge change in craniovertebral and sagittal shoulder pose when contrasted with dumped act. Consequently, suggesting that school sack gauging 15% of body weight would be excessively weighty for the Indian school youngsters matured 17-20 to have the option to keep up with their ordinary cervical and shoulder pose arrangement.
REFERENCES
1. Knapik J, Harman E, Reynolds K. Load carriage using packs: a review of physiological, biomechanical and medical aspects. Applied ergonomics. 1996 Jun 1;27(3); 207-16.
2. Voll HJ, Klimt F. Strain in children caused by carrying school bags (author’s transl). Das Offentliche Gesundheitswesen. 1977 Jul 1;39(7); 369-78.
3. Oliveira R, Cabri JM. Low back pain in young people: cross-sectional study in Lisbon. In AIESEP 2005 World Congress-” Active lifestyles: the impact of education and sport”, 2006; pp.233-237.
4. Taimela S, Kujala UM, Salminen J J, Viljanen T. The prevalence of low back pain among children and adolescents: a nationwide, cohort-based questionnaire survey in Finland. Spine. 1997 May 15;22(10);1132-6.
5. Iyer SR. An ergonomic study of chronic musculoskeletal pain in collegechildren. The Indian Journal of Pediatrics. 2001 Oct;68(10); 937-41.
6. Negrini S, Carabalona R. Backpacks on! School children’s perceptions of load, associations with back pain and factors determining the load. Spine. 2002 Jan 15;27(2); 187-95.
7. Pascoe DD, Pascoe DE, Wang YT, Shim DM, Kim CK. Influence of carrying book bags on gait cycle and posture of youths. Ergonomics. 1997 Jun 1;40(6); 631-40.
8. Whittfield JK, Legg SJ, Hedderley DI. The weight and use of school bags in New Zealand secondary colleges. Ergonomics. 2001 Jul 1; 44(9); 819-24.
9.Chansirinukor W, Wilson D, Grimmer K, Dansie B. Effects of backpacks on students: measurement of cervical and shoulder posture. Australian Journal of physio-therapy. 2001 Jan 1;47(2); 110-6.
10. S.I. Weinsein, Garry M. Banks and Ensor E. Transfeldt. 1994. The Pediarics Spine: Principles and Practice. Raven Press. Ltd. New York.
11. Raine S, Twomey LT. Head and shoulder posture variations in 160 asymptomatic women and men. Archives of physical medicine and rehabilitation. 1997 Nov 1; 78(11);1215-23.
12. Watson DH, Trott PH. Cervical headache: an investigation of natural head posture and upper cervical flexor muscle performance. Cephalalgia. 1993 Aug; 13(4); 272-84.
13. Darling DW, Kraus S, Glasheen-Wray MB. Relationship of head posture and the rest position of the mandible. The Journal of prosthetic dentistry.1984Jul 1; 52(1); 111-5.
14. Shi Wei Mo 1, Dong-Qing Xu, Jing Xian Li, Meng Liu Effectof backpack load on the head cervical spine and shoulder postures in children during gait termination, 2013; 56(12); 1908-16.
Citation: Prachi Jain, Syeda Khanam P, Manjunatha H(2021).Efficacy of heavy bags with 15% of body weight in teenagers on cervical and shoulder posture allignment, ijmaes; 7 (3); 1049-1060.
Ishwarya vardhini. C1, Nelshiya Anni Ruby Aishwariya. H. P2
Author:
1Assistant professor,
Faculty of physiotherapy, Dr.MGR Educational and research institute University,
Velappanchavadi, Chennai, Tamilnadu, India
Corresponding Author:
2BPT Internee, Faculty of physiotherapy, Dr. MGR. Educational and research institute University, Velappanchavadi, Chennai, Tamilnadu, India, Email id: nelshiyaannirubyaishwariya@gmail.com
ABSTRACT
Background of the study: Osteoarthritis (OA) knee is a commonest degenerative disorder, accompanied by pain, muscle weakness, and decreased ability to carry out activities of daily living. Strengthening of VMO is the exercise choice commonly used. Studies suggest that strengthening of hip abductor; can reduce the KOA-associated symptoms. Objective of this study was to find whether VMO in combination with hip abductor strengthening can improve the function and reduce pain in KOA. Materials and methods: 30 subjects with grade 1- KOA of both the genders belonging to age group from 45-60 years were chosen and subjected to VMO & hip abductor strengthening for a period of 12 weeks. Pre and Post exercise outcome scores were measured using VAS and WOMAC scale. Results: This study showed a substantial improvement of pain, stiffness and physical function in subjects who underwent VMO and hip abductor strengthening program. P-value on VAS and WOMAC scale was less than 0.0001 which was found significant. Conclusion: Hip abductor along with VMO strengthening is a better health interventionin subjects with Grade 1 Osteoarthritis knee .Thus hip muscle strengthening can serve a better intervention in slowing the progression of disease and reduction of symptoms in grade -1 KOA.
Received on 28th January 2021, Revised on 18th February 2021, Accepted on 27th February 2021; DOI:10.36678/IJMAES.2021.V07I01.007
INTRODUCTION
Osteoarthritis of knee is the second most common chronic degenerative joint disease occurring among elderly. It leads to pain, muscle weakness especially quadriceps and disability which are the earliest clinical signs of OA knee1. OA knee is classified into 2 divisions. Primary OA knee is without any known reason (idiopathic) and ccurs in the elderly due to ageing process. Secondary OA knee is due to increased body mass index, family history, joint hyper mobility, repetitive strain to the knee, trauma, immobilization, neuropathic disorders 2.
The symptoms that halt the function include morning stiffness, reduced joint movement, crepitus and muscle atrophy 3. Diagnosis of knee osteoarthritis can be confirmed based on clinical and radiographical Findings .The American College of Rheumatology criteria , EULAR diagnostic criteria ,can be further used to diagnose KOA which includes presence of constant knee pain, morning stiffness reduce function, joint crepitus, restricted mobility and hypertrophy of bone. The available treatment options are non-pharmacological, pharmacological or surgery. Physical therapy is a least expensive intervention for OA knee which is recommended by the American college of Rheumatology and the European League against Rheumatism4.
Exercise is recommended as a first-line of conservative management option for osteoarthritis (OA). They can decrease pain status, improve joint mobility & functional ability. Quadriceps weakness is common among OA knee which in turn causes painful lower limb thereby making it a risk factor for development of OA. The function of quadriceps group of muscles, particularly VMO muscle has an important role in the stability of the patella-femoral joint 5. Reduction in activity of hip abductor muscle has been suggested as a contributing factor for the disease progression in knee osteoarthritis (OA).
Hip abductor strengthening can serve as an intervention to reduce knee joint loading in subjects with OA knee 6. Increased hip abduction moment magnitude is directly proportionate in reducing the progression of medial compartment OA knee7. Hip abductor weakness results in poor functional performance in subjects with OA. They are stabilizer of trunk & hip during walking, maintain the position of lower extremity and transmit the forces from the lower extremity to the pelvis8. Therefore inclusion of hip abductor exercises along with VMO can prove beneficial when designing a rehabilitation program for persons with knee OA.
METHODOLOGY
This was an
Experimental study and the participants those attending the outpatient
physiotherapy department in ACS medical college and hospital, Dr. MGR
Educational and Research institute, Chennai India. The study duration was around 12 weeks. This
study included 30 subjects with grade I Osteoarthritis knee (as per kellgrenn
and Lawrence radio graphical grade(9)
of both the genders in age-group between 45 and 60 years. The participants were
selected by simple random sampling
method. Subjects apart from grade 1 OA knee, non-cooperative
subjects, those with balance, auditory, visual disorder, lower limb injury were
excluded from the study.
The objective of this study was to find the effect of hip
abductor and vastus medialis oblique muscle (VMO)
strengthening exercises on Pain
and Physical function were measured using VAS (Visual analog scale) and WOMAC
(The Western Ontario and McMaster Universities Osteoarthritis Index).
Procedure: The
subject’s pain & functional ability were documented using Visual Analogue
Scale (VAS) in which the patient denotes pain level on the line between two
endpoints. The distance between point of no pain and the marking measures the subject’s pain score(10).
Then WOMAC (The Western Ontario and
McMaster Universities Osteoarthritis Index)
which
includes five questions about pain, two about stiffness and seventeen on degree of disability of activities performed every day11.
Following this, the subjects underwent hip abductor and vastus medialis oblique muscle (VMO)
strengthening exercises namely clam shell, lateral leg slides, abduction lifts,
terminal knee extension, single leg lifts, leg extension respectively for a
total of 3 sets consisting 12 repetitions each .The exercises were given for 4
days in a week for total of 12 weeks. Subjects were advised to continue
the medications as prescribed by their physician. After 12 weeks post exercise,
they were subjected to Post Vas, WOMAC and findings were documented.
RESULT
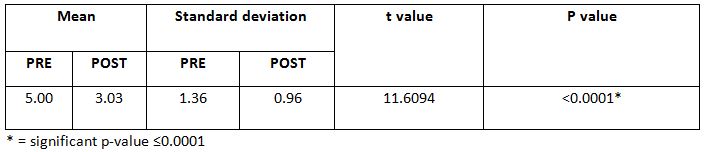
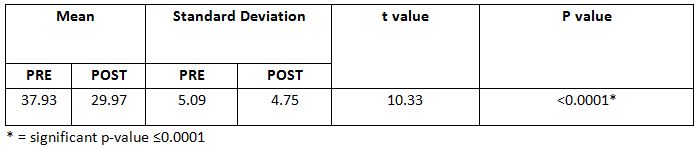
This study showed a substantial improvement of pain, stiffness and physical function in subjects who underwent VMO and hip abductor strengthening program. P-value on VAS and WOMAC scale was less than 0.0001 which was found significant.
Table 1: Mean pain score on VAS- (Pre and Post test) Table 2: Mean (pain sub score) on WOMAC – (Pre and Post test) Table 3: Mean (Stiffness sub score) on WOMAC – (Pre and Post test) Table 4: Mean (physical function sub score) on WOMAC – (Pre and Post test)
DISCUSSION
This study was aimed to find the impact of hip abductor
& VMO muscle strengthening in subjects with grade 1 osteoarthritis
knee. Pain and Physical function was
measured using VAS and WOMAC. The
outcome of the study was markedly improved, on the WOMAC score after twelve
weeks intervention program for the hip abductor and VMO in 30 participants.
In addition to the reduced dynamic loading at the knee,
each subject experienced a marked decrease in knee pain during the study. VMO
Strengthening served to reduce pain in subjects. The
hip abductor plays an important role as pelvic and trunk stabilizer in
locomotion 10.
The subjects
gave a feedback on reduced gait deviations and improved stability during
walking which is well evident from findings of Yujiexie, chi zhanget.al,
(2018) who reported that the
position of body center is depends on the strength of hip abductor weakness
which
can alter in
the contra lateral movement of the pelvis or lateral leaning of the trunk over
the weight bearing lower extremity 11.
Knee adduction
moment, associated with hip adduction has proved effect on reduce the disease
severity on OA Knee. Hip abductor appears to have certain impact on knee
joint load, which may also play a potential role in the symptoms, progression
of disease & studies have pointed that hip abductor strengthening
exercises may be helpful to improve the
physical function & alleviate pain in OA knee12.
A study on lower limb muscle strengthening also have reported effect on reduce pain and potential ability at knee joint which is inexpensive treatment for OA. The findings are evident for the effects of hip abductor and VMO strengthening on relieving pain and improving physical function in knee OA subjects. Hip abductor strengthening routine can be included in grade-1 stage of knee OA as it can reduce the progression of the disease and improve quality of life.
Ethical
Clearance: Ethical
clearance has obtained from Faculty of Physiotherapy, DR.MGR. Educational and
Research Institute, Chennai to conduct this study with reference number: A–026(A)/ PHSIO/IRB/2018-19dated 07/01/2019.
Conflict of interest: The author reported no conflict of interest to
do this study
Funding: The researchers had self financial support to conduct this research.
Limitation: A
small sample size, less study duration. Effect of medications was not taken
into consideration.
Recommendations of the study:
More outcome measure can be used. Several types of exercises can be compared
for future studies. This study can be compared with other grades of KOA.
CONCLUSION
We can conclude that hip abductor and VMO strengthening is
effective in reducing pain and improving physical function in subjects with
grade- 1 KOA. Hence it can be included during the initial phase of
rehabilitation of KOA.
REFERENCE
1. Hinman RS, Hunt MA, Creaby MW, Wrigley TV,
Mc Manus FJ BK. (2010). Hip muscle weakness in individuals with medial knee
osteoarthritis. Arthritis care Res. 62(8): 1190.
2.
Michael JW, Schlüter-Brust KU EP. (2010). The epidemiology, etiology, diagnosis, and
treatment of osteoarthritis of the knee. Dtsch Arzteblatt Int. 107(9): 152.
3.
Gorial F I, Sabah S A, Kadhim M B J N. (2018). Functional Status in Knee
Osteoarthritis and its Relation to Demographic and Clinical Features. Mediterr
J Rheumatol. ; 29 (4): 207.
4.
Zhang W, Doherty M, Peat G, Bierma-Zeinstra MA, Arden NK, Bresnihan B, (1962). Herrero-Beaumont
G, Kirschner S, Leeb BF, Lohmander LS MB. Eular evidence-based recommendations
for the diagnosis of knee osteoarthritis. Ann Rheum Dis. 69(3): 483.
5. Sled E A, Khoja L, Deluzio K J, Olney S J C E.
(2010). Effect of a home program of hip abductor exercises on knee joint
loading, strength, function, and pain in people with knee osteoarthritis: a
clinical trial. Phys Ther. 1 ; 90(6) :895-904.
7.
Rutherford DJ H-KC. (2009). Explaining
the hip adduction moment variability during gait: Implications for hip abductor
strengthening. Clin Biomech. 1; 24(3): 267-73.
8. Harikesavan
K, Chakravarty R D, Maiya A G, Hegde S P S S. (2017). Hip abductor
strengthening improves physical function following total knee replacement:
one-year follow-up of a randomized pilot study. Open Rheumatol Journal. 11:30.
9.
Kellgren J H L J. (1957). Radiological assessment of osteo-arthrosis. Ann Rheum
Dis.; 16(4): 494.
10.
Yang KA, Raijmakers N J, Verbout AJ, Dhert WJ SD. (2007). Validation of the
short-form WOMAC function scale for the evaluation of osteoarthritis of the
knee. J bone Jt surgery Br Vol. 89(1): 50-6.
11.
Xie Y, Zhang C, Jiang W, Huang J, Xu L, Pang G, Tang H, Chen R, Yu J, Guo S X F. (2018). Quadriceps combined with hip abductor
strengthening versus quadriceps strengthening in treating knee osteoarthritis:
a study protocol for a randomized controlled trial. BMC Musculoskelet Disord.
19(1): 1-7.
12.
Lim BW, Hinman RS, Wrigley TV, Sharma L BK. (2008). Does knee malalignment mediate
the effects of quadriceps strengthening on knee adduction moment, pain, and
function in medial knee osteoarthritis? A randomized controlled trial. Off J Am
Coll Rheumatol Care Res. 59(7): 943.
Citation: Ishwarya vardhini. C, Nelshiya Anni Ruby Aishwariya. H. P(2021). Efficacy of Vastus Medialis Oblique Muscle and Hip Abductor Strengthening on Pain and Functional Ability in Patients with Knee Osteoarthritis, ijmaes; 7 (1); 969-974.
2BPT Internee, Faculty of
physiotherapy, Dr. MGR. Educational and research institute University,
Velappanchavadi, Chennai, Tamilnadu, India
Corresponding Author:
1Assistant professor, Faculty of physiotherapy, Dr.MGR Educational and research institute University, Velappanchavadi, Chennai, Tamilnadu, India, Email id: divyamary.physio@drmgrdu.ac.in
ABSTRACT
Background of the study: Forward head posture is the anterior positioning of the “cervical spine”. This posture is sometimes called “text neck” or “reading neck”. Mostly the targeted group is younger & older adults. The main reason is our sedentary lifestyle-sitting at computers for hours, playing games continuously, driving for long distance time. Objective of the study is to find out the effectiveness of conventional exercise over fencing exercise to correct the forward head posture in individuals with abnormal head posture. Methodology: this study is the experimental design comparative pre & post type.30 subjects will be divided into two groups. Group a will be given conventional exercise & group b will receive fencing exercise. Ruler measurement & Cranio vertebral angle will be used as outcome measures. Result: on comparing pre test & post test within group a% group b on ruler measurement & cranio-vertebral angle shows highly significant difference in mean values p ≤ 0.001. Conclusion: This study shows that there was improvement in forward head posture in both groups. however conventional exercise(Group-A) showed more improvement than fencing exercise (Group-B) & to correct forward head posture & brings them back to normal posture. Keywords: Fencing exercise; Ruler measurement; Forward head posture; Cranio-vertebral angle.
Received on 29th January 2021, Revised on 14th February 2021, Accepted on 26th February 2021; DOI:10.36678/IJMAES.2021.V07I01.006
INTRODUCTION
Forward
head posture is one of the most commonly recognized types of poor head posture
in the sagittal plane. Forward head
posture has been defined as any alignment in which external auditory meatus is
positioned anterior to the plumb line through
the shoulder joint1, 2.
Mostly,
the targeted group is younger and older adults. Totally,100 peoples are
affected in the age group between 20-70 years old. The prevalence of anterior head translation in neck pain
patients was found to be 37%, out of
which 58% were female and 42% were male number. A review of different observational studies of neck pain around
the world showed that its 1-year prevalence ranged from 16.5 to 75.1% for the
entire adult population which aged from 17 to 70 years3, 4.
Data
show that the people affected by “Forward Head Posture” in their fifties
accounting for more than 23% of the total followed by those in their forties, thirties, and seniors over sixty. It
has become more prevalent in modern times as the COG shifts in the body posture. For, compensation the upper body
drifts backward and shoulder slump
forward by placing head anterior to the trunk5,6.
While
sitting, forward head inclination involves a combination of lower cervical
flexion, upper cervical extension, which reduces the average lengths of muscle
fibers, contributing to extensor
torque around the upper cervical joint. In addition to this, abnormal posture
causes musculoskeletal abnormalities such as decreased scapular upward
rotations well as greater internal rotation and anterior tilting, which may be
the difficulties in maintaining upright posture
.Conventional exercise aims at improving function of muscle, which counteracts
the forces of gravity in order to maintain the head and neck in upright position7-9.
Fencing
response designation arises from stimulating the “asymmetric tonic neck reflex”
in infants. like reflex, a positive fencing response resembles the en grade
position that initiates fencing with extension of one arm and flexion of other. This study aims at the
effectiveness of fencing exercise with conventional exercise in forward head
posture in individuals with abnormal head posture10.
Biomechanics: In
forward head posture, the head shifts anteriorly from the line of gravity, the
scapulae may rotate medially, a thoracic kyphosis may develop and overall
vertebral height may be shortened. The features are as follows: there is an
obliteration of the cervical lordosis and a compensatory tilting back of the
head at the atlanto-occipital joint. In the posterior cervical muscles there is
stretching and weakness of semispinalis cervicis and overaction with ultimate
shortening of semispinalis capitis 11.
Pathomechanics: Instabilities lead to more serious pathology
eventually, such as desiccation(thinning disc),cervical spine spondylosis, disc
pathology facet ¢ral cord stenosis, thoracic spine compression
fractures. People with uncorrected FHP
posture potentially suffer chronic or unpleasant conditions, such as pinched
nerves 12.
Upper Cross Syndrome– Tightness of the upper trapeziums and
elevator scapula on the dorsal side crosses with tightness of pectorals major
and minor. Weakness of the deep cervical flexors ventrally crosses with
weakness of middle and lower trapeziums’ his pattern of imbalance creates joint
dysfunction, particularly at the Atlanta occipital joint,C4-C5 segment,
cervico-thoracic joint, gleno-humeral joint&T4-T5 segment 13.
METHODOLOGY
This study is the experimental
design comparative pre & post type. 30 subjects were recruited from dr.mgr
educational & research institute (A.C.S medical college and hospital) –
physiotherapy – opd, Chennai. Subjects were selected by simple random sampling
method. Study duration was 5 days in a week for 4 weeks. Inclusion criteria were both male and
female subjects between age group 18-35 years old, who have 4-12cm in “ruler
measurement” & “cranio-vertebral angle” less than 50 degree. Exclusion
criteria were age group between below 18 & above 35 years were excluded.
Subjects with systemic illness, no recent injuries & neurological
complications were excluded. Ruler measurement & cranio-vertebral angle
will be used as outcome measures. Mobile application (on protractor), adhesive
skin markers, millimeter ruler were the materials used.
Procedure: 30 volunteers fulfilling the inclusion criteria were
included in this study. The forward
head posture is identified by measuring the spinal column alignment.
Measurement of Forward Head Posture Ruler
Measurement: This method is done with ruler (scale),ask the patient to lean
on the wall in relaxed position & measure the length between the wall and
head.
Cranio-vertebral Angle
This method was measured using
smartphone application-“ON PROTRACTOR”. This application allows to take picture
and draw angle by touching the screen at the reference points on the markers.
Two markers were Used: One placed on the tragus of the ear and second placed on
C7 vertebra were measured and photographs taken.
Position of patient: The
patient is made to stand against the wall. 30 Volunteers Were Divided Into 2
Groups,
Group A- In this group, 15 volunteers performed forward head posture
correction program ,the exercise were done 5 days in a week for 4 weeks,
which consists of 2 sets with 15 repetitions.
Chin tucks, Isometric neck exercise,
Shoulder retraction/ Protraction,
Shoulder shrugging/ Dropping, Then followed by posture correction techniques.
The patient should stand in front of the mirror and correct the abnormal
posture, Chin tucked position.
Shoulder retracted position. The
patient should correct their abnormal posture for every one hour.
Group B- In
this group, 15 volunteers performed fencing exercise, the exercise were done 5
days in week for 4 weeks, which consists of 2 sets with 15 repetitions. The patient is given a wand
to perform fencing movements. All the fencing movements are done under the
instruction and supervision of physiotherapist only.
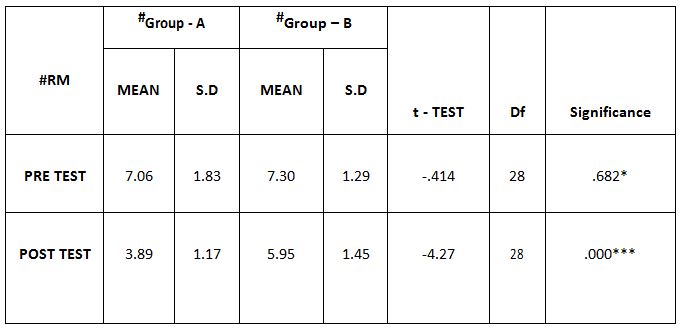
Table-1 Comparison Of Ruler Measurement Score Between Group – A And Group – B In Pre And Post Test
Group – B In Pre And Post Test
Table –2 Comparison Of Cranio-vertebral Angle Between Group – A And Group – B In Pre And Post Test
Comparison of Cranio-vertebral Angle Between Group – A And Group – B In Pre And Post Test
Table–3 Comparison of Ruler Measurement Score Within Group A & Group B Between Pre & Post Test Value
Comparison Of Ruler Measurement Score Within Group – A & Group – B Between Pre & Post Test Value
Table – 4 Comparison of Cranio-vertebral Angle Within Group – A & Group– B Between Pre & Post Test Values
RESULT
On comparing the pre and post
test values within the experimental group, Group A & Group B on Ruler
Measurement & Cranio-vertebral Angle shows highly significant difference in
Mean values where p value is P ≤ 0.001.Group A – Conventional Exerciseshows
statistically significant improvement then Group B – Fencing Exercise.
DISCUSSION
In this world, almost
everywhere including schools, colleges, offices and even in homes computers and Smartphone’s are commonly used today.
Forward head posture is the misalignment of head on trunk, leads to increased
lordotic curve of the cervical spine and accompanied by increased kyphosis of
thoracic spine. Forward head posture leads to body mechanical deformation
anterior to centerline of gravity, this reduces muscle strength of neck
stabilization muscles, reduces
the activity of the stabilizer
muscles of the scapulae and changes body mechanics of the scapulae. A sample of
30 subjects were selected and assessed then recorded the values. After, giving
treatment the values are analyzed for significant differences. Cranio-vertebral angle is a good indicator for
measuring forward head posture. The cranio-vertebral angle was measured using,
”On Protractor App” which is available
on goggle play store 13,14.
A study on validity and
reliability of “ON PROTRACTOR” smartphone application for measurement of cranio-vertebral
and cranio-horizontal angle. In this
study, the mean cranio-vertebral angle in non forward head posture is 50
degrees. The result of the study showed a effectiveness between conventional
exercise and fencing exercise. This
study proved that there was an increased effect in conventional exercise than
fencing exercise after correction forward head posture 15.
The conventional exercise
treatment showed improved ability in holding an upright posture of cervical
spine and retraining these muscles was shown to reduce the neck symptoms and
improved ability in maintaining an upright posture of cervical spine. The
result showed that forward head posture significantly, reduced in the treatment
groups after 4 weeks exercises, this improvement was also maintained after 1
month follow-up. Moreover, when compared with group A and group B, the forward
head posture was reduced in group A (conventional exercise), which is effective
16.
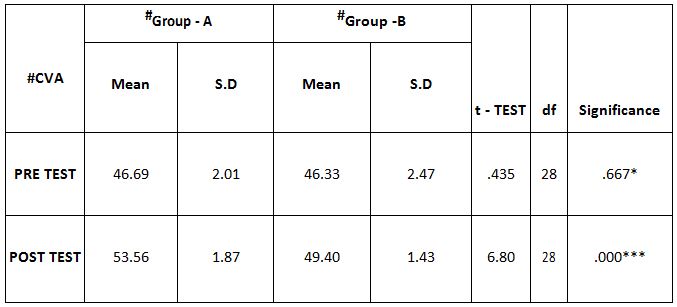
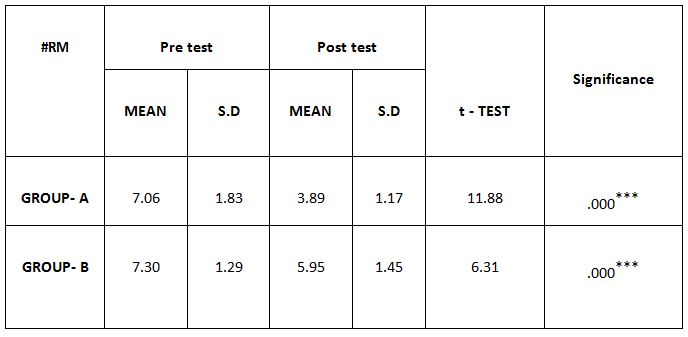
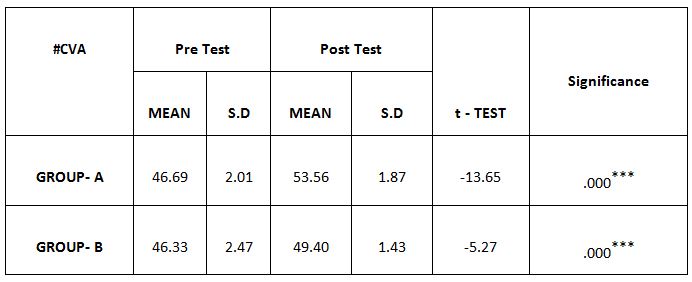
In this study 15 subjects were
included for conventional exercise (Group-A). It supported on effect in forward
head posture which reveals significant difference in mean values. In pre-test
7.09 in ruler measurement and 46.69 in cranio-vertebral angle. In post-test
3.89 in ruler measurement and 53.56 in cranio-vertebral angle. Another 15 subjects included in fencing
exercise (Group-B) .The fencing exercise also showed effect in forward head
posture correction. The study reported significant differences in mean values.
In pretest 7.30 in ruler measurement and 46.33 in cranio-vertebral angle. In
post-test 5.95 in ruler measurement and 49.40 in cranio-vertebral angle.
Fencing is a great cardiovascular
exercise, using several sets of muscles at a demanding intensity level over an
extended period of time. The physical benefits of fencing include increased
agility, balance, flexibility, Strength and cardiovascular endurance. While fencing is a whole exercise, it
exercises the arms, thighs, buttocks hardest of all .You also benefit from
fencing by gaining greater mental agility. Key muscles used for fencing
exercise are, Upper body-Back muscles and Trapezius, Lower body-quadriceps, hip
flexors, Gluteus, Hamstrings, Calves and core 17.
The purpose of this present study is to focus the effects of
conventional exercise and fencing exercise in correction of forward head
posture in younger adults. The conventional exercise is very effective because
it demands deep muscles to work and strengthen muscles. Conventional exercise
are very easy to learn and 15 subjects
were practiced at home without the supervision of physiotherapist.These,15
subjects set remainder in their
mobile phones to correct their posture and to do exercise regularly. They, also see mirror to
correct their head posture which act as visual feedback. Because, of active
participation of subjects in group A showed good and effective results.
In fencing exercise, especially
in upper body few sets of muscles are used like trapezius, back muscles, biceps,
triceps which is used for holding a wand and to keep shoulders in retracted
position. The 15 subjects in group also actively participated for fencing
exercise. To prevent unwanted consequences fencing exercise was done under the
supervision of physiotherapist. Fencing exercise also showed values nearing to
conventional exercise in 4 weeks duration. The pre-test and post-test of ruler
measurement and cranio-vertebral angle in experimental groups is statistically
significant at p<0.01 i.e. there is improvement in correction of forward
head posture after treatment.
Ethical
Clearance: Ethical
clearance has obtained from Faculty of Physiotherapy, DR.MGR. Educational and
Research Institute, Chennai to conduct this study with reference number: A-12/ PHSIO/IRB/2018-19dated 08/01/2019.
Conflict of interest: The
author reported no conflict of interest to do this study
Funding: The researchers
had self financial support to conduct this research.
CONCLUSION
By the obtained result from
this experimental study , it is concluded that there was improvement in forward
head posture in both groups. However, conventional exercise(Group-A) showed
more significant improvement than fencing exercise (Group-B) and corrects
forward head posture and brings them back to normal posture.
REFERENCES
Levangie P,Norkin C. (2012). Joint structure and function, 5th edition. New Delhi:Jaypee Brothers Medical publishers (P) Ltd; .P 502.
Jung Won Kwon, Phd, PT, et ai. (2015). Changes in upper-extremity muscle activities due to head position in subjects with a forward head posture and rounded shoulders. J Phys Ther Sci; 27(6): 1739-1742.
Gupta BD,Aggarwal S, Gupta B, Gupta M, Gupta N. (2013). Effect of Deep Cervical Flexor Training vs. Conventional Isometric Training on Forward Head Posture, Pain, Neck Disability Index In Dentists Suffering from Chronic Neck Pain. J Clin Diagn Res. 7(10):2261-4.
Deborah Falla, Gwendolen Jull, et al.(2007). Effect of neck exercise on sitting posture in patients with chronic neck pain.Physical therapy 87 (4), 408-417.
John S.Y. Chanaalan C.N. et al. (2011). Fencing expertise and physical fitness enhance action inhibition. Psychology of Sport and Exercise Volume 12, Issue 5, September Pages 509-514.
Johnson, Gillian M., Dip Phty, Msc Spine. (1998). The Correlation between Surface Measurement of Head and Neck Posture and the Anatomic Position of the Upper Cervical Vertebrae. April 15, – Volume 23 – Issue 8 – p 921-927.
Bhuvan Deep Gupta, Shagun Aggarwal, and Neha Gupta. (2013). Effect of Deep Cervical Flexor Training vs. Conventional Isometric Training on Forward Head Posture, Pain, Neck Disability Index In Dentists Suffering from Chronic Neck Pain. J Clin Diagn Res.; 7(10): 2261-2264.
Alireza Rabieezadeh, et al. (2016). The relationship of height, weight and body mass index with curvature of spine kyphosis and lordosis in 12-15 year old male adolescents of Tehran. Turkish Journal of Sport and Exercise.6Year: -Volume: 18 – Issue: 3 – Pages: 42-46 .
Kyeong-Jin Lee, et al.(2015).The effect of forward head posture on muscle activity during neck protraction and retraction. J. Phys. Ther. Sci. 27: 977-979.
Jae Woong Han (2016). Biomechanical Analysis of Chin Tuck Exercise with a Subject-Specific Neck Model for the Forward Headed International Journal Of Precision Engineering And Manufacturing Vol. 19, No. 4, pp. 587-592.
Jeong-Gon Na, et al. (2018). Effects of Exercise Type on Neck Disability, Pain, and Postural Changes in Subjects with Forward Head Posture: Systematic Review and Meta-Analysis. J Korean Soc Phys Med;13(3): 121-132.
Lindsay M. Bottoms, et al (2011). Physiological responses and energy expenditure to stimulated epee fencing in elite female fencers. Serbian Journal of Sports Sciences, 5(1): 17-20.
Jonathan D. Wiles, et al. (2018) The safety of isometric exercise Rethinking the exercise prescription paradigm for those with Stage 1 hypertension. Wiles et al. Medicine 97:10.
Minou Khakhali-Zavieh, et al. (2003) .The validity and reliability of measurement of thoracic kyphosis using flexible ruler in postural hyper kyphotic patients. Archives of Rehabilitation 4 (3), 18-23.
Jay Smith, Brian R Kotajarvi, Denny J Padgett, Joe J Eischen. (2002). Effect of scapular protraction and retraction on isometric shoulder elevation strength. Archives of physical medicine and rehabilitation 83 (3), 367-370.
Jerrold S Petrofsky, Richard L Burse, AR Lind. (1975). Comparison of physiological responses of women and men to isometric exercise. Journal of Applied Physiology 38 (5), 863-868.
Karthikeyan selvaganapathy, Roshini Rajappan, Thom hung dee. (2017). The effect of smartphone addiction on craniovertebral angle and depression status amount university students. International journal of integrative medical sciences, vol4(5): 537-42.
Citation: S. M. Divya Mary, S. Bhargavy(2021). Effect of movement therapy in individuals with abnormal head posture , ijmaes; 7 (1); 960-968.
1MPT Student, Faculty of physiotherapy, Dr. MGR. Educational and research institute University, Velappanchavadi, Chennai, Tamilnadu, India, Email id: vijayalakshmi260497@gmail.com
Author:
2Associate professor, Faculty of physiotherapy, Dr.MGR Educational and research institute University, Velappanchavadi, Chennai, Tamilnadu, India
ABSTRACT
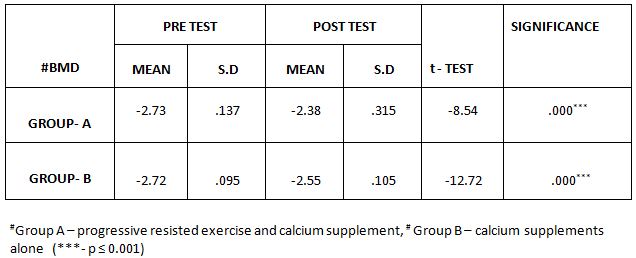
Background of the study: Osteoporosis is reduced density of bone due to vitamin D deficiency, which can be prone for bone fracture. Bone mineral density (BMD) has to be checked routinely to screen out its deficiency. Osteoporotic fractures in India occur commonly in both sexes, and many occur at a younger age. Objectives of the study are to find the status of BMD among women using calcaneal ultrasound bone densitometer (QUS) and the effect of progressive resisted exercises (PRE) on BMD. Methodology: It is an Experimental study, the study was conducted among women, of ‘’Bone Mineral Density Free Camp’’ organized at the ACS Medical College and hospital, Chennai. A total of 270 subjects (women) were screened by using Calcaneal Ultrasound Heel bone densitometer (QUS), out of which 66 subjects were detected with Osteoporosis. They were randomly assigned into Group A (Calcium supplements +Progressive Resistance Exercises) and Group B (Calcium supplements) by Randomized Control Trial (RCT) method. The duration of this study was three months. Results: The study has reported there is a significant difference after post test t-score measurements between group A and group B. The mean of Group A was higher than that of Group B. Conclusion: This study has recommended doing resistance exercises to prevent growing Osteoporosis among women. Calcaneal Ultrasound measurement could be a useful tool to asses BMD.
Keywords: Osteoporosis, Bone mineral density, Progressive resisted exercises, Calcaneal Quantitative Ultrasound Densitometer.
Received on 22nd January 2021, Revised on 7th February 2021, Accepted on 26th February 2021; DOI:10.36678/IJMAES.2021.V07I01.005
INTRODUCTION
Osteoporosis is a foremost cause
of bone related health issues, which can lead to skeletal abnormalities
including morbidity and socio economic troubles1. By 5th
decades of life it is reported as most women are affected with osteoporosis.
Early detection and treatment with adequate supplement is important to avoid
complication of low bone mineral density 2,
3.
Currently the most widely used
tool is Dual energy X-ray absorptiometry, which can measure density of skeleton
both appendicular and axial, but portable ultrasound is most cost effective. It
can measure the bone density more accurately with more cost effective and
radiation free screening test 4, 5.
Quantitative Ultrasound (QUS) is
the commonest device used to measure bone density. Bone density measurement
sites include vertebra, hip, forearm and calcanium. QUS can rule out osteopenia
of bone at any age of population6,7.
Lack of exercises has been found to significantly associate with lower
BMD in Indian women. Hormonal therapy is assumed to be helpful to prevent loss
of bone density, which can leads to osteoporosis. Different exercise program
has proved effect on bone absorption and prevent osteopenia. Best exercise
program to prevent osteoporosis need to be developed. Adequate levels of
estrogen, calcium intake, and vitamin D are essential along with exercise
program to get best effect on prevention of osteoporosis8, 9, 10.
Objectives of the study were to find out
the status of BMD among women using calcaneal ultrasound bone densitometer
(QUS) and to find the effect of progressive resisted exercises (PRE) on the
level of BMD.
METHODOLOGY
This is a
comparative experimental study conducted by a camp based approach to screen out
bone mineral deficiency. Free health check-up camps were organized in ACS
Medical College and hospital, Velappanchavadi, Chennai. Total 66 patients were
participated in this study. The
study was conducted for 3 months. Each week consist of 2 sessions per week.
Inclusion Criteriaof the study were female
subjects with age of above 35 years, subjects with osteoporosis.Exclusion Criteria were Systemic
disease like renal disease and hepatic disorders, Rheumatoid arthritis,
Endocrine disorders, Chronic medications of steroid and hormonal drugs,
Impaired skin sensation, Any malignancy / infections, Metal implants, Poor
hysterectomy and Known osteoporosis under treatment.
Materials used were treatment couch, towel, Chair, Stop watch, Sand
bags and Assessment sheet. Outcome measured was bone mineral density by
Quantitative Calcaneal Ultrasound (QUS) Bone densitometer.
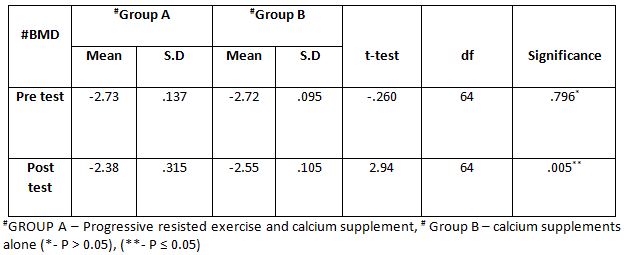
Method: Based on the
selection criteria 66 patients were randomly selected. Group A(n=33)
Progressive Resisted Exercises for 30-45mins per session of twice per week for
3 months and Calcium Citrate supplements twice a day (800mg). Group B (n=33)
Calcium Citrate supplements twice a day alone (800 mg).
Procedure: The subjects
were selected based on inclusion and exclusion criteria. All the patients
underwent pre-test assessment for Calcaneal Ultrasound on BMD. They were
randomly assigned into two groups (Group A Progressive resisted exercises and
calcium supplements) & (Group B calcium supplements only ). Written
informed consent was taken.
Menstrual history, systemic illness, height and weight were checked
before measure the bone mineral density. BMD was measured in Calcaneus (heel
bone) ultrasound bone densitometer. QUS device used to measure BMD values in
term of specific T-score criteria.
T-score of −1.0 or higher considered as normal and Osteopenia is defined
when the score is between 1.0 and 2.5, Osteoporosis is defined as 2.5 or more.
Group-A
Exercises interventions: Progressive resisted exercises and calcium supplements: Exercise protocol (Lora M, Giangregorio et al): Week-1 (elimination of gravity), Hip Extension 3X8 at 10 % , Knee Extension 3×8 at 10 %, Back Extension 3×8 at
10%, 1RM, Abdominal Flexion 3×8
at 10%, all exercise at 1RM, for week-
2 to 6 weeks 2 sets of 8-10 Repetitions At 1RM (against
gravity).
Sit to stand or Squat, Wall Squat Combine with Lateral Pull, Squats to
touch chairs- arms folded, Squat without touching chair, Standing Hip,
extension and abduction 10 repetitions, progress to abduction. Perform these
exercises and add resistance progress by sand bag. Lunge 1 walking lunge; alternating legs,
week-8 to 12 weeks (resistance against gravity), and the progression will be 15
repetitions at 60 to 80 % of 1RM.
Data analysis: The data were collected and analysed using both descriptive and inferential statistics .
Table -1 Comparison of bone mass density (BMD) test between group -A and group -B in pre and post test
This table shows that there is no significant difference in pre-test values of the BMD between Group A & Group B and statistically significant difference in post-test values of the BMD between Group A & Group B
Table 2: Comparison of bone mass density (BMD) test values within Group-A & Group-B between pre & post test values
Based on the BMD values,
it shows that there is a statistically significant difference between the pre-
test and post -test values within Group-A and Group-B.
RESULTS
On comparing the mean values of Group A & Group B on Bone Mass
Density (BMD) test values, it shows significant increase in the post test mean
values but (Group A- Progressive
Resistance exercises and Calcium supplement) shows (-2.38) which has the
higher mean value is effective than (Group B-Calcium Supplement alone) (-2.55) at P ≤ 0.05.Hence Null Hypothesis is rejected.
On comparing Pretest and Posttest within Group A &
Group B on Bone Mass Density (BMD) Test Values
shows significant difference in Mean values at P ≤ 0.001
DISCUSSION
This present study was based on camp conducted in ACS medical college
and hospital, Chennai. The aim of the study was to evaluate
bone mineral density. The study reported the role of progressive
resistance exercises in association with BMD. Women of 5th decade
found more vulnerable for osteoporosis and bone fracture, so need to take more
measures to prevent disability.
Osteoporotic changes are common among aged women than men. This has
been reported as the mineral bone density is decrease with increase of age.
Above 50 year are shown more prone for osteoporosis over 36.4% of women
population. Fewer symptoms in early stage make the people to be less aware
about low bone mineral density. Later stage with bone fracture leads the
patients to measure bone density, by the time they would have developed
osteoporosis. As BMD screening is not done routinely turns up the patients with
fractures 11, 12.
Boneosteoblastic activity suppresses in both elderly male
and female, it is common in women with aging.
Estrogen withdrawal in aged people suppresses osteoblastic activity and
enhances osteoclastic activity. Low BMD
increases with age in both the sexes, so prevention of deficiency in BMD is
essential to avoid complications. Timely intervention with proper nutrition and
exercise can improve bone density and can prevent the progression of the
condition 13, 14, 15.
In addition Progressive resistance exercises are found to be more
effective in recent researches. Hence, for the women to be normal, she must be
enrolled in effective exercises, adequate calcium intake along with their
routine physical activities, despite the availability of gym with efficient
friendly atmosphere for women is rarely found in India. To overcome these
difficulties and to enroll women in exercise session and to educate them, home
based Progressive resistance exercise protocols are intervened 16,
17, 18.
Ethical Clearance: Ethical
clearance has obtained from Faculty of Physiotherapy, DR.MGR. Educational and
Research Institute, Chennai to conduct this study with reference number: IV B–051/ PHSIO/IRB/2017-18dated 08/01/2018.
Conflict of interest: The author reported no conflict of interest to
conduct and publish this article.
Funding:The researchers had self financial support to conduct this research.
CONCLUSION
The present study demonstrates that there is positive significant
relation between Bone Mineral Density and Progressive Resistance Exercises
among women. Hence, Progressive Resistance Exercises is an important
determinate factor of Bone Mineral Density among women. Thus, more sensitive
methods are recommended at this stage for formulating policy regarding
preventive interventions. Through this study, we concluded that risk of
Osteoporosis among women should be targeted for Resistance exercises to prevent
growing increase of the condition and its complications.
REFERENCES
Aggarwal N, etal. (2011). Prevalence and related
risk factors of osteoporosis in peri and postmenopausal Indian women. J Midlife
Health 2: 81-5.
Syed Z, Khan A. (2002). Bone densitometry: Application
and limitation. J obstet Gynaecol Can 24:476-84
Cumming SR, et al. (1995). Risk factors for hip
fracture in white women. Study of Osteoporotic Fractures Research Group. N Engl
J Med.; 332(12):767-73.
Sharma S, Tandon VR, Mahajan A, Kour A, Kumar D.
(2006). Preliminary screening of osteoporosis and osteopenia in urban women
from Jammu using calcaneal QUS. Indian J Med Sci; 60:183-9.
Shatrugna V, Kulkarni B, Kumar PA, Rani KU,
Balakrishna N. (2005). Bone status of Indian women from a lowincome group and
its relationship to the nutritional status. Osteoporos Int.; 16(12):1827-35.
Kataria SK, Pareek P, Dadhich A, Kataria KR,
Bhati M. (2012). The effect of body mass index on bone mineral density in pre
and postmenopausal women of western Rajasthan population. Int J Biol Med Res.
3(3):1899-1901.
Anburanjan M, Kumar D A, Sapthagirivasan V. (2011). Evaluation of
osteoporosis in Indian women and men usingp DXA. Academia.ed. International
conference on bioscience, biochemistry & bioinformatics (ICBBB- 2011),
ISBN: 978-1-4244-9388-3 pp 470-474,.
Shukla J, Sarkar PD, Bafna A, Shukla N. (2013).
A retrospective study to investigate association among age, BMI and BMD in
postmenopausal women. IOSR-Journal of pharmacy and biological sciences,
6(2):93-6.
Widmaier EP, Raff H, Strang KT. (2011). Vander’s
human physiology the mechanisms of body function. 12th edn. New York:
McGraw-Hill; p. 345-48.
Navarro MC, Sosa M, et al.
(2009). Poverty is a risk factor for osteoporotic fractures. Osteoporos Int.
Mar; 20(3): 393-8.
Paul TV, Thomas N, et al.
(2008). Prevalence of osteoporosis in ambulatory postmenopausal women from
semi-urban region in south India: relationship to calcium nutrition and vitamin
D status. Endocr Pract., 14(6):665-71.
Baheirai A, Pocock NA, et
al. (2005). Bone mineral density, body mass index and cigarette smoking among
Iranian women: implications for prevention. BMC Musculoskelet Disord. 6:34.
Salamat MR, Salamat AH,
Abedi I, Janghorbani M. (2013). Relationship between weight, body mass index
and bone mineral density in men referred for dual-energy X-ray absorptiometry
scan in Isfahan, Iran. J Osteoporosis 2013:205963.
Citation: Vijayalakshmi B, Padmanabhan K(2021). Effectiveness of progressive resisted exercises among women on bone mineral density , ijmaes; 7 (1); 954-959.
Syeda
Khanam. P1, Manjunatha. H2, Thummala S. Pavani3
Corresponding Author:
1Professor, East
College of Physiotherapy, Bidrahalli, Bangalore, Karnataka, India
Co Authors:
2Principal, East College of Physiotherapy, Bidrahalli, Bangalore, Karnataka, India3Assistant Professor, East College of Physiotherapy, Bidrahalli, Bangalore, Karnataka, India
ABSTRACT
Background and purpose: This study was to find the effect of inspiratory muscle training on dyspnoea and exercise tolerance among chronic obstructive pulmonary disease patients.
Methods: It is a randomized control study of 30 COPD participants with 15 in each control and experimental group. Experimental group underwent inspiratory muscle training with threshold IMT device in the physiotherapy department, where subjects have to breathe against various threshold levels, 30sets/sessions where as control group underwent only breathing and general mobility exercises at home. The training lasted for 20-30 minutes, twice daily 6days per week, and was continued over the course of 4 weeks duration. Parameters included were 6minutes walk test, MRC dyspnoea grade, PEFR values. The data collected data of control and experimental group was compared to find the outcome.
Results: Before interventions, all patients showed increased dyspnoea levels and reduced exercise tolerance. After interventions they all exhibited reduced dyspnea and increased exercise tolerance based on 6min walk test, MRC dyspnoea grade, PERF Parameters. Control group patients didn’t exhibit any improvement in any of the parameters.
Conclusion: The results support that inspiratory muscle training is more effective on reducing dyspnoea and increasing exercise tolerance among COPD patients.
Keywords: Chronic Obstructive Pulmonary; Dyspnoea; Exercise tolerance; Inspiratory muscle training
Received on 20th January 2021, Revised on 4th February 2021, Accepted on 24th February 2021; DOI:10.36678/IJMAES.2021.V07I01.003
INTRODUCTION
Chronic obstructive pulmonary
disease is a condition characterized by narrowing of airway tract with symptoms
of chronic cough, expectoration, wheeze and exertion dyspnoea. COPD can develop
and progress by 25% risk factors of smoking and to mortality by 15% with
addiction of smoking 1-3.
Diaphragm is the main inspiratory
muscle morphologically and functionally responds to the inspiratory muscle
training. There are evidence documented in possibility of resultant
accumulation of co2 takes place even after resolution of acute
exacerbation of conditions and relative obstruction of airway 4, 5.
The IMT device can help to do
inspiratory training exercise which can increase strength of inspiratory
muscle; there by it can improve the threshold of inspiratory resistance.
Overall health related quality of life (HRQL) can improve by repeated
inspiratory muscle training. The exercise training decrease dyspnoea and work
of breathing becomes easier in patients with COPD. Regular inspiratory training
can facilitate to perform physical activities more easily 6-10.
Aims and objectives of the study
was to find the effect of inspiratory muscle strength and endurance to increase
exercise tolerance, decrease work of breathing, and to improve functional
exercise capacity and also to increase overall health related quality of life.
METHODOLOGY
The study Design was Randomized control study. Data collected were from the patients recruited from pulmonology OPD and treated in the physiotherapy department, Nizam’s institute of medical sciences, punjagutta Hyderabad. Patients were assessed thoroughly and treated during the trails. Period of study intervention was 4 weeks and materials used were threshold inspiratory muscle trainer.
Figure 1: Peak Expiratory Flow Meter
Peak expiratory flow meter is
used to record the peak expiratory air flow rate of a person. The forced
expiratory volume of a person is measured using this device. The forced
expiratory volume of a person is measured using this device. The forced
expiratory volume is given in liters’/minute. In COPD patients the PEFR is
altered due to biomechanics of chest.
GAIAMS*Power breathe provides a
threshold resistance during inspiratory phase. It helps in increasing strength
and endurance of respiratory muscles, reduce severity of dyspnoea and improves
exercise capacity patients with COPD, asthma, cystic fibrosis, chronic heart failure,chronic spinal
injury, muscular dystrophy, before cardio thoracic surgery.Materials
required for the study was Sphygmomanometer, Stop watch, and Measure tape 11-14.
It has got 9 levels and load varies from level 1 to level 9, approximately as follows: Load (-cm H2O).
Table 1: 9 levels and load
Intensity: 10% to 52% of maximal
inspiratory pressure (PI Max).most commonly used training device in these
studies is threshold IMT. Frequency of the study duration was 7days/week and
total duration of the study was 4 weeks, 20-30 min session, twice a day.
Procedure: Subject has to sit in a high sitting position on a couch, hold the apparatus close to the mouth and take deep breathe against the resistance set with in the threshold IMT apparatus and blow air out relax. Patient has to repeat the same for 30 times. This procedure should be done twice a day, 30 minute every session. Patient is instructed properly and to discontinue usage if they have symptoms of breathlessness and cough.
Figure 2: Patient performing inspiratory muscle training
Inclusive criteria for this study
was Mild and moderate exacerbation of COPD
Exclusive criteria for this study was Severe exacerbation of COPD,
Pulmonary tuberculosis, Restrictive lung disease, Severe asthma, neuro muscular
disorders, musculo skeletal problems of spine, Heart failure/unstable angina
and Peripheral vascular diseases.
The data collected ranged from
parameters: 6 min walk test, Peak expiratory flow rate, and MRC dyspnoea
grading.
During study period 60 patients
were examined who were all COPDS associated with other problems but only 30 met
the inclusive criteria.15 patients were assigned for group A and remaining 15
for group B according to randomized control study. Their mean ages (group A
58.13; group B 52.06) were calculated.
Data analysis and results: All
data analysis was computed with statistics, paired T-test .within groups, student
T-test between groups and mean values were used for both groups to determine
the difference between outcome measures of 6 min walk test, MRC dyspnoea and
PEFR. Level of significance was fixed as 5 % for the present study.
Out of large proportion COPD with
mild and moderate exacerbation the sample taken for the study is 30,based on
convenience sampling method after thorough examination based on inclusive
criteria from the department of physiotherapy.30 participants were present for
the whole duration of the study 4 (week).
During 4 week of study course the
parameters studied were 6 min walk test, MRC dyspnoea scale, Peak expiratory
flow rate.
The data was collected on subject
on 1st week and 4th week, and raw data was arranged in
order to maintain the master chart, which was subjected to further statistical
analysis.
To find out of the average line
score in above mentioned parameters in each subject the means were calculated
at 1st week and these values were considered as base line values for
the study simultaneously the same parameters are studied at 4th week
and average variations were recorded in terms of means of each parameters and
the variations from the mean were also calculated.
The difference in each parameter
from 1-4 weeks was tested with paired T-test, within group and student T-test
between groups, finally the observed variations in each parameter was
represented in graphical format for easy understanding.
RESULTS
From 1st week to 4th
week all the parameters collected from the data are arranged in master chart
for further statistical analysis .The difference in each parameter from 1st
week(initial )to the end of 4th week(final),of the subject is shown
in the following tables.
6 Min Walk Test: The performance of 6min walk test was
conducted for both the groups (Experimental and control group) that to in
particular time schedule (1st week to 4th week). 1st
week taken as base period which is compared with other time factors,
combination allay. Different variables were studied between: 1st
week-4th week. For with group paired T-test was performed and among
two different groups student T-test was used; same tests are used for other
parameters MRC dyspnea, PEFR too.
Within Control Group: Among all the variables within the control group, paired T-test calculated value for 1st -4th week is 1.00000 and the table value is 2.145 at 5%level of significance with 14 degrees of freedom.
Table 2: 6min walk test within control Group Table 3: 6min walk test within Experimental Group
Within Experimental Group: Among all the variables within the experimental group, paired T –test calculated value for 1st week -4thweeks is 14.58441 and the table value is 2.145 at 5% level of significance improvement in 6minute walk in experimental group to control
Table 4: 6min walk test between control and Experimental Group
Between Control Group and Experimental Group: Between control and
experimental group student T-test was performed. Among all the variables the
student T- test calculated values for 1st and 4th week
(2.24).
The tabulated value at 5% level of significance with 28 degree of freedom is 2.049 showing the significant difference.
Table 5: MRC Grading of Dyspnea within Control Group
MRC Grading of Dyspnea within Control Group: Among all the variables with in control group, paired T-test calculated value for 1st week-4th week is less than 1.000 and the Table value is 2.145 at 5%level of significance with 14 degrees of freedom.
Table 6: MRC Grading of Dyspnea within experimental Group
MRC Grading of Dyspnea within Experimental Group: Among all the
variables within the experimental group, paired T –test calculated value for 1st
week -4th weeks is 5.69 and the
table value is 2.15 at 5% level of significance improvement in dyspnoea levels in experimental group to control
Table 7: MRC Grading of Dyspnea between Control Group and experimental Group
MRC Grading of
Dyspnea between Control Group and Experimental Group: Between control and
experimental group student T-test was performed. Among all the variables the
student T- test calculated values between1st and 4th week (6.25).The tabulated value at 5% level of significance with 28 degree of freedom is 2.05 showing the significant difference.
Table 8: Peak expiratory flow rate within control Group
Peak expiratory flow rate within Control Group:Among all the variables within the control group, paired T-test calculated value for
1st -4th week is 1.46759 and the table value is 2.145 at 5%level of significance with 14 degrees of freedom.
Table 9: Peak expiratory flow rate within Experimental Group
Peak expiratory flow rate within
Experimental Group: Among all the variables within the experimental group,
paired T –test calculated value for 1st week -4th weeks
is 9.57556 and the
table value is 2.145 at 5% level of significance with 14 degrees of freedom showing significant improvement in PEFR values in experimental group compared to control
Table 10: Peak expiratory flow rate between control and Experimental Group
Between Control Group and
Experimental Group: Between control and experimental group student T-test
was performed. Among all the variables the student T- test calculated values
for 1st and 4th week (4.09).The tabulated value at 5%
level of significance with 28 degree of freedom is 2.05 showing the significant
difference.
DISCUSSION
COPD is progressive and
irreversible disorder of airway. Therefore even after resolution of acute
exacerbation of condition there may be relative obstruction of airway. So
complete expiration is not possible after resultant accumulation of Co2.
Therefore, these patients frequently report dyspnoea related to activities of
daily living, such patients are considered as stable COPD patients. The symptom
induced inactivity leading to deconditioning and muscle weakness & thus
resulting into crucial impact of functional and health status15-17.
The present study has done on patients
with mild and moderate COPD for 4 weeks showed significant effects of IMT on
dyspnoea &exercise tolerance. Many
studies have reported the effect of inspiratory muscle training on dyspnoea and
exercise tolerance among COPD Patients. Parameters included in this study are 6
minute walk distance test, PEFR, and MRC grading of dyspnoea.
In experimental group in present
study the mean improvement in 6 minute walk distance at the end of 4 weeks of
training is 109.4 m, T cal values 14.584, T tab value 2.145,
showing significant improvement. In control group the mean difference in 6 min
walk is 3.2 m at the end of 4th week T cal values 1.000,
T tab value 2.145, showing no significant improvement. The limiting
factors for reduced exercise tolerance in patients with COPD are dyspnoea. The
increase in 6 min walk distance could be because of reduction in dyspnoea,
increased exercise tolerance.
PEFR mean difference within the
experimental group is78.66 T cal values at the end of 4th
week is 9.576 and the, T tab value 2.145, showing significant
improvement compared to control group where the mean difference is 1.33, T cal
values 1.468, T tab value 2.145. MRC grading of dyspnoea within
experimental group at end of 4th week the mean difference is 1.33, T
cal values 5.69, T tab value 2.15, showing significant
changes in dyspnoea levels in experimental group compared to control where
there is no significant changes in mean values, at the end of 4th
week T cal values is less than 1.000, and T tab value is
2.145.
A study on specific inspiratory
and specific expiratory muscle training has proved both are effective on
improving respiratory function, specifically it could reduce dyspnoea and
improve exercise performance. There was no difference in effect on the outcomes
when the patient performed combined specific inspiratory and expiratory muscle
training exercise program among COPD Patients 18-20.
The effect of specific expiratory
muscle training for one year among COPD patients have shown, it improves in
respiratory muscle strength and health related quality of life. The study has also reported maximal
inspiratory pressure and improves 6 minute walk distance and a decrease in the
mean Borg score during breathing against resistance scores. Some studies have
reported inspiratory muscle training has improved functional exercise capacity
and strength of respiratory muscles 21, 22.
Present study even showed
significant improvement in dyspnoea, exercise tolerance in COPD who underwent
IMT for 4 weeks. Most commonly used training device in these studies is
threshold IMT where intensity varied from 10% to 52% (high) of maximal
inspiratory pressure (PI max) 20-30 min session, twice a day.
The reduction in dyspnoea due to
IMT could be due to increased inspiratory muscle strength as determined 20%
Larson et al. study (1999), 34% Lisboa et al(1997), 25%weiner et al (2000),50%,
Sachez Riera et al (2016).
Inspiratory muscle training for
five weeks has proved effect on external intercostals muscles with strong
evidence of biopsy report on increase in size of type 2muscle fibers among COPD
patients.
A study among COPD patients in
Spain, they have analyzed health related quality of life (HRQL) using
Questionnaire after inspiratory muscle training and found effect on outcomes of
sustained maximal inspiratory pressures, shuttle walk test, in experimental
group.
Comparatively the present study
even showed significant changes and improvement in dyspnoea and exercise
tolerance on mild and moderate COPD patients where the duration of the study
was for 4 weeks and the outcome measures used were 6 min walk test, MRC
dyspnoea grade and PEFR values. Experimental group showed significant
improvement in all these outcome measures than the control group.
In a study conducted at south
Korea, the effects of inspiratory muscle training has reported the changes in
outcome measures of FEV1, level of dyspnoea based on Borgs score, and 6 min
walk distance, they were analyzed in experimental group and showed decreased
perception of dyspnoea and improved exercise capacity among moderate to severe
obstructive components in the presentation of COPD.
Comparatively in the present
study subjects were only mild, moderate COPD patients where control group did
not participate in IMT for 4 weeks but practiced general mobility exercises and
breathing exercises where as experimental group who underwent inspiratory
muscle training showed significant improvement in dyspnoea and exercise
tolerance.
The meta-analysis has reported
the effect of inspiratory muscle training on inspiratory muscle strength and
endurance, improved functional exercise capacity and decreased dyspnoea in
patients with COPD. The documented effects of inspiratory muscle training were
examined in a meta-analysis. The study is also recommended inspiratory muscle training
is a very essential addition to pulmonary rehabilitation programs.
In the present study done on
patients with mild and moderate COPD for 4 weeks the experimental group showed
significant effects of IMT on dyspnoea &exercise tolerance than control
group who underwent only breathing and general mobility exercises.
The studies conducted were
performed on a limited number of subjects. Further study is required on a large
group to quantitatively analyze the results of IMT on large scale.
Ethical Clearance: Ethical clearance
has obtained from Faculty of Physiotherapy, Nizam’s Institute of Medical
Sciences, Punjagutta, Hyderabad on 02/05/2008 to conduct this study.
Conflict of interest: There was no
conflict of interest to conduct this study.
Fund for the study: It was aself financed study.
CONCLUSION
The study has concluded from the
study that inspiratory muscle training can reduce dyspnoea and improved
exercise tolerance in COPD patients with mild and moderate exacerbation. The
study has also supported the exercise program can improve overall health
related quality of life (HRQL) among COPD patients.
Limitations: Limitations of the study were small sample size, short
time training period, IMT apparatus is not accessible and it is cost effective
for the patients and study was limited to a specific group of mild and moderate
COPD.
Future Direction: The present study can be extended for long term
rehabilitation. Future study can imply IMT on severe exacerbation of
COPD/chronic asthma, cystic fibrosis, pre op lung conditions such as lobectomy,
pneumonectomy. Pre and post training PI Max value of IMT can be taken to
further strengthen the study, and also can imply expiratory muscle training.
REFERENCES
Nice, L (2000). Mechanism and measures of
exercise intolerance in chronic obstructive lung disease.Clin Chest Med 21,
693-704.
Van’tHul, HA, Gosselink, R, Kwakkel, G (2003). Constant-load
cycle endurance performance; Test-Retest reliability and validity in patients
with COPD. J Cardio-pulmo rehabil. 143-150.
Polkey, MI, Moxham, J, (2004). Improvement in
volitional tests of muscle function alone may not be adequate evidence that
inspiratory muscle training is effective Eur Respir. J, 23, 5-6.
Holm, P, Sattler, A, Fregosi, RF (2004).
Endurance training of respiratory muscle improves cycling performance in fit
young cyclists.BMC Physio., 4: 9.
Weiner, P, Magadle,R, Beckerman, M, et al
(2003). Specific expiratory muscle training in COPD. Chest 124, 468-473.
Weiner, P, Magadle, R, Beckerman, M, et al
(2003). Comparison of specific expiratory, inspiratory and combined muscle
training program in COPD Chest 124, 1357-1367.
Bourjeily, G, Rochester, C L, (2000). Exercise
training in chronic obstructive pulmonary disease, Clinical chest med,
21,763-781.
Caine MP and MC Connell AK (2000). Development
and evaluation of a pressure threshold inspiratory muscle trainer for use in
the context of sports performance. Sports Engin 3,149-159.
Covey MK, Larson JL, Wirtz SE, Berry JK, Pogue
NJ, Alex CG and Patel M., (2001). High intensity inspiratory muscle training in
patients with chronic, obstructive pulmonary disease and severely reduced
function. J. Cardiopul. Rehabil. 21; 231-240.
Lotters, F, Kwarkkel, G, Gosselink, R. (2002).
Effect on controlled inspiratory muscle training in patients with COPD.A
Meta-analysis. European Respiratory Journal, 20,570-577.
Oh, Eui-Geum. (2003).The Effect of home-Based
pulmonary Rehabilitation in patients with chronic lung disease. International
journal of nursing studies, 40, 873-880.
Beckerman, Marinella, Magadle, R, (2005,
November). The effect of one year of specific inspiratory muscle training in
patients with COPD. Chest, 5, 3177-3183.
Martin, Daniel, (2002). Use of inspiratory
muscle strength training to facilitate ventilator weaning. Chest 122,192-196.
Sanchez, RH, Monte mayor, RT, Ortega, RF, et al.
(2001). Inspiratory muscle training in patients, with COPD; Effect on dyspnoea,
exercise performance, and quality of life chest 120,748-756.
De Jong W, Van Aalderen WM, Koeter GH, and van
der schans CP.(2001). Inspiratory muscle training in patients with cystic
fibrosis. Respir Med., 95: 31-36.
Enright, S, Chatman, K, Lonescu, A.(2004).
Inspiratory muscle training improves lung function and exercise capacity in
adults with cystic fibrosis. Chest, 2, 405-412.
Lisobia, C, Munoz, V, Beroza, T, Leiva, A, Cruz,
E, (1994). Inspiratory muscle training in chronic airflow limitation: A
compensation of two different training loads with a Threshold Device European
Respiratory Journal, 7, 1266-1274.
Citation: Syeda Khanam. P, Manjunatha. H, Thummala S. Pavani (2021). Effect of Inspiratory Muscle Training in Patients with Chronic Obstructive Pulmonary Disease on Dysponea and Exercise Tolerance, ijmaes; 7 (1); 933-942.