Rosintan Milana Napitupulu1, Novlinda Susy Anrianawaty Manurung2
Corresponding author:
1Physiotherapy Program, Faculty of Vocational Studies, Universitas Kristen Indonesia.
Mail id: rosintan.napitupulu@uki.ac.id
Co-Author:
2 Physiotherapy Program, Faculty of Vocational Studies, Universitas Kristen Indonesia
ABSTRACT
| Introduction: The composition of the elderly population is increasing rapidly in both developed and developing countries, which is caused by a decrease in fertility (birth) and mortality (death) rates as well as an increase in life expectancy, which changes the structure of the population as a whole. Stroke can generally occur in all age groups, but three quarters of strokes occur in people who are already 65 years old or older (the elderly) and result in the onset of disability or invalidity. Stroke is one of non-communicable diseases, which is the leading cause of death worldwide. Methodology: Data was taken from the integrated health service post (for the elderly) to obtain an overview of the risk of stroke in the elderly based on the available secondary health data of the elderly. Results: Two hundred and sixty-eight (268) elderly people with the available health data can be described by the following criteria: 56% of the elderly have low risk, 32% of the elderly have moderate risk, and 12% of the elderly have high risk. Conclusion: The elderly in the integrated health service post for the elderly have various risks of stroke from moderate to high. Keywords: Risk of stroke; Physiotherapy; Health status; Elderly |
| Received on 18th January 2021, Revised on 24th January 2021, Accepted on 20th February 2021; DOI:10.36678/IJMAES.2021.V07I01.002 |
INTRODUCTION
Stroke is one of non-communicable diseases, which is the leading cause of death 1,2. Stroke is included in cerebrovascular disease, which is a brain function disorder associated with the disease of a blood vessel that supplies blood to the brain3. Stroke is also called a brain attack which always occurs suddenly with various symptoms. However, most of the symptoms that are often found are the condition of the body that is half paralyzed and/or accompanied by decreased consciousness4. Stroke can generally occur in all age groups, but three-quarters of strokes occur in people who are already 65 years old or older (the elderly) and result in the onset of disability or disorders 5.
The large number of elderly people in Indonesia will have both positive and negative impacts. It has a positive impact if the elderly population is healthy, active, and productive. On the other hand, the large number of the elderly population becomes a burden if they have a problem of declining health which results in an increase in the cost of health services, a decrease in revenue/income, an increase in disability, the absence of social support, and an environment that is not friendly to the elderly population6.
Based on the magnitude of the problem that will arise due to stroke in the elderly, we consider it important to portray or describe the risk of stroke that exists in the elderly in sub-district of Cililitan, Jakarta, Indonesia as an area that is fostered by Universitas Kristen Indonesia. We processed the secondary data on the health of the elderly to describe the risks of stroke that exist in the elderly in this area. The research was conducted at the Integrated Health Service center for the elderly of Cililitan because it is one of the Integrated Health Service center that also fostered by the UniversitasKristen Indonesia, so further research is needed to increase the role of the university to the community in terms of health, disease prevention, and improvement of public health.
RESEARCH METHODOLOGY
The methodology of this research is a descriptive study by taking secondary data from the Integrated Health Service Centre for the elderly in Sub-District of Cililitan, Jakarta, Indonesia. The selection of this integrated health service post was based on its collaboration with the Universitas Kristen Indonesia, so that community service-based research could be carried out. The data taken was then processed using a cross sectional study method.
Secondary data was obtained from the report on the results of examining the general condition of the elderly made by health workers from the integrated health service post for the elderly with the examination period in March 2020. The data used is on routine health checks carried out by health care professionals at the integrated health service center for the elderly. The use of data in this study has received permission from the management of the integrated health service post by not displaying the identity of the elderly.
Data analysis: The data obtained is the health data of the elderly which includes: blood pressure, random blood sugar level, cholesterol, age, and sex. This secondary data was processed using Microsoft Excel software in order to obtain an overview of the risk of stroke in the integrated health service center for the elderly of Sub-District of Cililitan.
RESULTS and DISCUSSION
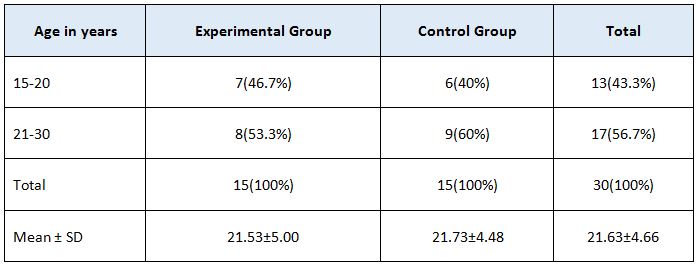
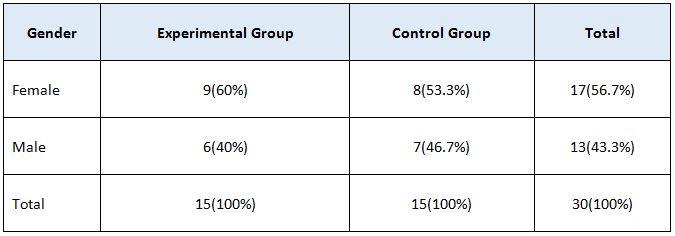
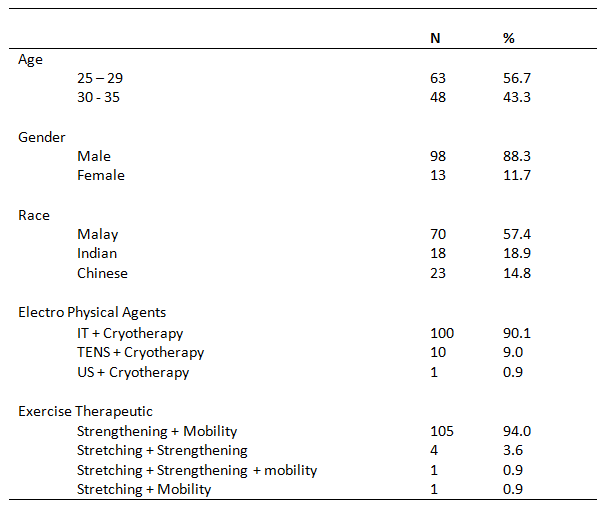
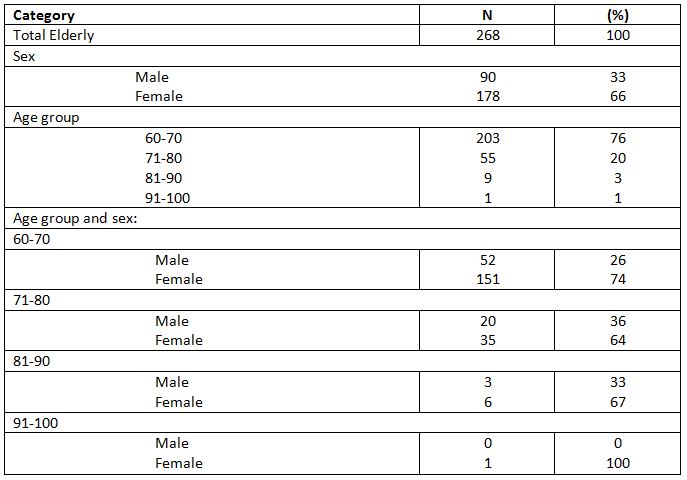
The following is the data obtained through the secondary data available in the integrated health service post for the elderly taken in March 2020. The data in Table 1 shows the profile of the elderly at the integrated health service center for the elderly.
Thereafter, from the profile of the elderly, the researchers continued to process the health profile data of the elderly consisting of the conditions of blood pressure, blood sugar, and cholesterol.
Based on the results of the profile data processing in the form of sex and age shown in Table 1 above, it is known that there are 268 elderly people consisting of 33% males (90 people) and 66% females (178 people), with 76% (203 people) in the age range of 60-70 years, 20% (55 people) in the age range of 71-80 years, 3% (9 people) in the age range of 81-90 years, and 1% (1 person) in the age range of 91-100 years. In this data, it is found that most of the elderly are female. In the study, stroke is more common in men aged 65-79 years although older women can also be at higher risk, namely those over 80 years 7,8.
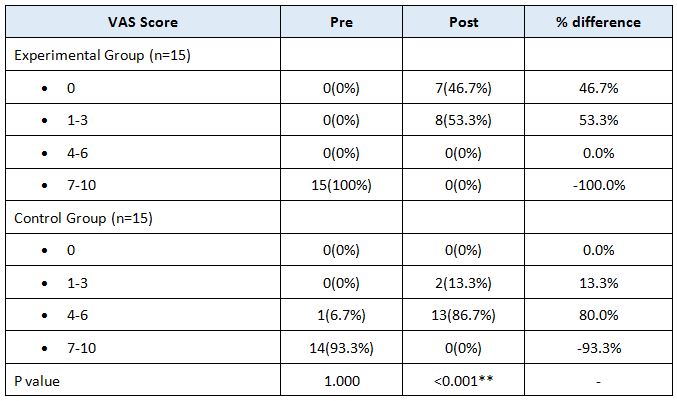
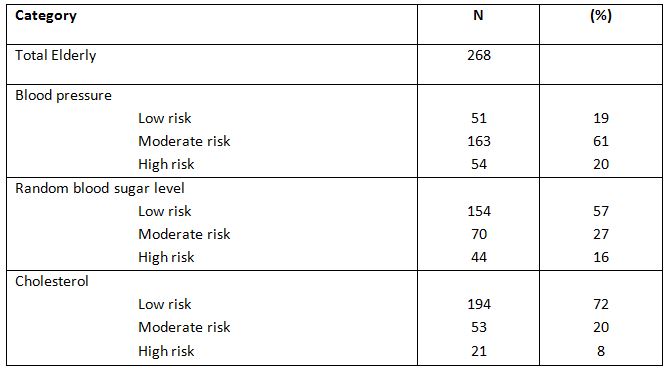
Based on the health profile shown in Table 3, there are three important factors that constitute indicators in the assessment of potential risks of stroke, such as:blood pressure, blood sugar, and cholesterol. A study also explains that those three indicators can be initial risk assessment for stroke conditions 5.
In the data processing table of the recorded results of medical examination based on blood pressure, it is concluded that 19% (51 people) of the elderly havea low risk potential, 61% (163 people) have a moderate risk potential, and 20% (54 people) have a high risk potential of stroke. It is also supported by a study conducted by Seshadri et al., which actually states that high blood pressure would result in higher risk of stroke in the elderly below 80 years old9. It is also visible from the data that such condition can also affect more than 70 percent of the elderly in the integrated health service center. A study conducted by Rodgers et al. also states that hypertension in the elderly can also result in a higher risk for the occurrence of stroke in the elderly5. A study conducted by Arboix et al. also states that high blood pressure conditions play a major role in increasing the risk of ischemic stroke in the elderly who are older than 85 years or more10.
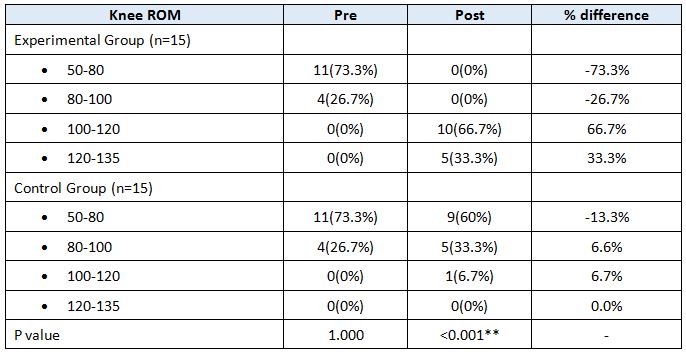
In the data processing table of the recorded results of medical examination based on random blood sugar level,it was found that 57% (154 people) of the elderly have a low risk potential, 27% (70 people) have a moderate risk potential, and 16% (44 people) have a high risk potential of stroke. In general, the blood sugar condition and other conditions such as food management are also influential to the risk level of strokein the elderly 11.
In the data processing table of the recorded results of medical examination based on cholesterol, it was found that 72% (194 people) of the elderly have a low risk potential, 20% (53 people) have a moderate risk potential, and 8% (21 people) have a high risk potential. It can be said that most of the elderly are still safe in terms of cholesterol contained in the blood as a stroke risk parameter. Nevertheless, high cholesterol levels in the blood can be one of the risks that result in stroke among the elderly4. A study conducted by Reddy et al. stated that, besides the risks of diabetes and hypertension, dyslipidemia, obesity, smoking, and drinking alcohol can also increase the risk of stroke in the elderly12.
In this study, there were still more elderly women who came regularly, so that the data presented has not covered all the elderly. The data displayed is also only the data taken in the month of March. The activities in the integrated health service post for the elderly need to be enhanced with simple exercises that can increase physical activity in the elderly to help improve general health 13.
Ethical Clearance: Ethical clearance has obtained from Universitas Kristen Indonesia, Jakarta, Indonesia to conduct this study with reference number: 309/UKI.F8.D/PPM dated 01/06/2020.
Conflicts of Interest: The author declares that there is no competing interest in publishing this article.
Fund for the study: This is self-funded study.
Recommendation: The participation of elderly men in the integrated health service post needs to be increased, so that the elderly men who are at risk can be recorded because, based on data, many men have the risk of stroke. Health examination in the integrated public health service center for the elderly needs to be conducted regularly which needs to be supplemented with exercises or gymnastics for the elderly to improve their health condition. Simple exercises to increase physical activities can improve the health condition of the elderly.
CONCLUSION
As a conclusion, the elderly in the integrated health service center have quite various stroke risk potentials from moderate to high. In such conditions, information about health condition needs to be disseminated about the basic risks that would result in stroke also with initial handling for the prevention of stroke.
REFERENCES
- Hu, G., Sarti, C., Jousilahti, P., Peltonen, M., Qiao, Q., Antikainen, R., &Tuomilehto, J. (2005). The impact of history of hypertension and type-2 diabetes at baseline on the incidence of stroke and stroke mortality. Stroke, 36(12),2538-2543.
- Feigin, V. L., Krishnamurthi, R. V., Parmar, P., Norrving, B., Mensah, G. A., Bennett, D. A., & Davis, S. (2015). Update on the global burden of ischemic and hemorrhagic stroke in 1990-2013: the GBD 2013 study. Neuroepidemiology, 45(3), 161-176.
- Dávalos, A. (2005). Thrombolysis in acute ischemic stroke: successes, failures, and new hopes. Cerebrovascular Diseases, 20 (Suppl. 2), 135-139.
- Chen, R. L., Balami, J. S., Esiri, M. M., Chen, L. K., & Buchan, A. M. (2010). Ischemic stroke in the elderly: an overview of evidence. Nature Reviews Neurology, 6(5), 256-265.
- Rodgers, H., Greenaway, J., Davies, T., Wood, R., Steen, N., & Thomson, R. (2004). Risk factors for first-ever stroke in older people in the north East of England: a population-based study. Stroke, 35(1),7-11.
- Parr, E., Ferdinand, P., &Roffe, C. (2017). Management of Acute Stroke in the Older Person. Geriatrics, 2(3),27.
- Appelros, P., Stegmayr, B., &Terént, A. (2009). Sex differences in stroke epidemiology: a systematic review. Stroke, 40(4), 1082-1090.
- Arboix, A., Oliveres, M., García-Eroles, L., Maragall, C., Massons, J., & Targa, C. (2001). Acute cerebrovascular disease in women. European neurology, 45(4), 199-205.
- Seshadri, S., Wolf, P. A., Beiser, A., Vasan, R. S., Wilson, P. W., Kase, C. S., & D’Agostino, R. B. (2001). Elevated midlife blood pressure increases stroke risk in elderly persons: the Framingham Study. Archives of internal medicine, 161(19), 2343-2350.
| Citation: Rosintan Milana Napitupulu, Novlinda Susy Anrianawaty Manurung (2021). Overview of the health profile of the elderly referring to the risks of stroke in the Sub-district of Cililitan, Jakarta, Indonesia , ijmaes; 7 (1); 927-932. |