SITI NUR BAAIT BINTI MOHD SOKRAN1, ROGINI A/P PERIASAMY2, JIBI PAUL3
Corresponding Author:
1Lecturer, Department of Physiotherapy, School of Health Sciences, KPJ Healthcare University College, Nilai, Malaysia. Mail id: sitinurbaait@kpjuc.edu.my
Authors:
2 Physiotherapist, Department of Physiotherapy, KPJ Selangor Specialist Hospital, Selangor, Malaysia.
3Professor, Faculty of Physiotherapy, Dr.MGR Deemed to be University, Chennai, Tamilnadu, India.
ABSTRACT
Purpose: Intra-rater reliability refers to the consistency of measurements demonstrated in similar assessment situation at two different times by the same examiner which also refers to test-retest. Inter-rater reliability test denotes the consistency of assessments performed by two different examiners. The objective of the study was to determine the inter-rater and intra-rater reliability between experienced and non-experienced physiotherapist on 90-90 active knee extension test using goniometer among healthy college students.
Methodology: This study method is a reliability design in determining hamstring flexibility among 42 young healthy college students of School of Physiotherapy, KPJ Healthcare University College, Nilai, Malaysia. The 90-90 active knee extension was performed using goniometry. Four physiotherapists involved in the study consist of two non-experienced physiotherapist and two experienced physiotherapists.
Results:The mean and standard deviation of active knee extension 90-90 Active Knee extension test among two experienced physiotherapist were 19.830(SD= 10.21) and 43.14 (SD= 47.05). Mean and standard deviation for two non-experienced physiotherapist value were 21.21(SD 11.14) and 42.55 (47.66).
Conclusion:The conclusion of the inter-rater and intra-rater evaluation between experienced and non- experienced physiotherapist showed that goniometer is a reliable tool to evaluate hamstring flexibility among healthy college students.
ISHWARYA VARDHINI C1, DENNIS ROBINSON2, JIBI PAUL3
Corresponding Author: 1Asst.Professor, Faculty of Physiotherapy, Dr. MGR Educational and Research Institute, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India. Mail id: ishphysio@gmail.com
Authors: 2Professor, Department of Physiotherapy, KG College of Physiotherpy, Coimbatore, Tamilnadu, India. 3Professor, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India.
ABSTRACT
Background of the study: Chronic obstructive pulmonary disease (COPD) is the 5th cause of mortality and morbidity in the world and represents an economic and social burden. Chronic obstructive pulmonary disease is a chronic pulmonary disorder affecting 10%-15% individuals over age of 45 years. Objective of the study is to compare the effect of conventional pulmonary rehabilitation and Global Postural Re-education method on pulmonary function and thoracic expansion in patients with moderate chronic obstructive pulmonary disease. Methodology: Thiswas an experimental Study of two groups’ with pre-post comparative study design.The study was conducted for a period of six months in the department of Pulmonology, K.G.Hospital and postgraduate research and medical institute, Coimbatore. All adult patients attending the Pulmonology department of the hospital were assessed and selected for the study. A total of 20 patients with moderate chronic obstructive pulmonary disease were selected by random sampling method and were divided into 2 groups A and B. Pulmonary function test (FEV1/FVC) and Thoracic expansion at Axillary and Xiphoid level was measured and recorded. Unpaired ‘t’test used to find the difference between two groups. Result: Tvalue for FEV1/FVC was 7.313, thoracic expansion was 11.90 and 16.39 at Axillary & Xiphoid respectively between two groups with ‘P’ value <0.05. The study showed that there is a significant difference in improvement of FEV1/FVC ratio and thoracic expansion in Group-B, who underwent Global postural re-education method. Conclusion: Global postural re-education method is better intervention in the improvement of pulmonary function, thoracic expansion in patients with moderate chronic obstructive pulmonary disease.
2 BPT Intern, Faculty of Physiotherapy, DR.MGR.Educational and Research Institute, Velappanchavadi, Chennai,India
Corresponding Author:
Professor, Faculty of Physiotherapy, ACS Medical College and Hospital, Dr M.G.R. Educational and Research Institute University, Chennai. Mail id: physojibi@gmail.com
ABSTRACT
Back and objective of the study: Individual with neck pain that lack an identifiable patho-anatomic cause for their symptoms are usually classified as having mechanical neck pain. Stretching is believed to provide many physical benefits including improved flexibility, injury prevention, improved muscle or athletic performance. Aim of the study was to find out the effects of static stretching and dynamic stretching on mechanical neck pain and also to compare the effectiveness between static and dynamic stretching on mechanical neck pain.
Methodology: Comparative study with Quasi Experimental design conducted at ACS Medical College and hospital, Chennai. Both genders of thirty patients were selected for the study. Convenient sampling method used to select the samples on the basis of selection criteria. Visual analogue scale and neck disability index were used as measurement tools for data collection. The study conducted for duration of four weeks.
Results: The results shows significant difference in neck pain and neck function between static stretching and dynamic stretching with F value 1733 and <0.0001. Static stretching found more effective than and dynamic stretching with more mean difference of VAS and NDI scores 5.33 and 22.8 compared to 1.73 and 12 respectively.
Conclusion: The static stretching is more effective than dynamic stretching in improving pain and functional disability in patients with mechanical neck pain.
1 Principal, East Point College of Physiotherapy, Jnana Prabha, Bidarahalli, Virgo Nagar, Bangalore, India, Mail id: manjuinlife@gmail.com
Co Authors:
2 Professor, Faculty of Physiotherapy, DR MGR Educational and Research Institute, Velappanchavadi, Chennai,India 3 Associate Professor East Point College of Physiotherapy, Jnana Prabha, Bidarahalli, Virgo Nagar, Bangalore, India.
ABSTRACT
Background and objective: Trunk control is a crucial component to perform motor function and also to maintain good posture. Trunk gives background for moving upper limbs and lower limbs. The objective of this study was to find out the effectiveness of selective trunk activities in rehabilitation of hemiplegia.
Methods: It is a pre and post experimental design. 30 patients have participated and were divided into two equal groups. i.e, experimental and control group, with 15 subjects in each group. Experimental group received routine neuro-rehabilitation along with selective trunk activities, whereas, control group received only routine neuro-rehabilitation program. Pre and post assessment of trunk balance and impairment was measured by using Trunk Impairment Scale (TIS) and Rivermead Motor Assessment Protocol (RMAP).
Results: Before the treatment mean values of both control and experimental groups were approximately equivalent There was a significant increase in the mean value of the TIS and RMAP in the experimental group than that of the control group.
Conclusion: Posture and stability are the key factors in maintaining proper balance of the trunk. Hence, selective trunk activity has a significant improvement in trunk balance and postural stability and could be considered as an important part in rehabilitation of hemiplegia.
S. GLADIES KAMALAM1 , G. SRIVIDYA2 , J. ANDREWS MILTON3
Corresponding Author:
1 Associate Professor, Bethany Navajeevan College of Physiotherapy, Kerala, India. Mail id: mail2drsgk@gmail.com
Co Authors:
2 Research Guide, Department of PMR, Annamalai University, Tamilnadu, India. 3 Research Co- Guide, Bethany Navajeevan College of Physiotherapy, Kerala, India.
ABSTRACT
Background: Over ages; bronchial asthma and its adverse physiological, psychological impacts upon varied group of age, people, and health remains a searchable quest in its depth. Behaviour modification as an emerging outlook of Physical therapy helps to exhibit positive changes in this broad spectrum of asthma. This study aimed to identify the possible potential factors to improve chest expansion by analysing the effect of buteyko breathing and relaxed postures.
Methods: Experimental study design; 20 patients of the age group 17-19 years were selected using simple random sampling method. Group A; consisting 10 patients were advocated buteyko relaxation training. Group B; consisting of 10 patients were advocated relaxed postures along with the conventional asthma management. Stop watch, nose clip, inch tape, pediatric asthma quality of life questionnaire [PAQLQ] were used as the operational tools. Paired and Unpaired “t” testing was used to analyze the pre- test and the post- test values after a period of 6 months.
Results: Analysis of the peak expiratory flow rate and the quality of life over Group “A” and Group “B” at 0.05% level of significance showed positive results for Group “A” when compared with the ‘t’ value.
Conclusion: The findings support the multidimensional positive effects of behavior modification over the physiological and psychological parameters that lead to the onset of bronchial asthma.
Keywords: Bronchial asthma, behavior modification, buteyko breathing, relaxed postures, peadiatric asthma quality of life questionnaire
KANCHAN A. KATRE1 , VIJAYAKUMAR PUSHPARAJ 2 , JIBI PAUL3
Authors:
1 Faculty of Physiotherapy, P.E.S Modern college of Physiotherapy, Modern College road, Pune-5, Maharastra, India .
3 Faculty of Physiotherapy, DR.MGR.Educational and Research Institute, Velappanchavadi, Chennai,India
Corresponding Author:
2 Professor, Rajarajeswari College of Physiotherapy, Kambipura, Mysore Road, Bangalore, Karnataka, India. Mail id: vijayrrc@yahoo.com
ABSTRACT
Introduction: The objective of the study was to determine the
effectiveness of Otago exercise program (OEP) and strength training program
(STP) on lower limb strength and risk of fall among bilateral knee
osteoarthritis patients and compare its effects.
Method: Subjects diagnosed with bilateral knee osteoarthritis
were included and randomly assigned into group A ( N=20) and group B ( N=20).
Subjects in Group A received otago exercise program and strength training
program in group B. All the subjects were assessed with baseline and post
intervention outcome measure for risk of fall with The Time up and Go test
(TUG) and lower limb strength with 30-sec Chair Stand Test.
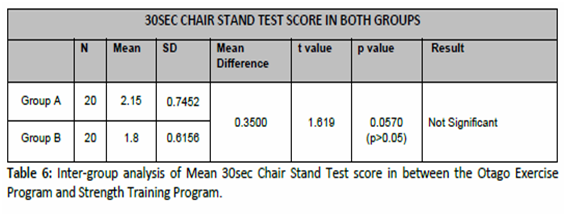
Result: This study shows that the mean score Inter-group
analysis of time up go test (TUG) in between Otago Exercise Program and
Strength Training Program group shows (p < 0.05) with significant
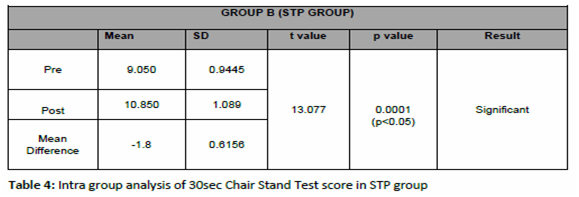
improvement and with mean score of 30sec Chair Stand Test (30sec CST) on the Lower
limb strength in between Otago Exercise Program and Strength Training Program
group shows no significant improvement with p value of 0.0570 (p>0.05).In
intra group analysis the time up go test shows significant result in OEP group
but not in STP group and with the 30 – sec chair stand test showed significant
result in both the groups.
Conclusion: The study showed that otago exercise program is
effective in reducing the risk of fall and improving lower limb strength among
bilateral knee osteoarthritis than Strength training program.
Keywords: Osteoarthritis , Otago exercise program, strength training program, time up and go test, 30-sec Chair Stand Test and risk of fall.
Received on 11th February 2019, Revised on 24th February 2019, Accepted on 28th February 2019
INTRODUCTION
Osteoarthritis (OA) is a prevalent
disease characterized by structural changes in cartilage, bone, synovium, and
other joint structures1. Osteoarthritis is estimated to be the eighth leading
non-fatal burden of disease, accounting for 2.8% of total years of living with
disability2. It is the most prevalent and disabling chronic diseases
affecting the elderly causing progressive dysfunction of articular cartilage
which results in impaired joint motions, severe pain, and disability3.
The ageing process is accompanied by a decline in function of systems that are
responsible for the control of balance 4.
Osteoarthritis of the knee is
associated with disability due to pain, quadriceps dysfunction, and impaired
proprioception. Quadriceps dysfunction in OA knee includes impaired
proprioception, especially in the more extended knee joint positions; impaired
ability to accurately and steadily control submaximal force and impaired
eccentric strength5. These proprioceptive deficits may contribute towards
reduced dynamic knee stability. The integrity and control of sensorimotor
systems i.e. proprioceptive acuity and muscle contraction,are essential for the
maintenance of balance and production of a smooth and stable gait.It has been
established that proprioceptive acuity, joint movement and sense of resistance
declines both with age and as a result of OA 6,7.
Pattern of muscle use changes as an
individual ages8. Out of more than 400 risk factors for fall9, lower limb
weakness and decreased balance are the two of the most easily modifiable risk
factors. Fall rates increase with age10 and the frequency of fall is higher
among women than men11. With the increasing age, approximately after the age of
60 years, a person’s physical ability, including gait speed,muscle strength,and
balance, generally declines, so the incidence of fall and the severity of fall
related complications increase 12,13,14.
Timed Up & Go Test (TUG) is a
test for balance that is commonly used to examine functional mobility in
community-dwelling, frail older adults with age group between 70–84 years15 and
appears to be a valid method for screening for both level of functional
mobility and risk for fall in community-dwelling elderly people16. Also the
30-sec chair stand test provides a reliable and valid indicator of lower body
strength in generally active, community-dwelling older adults17.
Balance and gait training are important components of any
exercise program aimed at decreasing the risk of fall among older adults, so
any exercise program for older adults should include exercises to improve both
strength and balance18. Evidence has shown that certain rehabilitation
exercises such as the Otago exercise program and Fall Management exercise are
effective in returning fall patients to normal functional movement if the
patient adheres to the routine19.
The Otago Exercise Program (OEP) is
a fall prevention program which addresses the risk factors of poor balance and
lower limb weakness with an individually prescribed, home based strength and
balance exercise program in older adults. There are only very few studies about
Otago Exercise Program focusing on reducing fall risk in older adults having
bilateral osteoarthritis of knee. Also few studies have stated that the
Strength training of the lower limb muscle helps to improve physical
performance and reduce disability along with improving the strength of muscles
in the community-dwelling elders with bilateral osteoarthritis of knee22.
But there are very few studies done for reducing the risk of fall in older
adults with bilateral osteoarthritis of knee by using Otago exercise program.
Hence, the main purpose of this study was to determine whether there is effect
of Otago Exercise Program over strength training program for 8 weeks in
reducing the risk of fall and improving leg strength in older adults having
bilateral osteoarthritis of knee.
Objective of the study: The
main objective of the study was to determine the effect of Otago exercise
program and strength training program and compare the effectiveness Otago
exercise program over strength training program on leg strength and risk of
fall among bilateral knee osteoarthritis patients.
METHODOLOGY
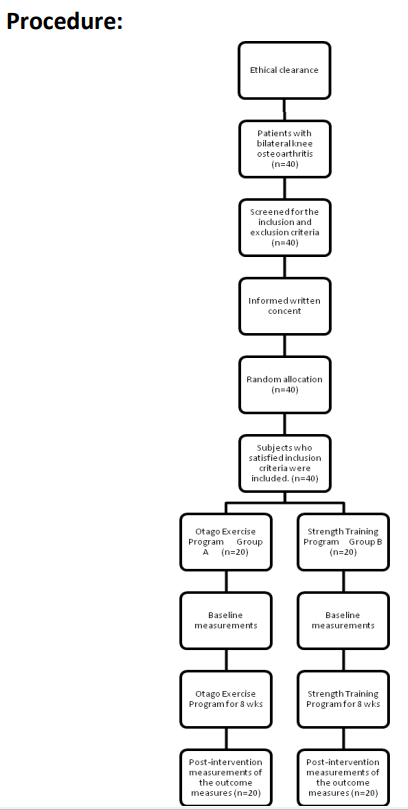
This was a randomized clinical
trial study design conducted after obtaining the approval from the
Institutional Ethical Committee (IEC) of PES Modern college of Physiotherapy,
Pune. The subjects who reported to the outpatient department (OPD) of the study
setting at PES Modern college of Physiotherapy, Pune with bilateral knee
osteoarthritis were selected and screened for the inclusion and exclusion
criteria. Those subjects who satisfied the inclusion criteria were included for
the study. Total 40 subjects (n=40), of both male and female gender between age
group of 60 to 69 years were included for the study and a written informed
consent was obtained from each of the forty subjects, after explaining about
the detailed procedure of the study. Then the selected subjects were randomly
allocated into group A and group B with 20 subjects in each group. Group A (
N=20) received Otago Exercise Program (OEP) which contains strength training,
balance training and walking program. Group B ( N=20) received Strength Training
Program (STP), which contains only strength training. Each subject in both the
groups received an exercise activity booklet of the respective exercise
program, with illustrations and instructions about the program. All the
subjects were instructed to wear comfortable clothing which should not be too
tight or too loose while performing exercises. The subjects in each group were
assessed for the baseline outcome measurement and post intervention outcome
measurement with TUG test and 30 sec Chair Stand Test. The subjects in both the
group were explained about the study and intervention in the language best
understood by them. They were encouraged to clarify questions regarding the
study if any. The baseline measures were recorded prior to intervention and post
intervention measurements were recorded 8 weeks after intervention.
After obtaining the baseline measurement and during each session from day one, subjects in both groups were given a common treatment with Interferential Therapy with the frequency with range of 0-100 Hz, followed by the respective exercise program35. Later, the subjects performed the warm up for the period of 10 minutes, followed by the respective interventional program for a period of 20 minutes and followed by the cool down exercises for 10 minutes. The exercises which were performed for the warm up and cool down program were: Marching in place, Calf stretching, Hamstring stretching and Illiotibial band stretch.
Figure 1: Flow diagram showing the process used in the study
Group A: Otago Exercise Program Group (OEP Group):
The subjects in this group received
OEP training, 3 days in a week for 8 weeks (total = 24 sessions), with 40 mins
per session. Each session included 10 mins of warm up and 10 mins of cool down
exercises. The Otago Exercise Program (OEP) is a fall prevention program which
addresses the risk factors of poor balance and lower limb weakness with an
individually prescribed, home based exercise program for older adults31. Otago
was developed to prevent fall among older adults. It is a set of exercise
program consisting leg muscle strengthening, balance retraining and walking.
Before starting the intervention, the subjects were briefed, demonstrated about
the procedure of the exercises and also were assured for the correct performance
of the exercise like, never exercise by holding on to an object which may move
and not stable, follow the correct pattern of breathing, work in a pain free
range, take rest interval while doing the exercise and to report to the
researcher in case of any breathlessness, dizziness or chest pain in between
the sessions.
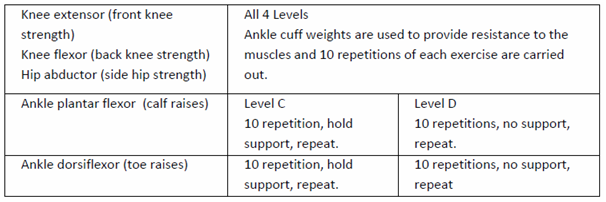
Strengthening exercises:
The strengthening exercises in the
OEP group were performed with various levels from A to D. All levels were
performed with ankle weights for knee flexors, knee extensors and hip
abductors. Body weight was used for resistance to the ankle dorsiflexor and
plantarflexor. The level C was performed with support and level D without
support. The progressions were executed when patients were able to do 2 sets of
ten repetitions with each exercise. The starting level resistance for the
exercise for each muscle group in each leg was determined by the amount of
ankle weight the patient can lift to perform 10 good quality of repetitions
before fatigue.
It was started by providing 1 kg weight, it is
to warm up the muscles which minimizes both muscle soreness and compliance
problems, then subjects were asked to rest for 1 min time period and ½ kg
weight was added to the warm up load to perform 10 repetitions without fatigue,
after giving 2 min rest period, again ½ kg weight was added and the subjects
were asked to perform 10 repetitions. If subject was able to perform 10
repetitions without fatigue then that weight was fixed as a resistance for the
exercises, and if subject was not able to do the repetitions withoutfatigue,
then after reducing the weight by 250 gm subjects were asked to continue the
exercises with that weight for resistance.
The subjects were instructed to do the exercises slowly through the functional range of active joint movement with two or three seconds to lift the weight and four to five seconds to lower the weight. They were instructed to take two min rest in between the sets.
Figure 2 : Exercise protocol
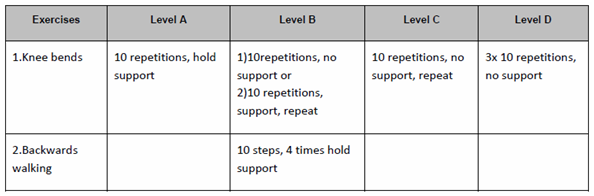
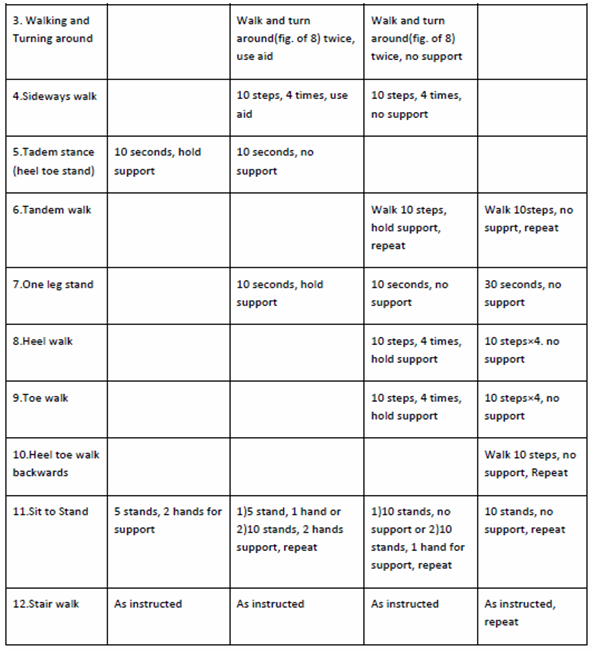
Balance re-training Exercises:
The balance exercises in the OEP
were performed with levels from A to D. level A consist of knee bending
exercise, tandem stance, sit to stand and stair walking exercises performed by
the subjects. Level B consist of knee bending, backward walk, walking and
turning around, sideways walk, tandem stance, one leg stand, sit to stand and
stair walking exercises. Level C consist of knee bending, walking and turning
around, sideways walk, tandem stance, one leg stand, heel walk, toe walk, sit
to stand and stair walking exercises.
Level D consist of knee bending, backward walk, tandem walk, one leg stand, heel walk, toe walk, heel toe walk backwards, sit to stand and stair walking exercises. Balance exercises progress from holding on to a stable structure to performing the exercise independent of support. The subjects were made sure that they can recover their balance using lower body strategies before prescribing the exercises without support. Unstable subjects initially needed a wider base of support and all were instructed to look ahead while doing exercises. There are 12 balance exercises, with 4 levels of difficulties, which are as follows:
Figure 3: Twelve balance exercises
Walking: Subjects were asked to include walking in the exercise program to help increase physical capacity by wearing comfortable shoes and clothing. Before they start walking, warm up exercise i.e. marching on a place for two minutes should have done by the subjects. While walking subjects should look ahead, shoulders should be relaxed and arms gently swing, use walking aids if any, use prescription eyeglasses if advised, do not go outside if it is too cold or too warm, walk at a normal and not a fast pace, walk in a maintained, and well lit area. For walking, subjects should aim for up to 30 minutes, by breaking the session into shorter sessions (three 10-minute sessions), walking at their usual pace, at least twice a week. The walking should only incorporate walking plan when they are physically ready and able. They should begin walking indoors and progress to walking outdoors when strength and balance have improved.
Group B: Strength Training
Program Group (STP): The subjects in this group received STP, 3 days in a
week for 8 weeks (total = 24 sessions), with 40 minutes per session. Each
session included 10 minutes of warm up, 20 minutes of strengthening program,
and 10 minutes of cool down exercises. Strength Training program focused on
strengthening the lower limb muscle groups i.e. hip flexors, hip extensors, hip
abductors, knee flexors and knee extensors with the help of theraband in a
color with which a subject could perform 3 sets of 10 repetitions while
selected for training.
Initially the exercises were performed
without resistance to make subjects comfortable. Before starting the exercise
protocol, the resistance level was determined by giving yellow band to all of
the subjects and they were instructed to perform 3 sets of 10 repetitions along
with the rest intervals in between the sets, for 3 minutes. If subject was able
to comfortably complete the repetitions, progression was done by changing the
next color band i.e. red color band. If subject was not able to complete the
repetitions, then resistance for strengthening was decided by returning to the
previous level.
The secure anchoring of theraband
was assured to a steady object before starting the exercises and subjects were
asked to perform all exercises in a slow and controlled manner. They were instructed
to perform all the exercises by maintaining the normal spinal curves, and not
to lock the joints, or avoid hyper-extending and over flexing them. All
subjects were instructed to work in a pain free range, to take the rest
interval while doing the exercise and to follow the correct pattern of
breathing. They were also instructed to report to the researcher in case of any
breathlessness, dizziness, and chest pain in between the sessions.
Selection criteria:
Inclusion criteria: The
inclusion criteria for this study were as follows:
Both male and female participants
with age group between 60-69 years, Bilateral knee osteoarthritis, Complain of
knee pain3, Complain of less than 30 minutes of morning knee joint stiffness3,
Crepitus on active movements in knee joint3,Complain of bony tenderness around
knee joint line3, TUG score of 14 sec and above27.
Exclusion criteria: Subjects
were excluded if they had21, 24, 25: Any history of surgery around the knee,
history of injury around the knee, deformity, neuromuscular disorders, and
cardiovascular disorders.
Outcome measurements: The
outcome measures used for this study were Time up and go test and 30-Sec chair
stand test.
The Time up and Go test (TUG): In
this study the risk of fall in bilateral knee osteoarthritis were assessed with
TUG test. Here the patients were made to sit on the standard armchair with seat
height of 18 inc16. The chair was having adequate back rest and positioned in
such way that it didn’t move when the subject is performing the test.
The subject
was asked to stand from the chair on the word “go” and walk at comfortable
speed to the line marked on the floor 3 meters away from the chair then, turn
around and return to sit on the chair. The subjects were timed from the word
“go” until they return back to the sitting position. The data was recorded in
seconds by using stopwatch. The older adults who take longer than 14 seconds to
complete the TUG test have a high risk for fall16.
30-sec
Chair Stand Test: Lower limb strength
was tested with the 30 second chair stand test, which has been found to be a
reliable and valid test, with a moderate correlation to weight adjusted 1
repetition maximum leg-press strength17. The subjects were asked to sit in a
chair with seat height of 17 inc17, without armrest. The arms of the subjects
were crossed at the wrist and held against the chest during the test. The
subjects were asked to perform the test after the word “go” by standing up
straight and sitting down on the chair as many times as possible in 30 seconds
. The data was recorded until the subjects complete the number of stands in 30
seconds. At the end of 30 seconds if a participant was more than halfway up,
the stand was counted. A score of 0 was awarded if any form of hand support was
used. The test was stopped if any loss of balance occurred.
Variables:
The variables used in the study were:
Dependent
variables:
Risk of fall
Leg strength
Independent
variables:
Otago exercise program (OEP)
Strength training program (STP)
Materials
Used: Following materials were used
for the recording purpose:
Measuring tape.
Stop watch.
Chair with straight back without arm rest.
Chair with straight back with arm rest.
Weight cuffs.
Thera band.
RESULT
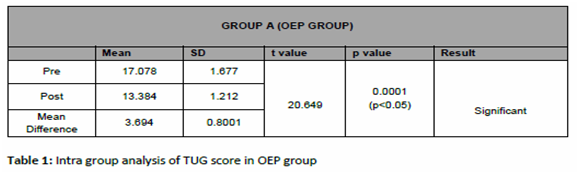
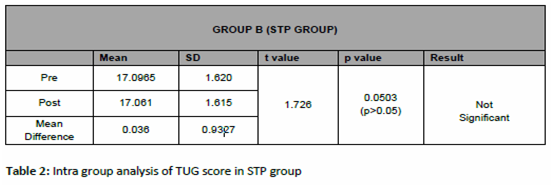
The significance of outcome measure with time up go test (TUG) on the risk of fall among bilateral knee osteoarthritis in OEP group is reflected in table 1, with p value of 0.0001 which is less than 0.05 (i.e. p<0.05) showing statistically significant results in improving the post intervention measurement score of TUG test. The significance of outcome measure with time up go test (TUG) on the risk of fall among bilateral knee osteoarthritis in STP group is reflected in table 2 ,p value of 0.0503 which is more than 0.05 (i.e. p>0.05) showing no statistical significant results in improving the post intervention measurement score of TUG test.
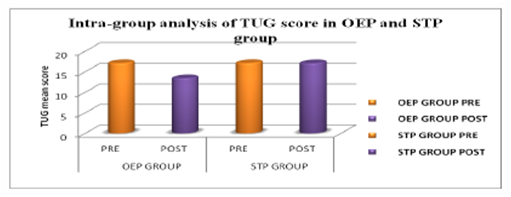
Graph 1: Graphical presentation of Intra-group analysis on TUG score in Otago Exercise Program and Strength Training Program.
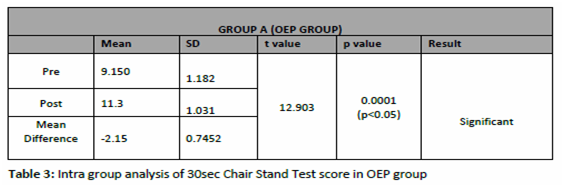
The significance of outcome measure with 30 second chair stand test (30sec CST) on the Lower limb strength among bilateral knee osteoarthritis in OEP group is reflected in table 3, which is less than 0.05 (i.e. p<0.05) showing statistically significant results in improving the post intervention measurement score of 30sec CST. And table 4 reflects the outcome measure with 30 second chair stand test (30sec CST) on the Lower limb strength among bilateral knee osteoarthritis in STP group with value less than 0.05 (i.e. p<0.05) showing statistically significant results in improving the post intervention measurement score of 30sec CST.
The significance of outcome measure of Inter-group analysis of Pre-intervention score with time up go test (TUG) in OEP group is 17.078 and STP group is 17.0965 with t value of 0.03644 and p value of 0.4856, which shows no significant results (p>0.05). The result shows that there is no discrimination in the pre scores of TUG test between both the groups. And the outcome measure with 30sec Chair Stand Test (30sec CST) on the Lower limb strength with pre-intervention mean score of OEP group is 9.15 and STP group is 9.05 with t value of 0.2956 and p value of 0.3846, which shows no significant results (p>0.05). The result shows that there is no discrimination and significant improvement in the pre test scores of 30sec CST between both the groups.
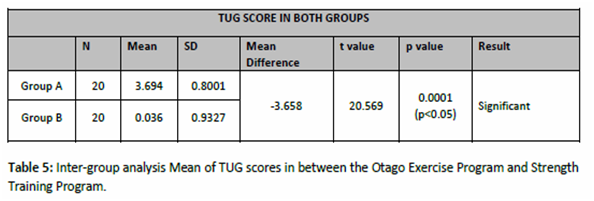
The significance of outcome measure of Inter-group analysis of mean score of time up go test (TUG) in between Otago Exercise Program and Strength Training Program group is reflected in table 5 which shows t value of 20.569 (p < 0.05) with statistical significant improvement when compared in between the two groups i.e. OEP group and STP group.
The significance of outcome measure of Inter-group analysis with mean score of 30sec Chair Stand Test (30sec CST) in between Otago Exercise Program and Strength Training Program group is reflected in table 6 which shows t value of 1.619 ( p>0.05) with no statistical significant improvement when compared in between the two groups i.e. OEP group and STP group.
DISCUSSION
The
purpose of this study was to determine the effect of Otago exercise program
(OEP) on risk of fall and leg strength, and to compare these effects with
Strength Training Program (STP) among patients with bilateral knee
osteoarthritis. In OEP group ( Group A) the results showed that there was
statistically significant improvement on the risk of fall with TUG test and leg
strength with 30sec Chair Stand Test in OEP (group A). On the other side the
subjects in the STP (group B) showed statistical significant improvement on
lower leg strength with 30sec chair stand test, but there was no statistical
significance demonstrated on risk of fall with TUG. And on comparison between
the groups there is statistical significant difference on risk of fall with TUG
score, whereas there is no statistical significant difference with 30sec chair
stand test for lower leg strength.
Thus,
it showed that the OEP is effective in improving both the outcome measures,
than on STP which showed improvement only on lower leg strength.The results is
supported by Province et.al.21 that exercises including balance
retraining reduces risk of fall in older adults. Similarly it is stated that
morelimitation in functional ability in subjects with poor
proprioception26, which is observed in patients with knee OA, where
there is articular damage reducing the quadriceps motorneuron excitability
leading to decrease in voluntary quadriceps activation. Thus, contributing to
quadriceps weakness and diminished proprioceptive acuity. This arthrogenic
impairment in quadriceps sensorymotor function and decreased postural stability
is proved to be associated with reduced functional performance of the
patients36. Also the physical function improves contributing to an effective
reduction in fall among elderly people on strength and balance training29.
In addition, strengthening
exercises using body weight have demonstrated a decrease in accidental fall9.
The training in the OEP group of this study improves the functional ability
which results in improved balance. And on the other outcome measure with 30sec
CST in OEP group the results showed significant results in improving 30sec CST
score indicating that there is improvement in leg muscle strength, which is
important to perform day to day activities, transferring, walking, etc. in
elderly bilateral knee osteoarthritis patients. The exercises which were
included in the OEP, helped to improve the strength of the leg musculature in
and around the knee joint reflecting on the 30sec CST, supported by Joshua N.
Farr (2010)23, that patients with osteoarthritis of the knee, improved muscle
strength when engaged into structured resistance exercise program. And
exercises using body weight as a resistance with sufficient intensity improves
the strength in the lower limb9.
The STP (group B) showed with no
statistical significant improvement on TUG but it showed statistically
significant improvement on 30sec CST, this result showed that there is
improvement in functional leg strength but not on risk of fall which reflected
on TUG. The result of this study is supported by Moreland JD et.al.(2003)30,
the strength training alone is not effective in reducing the risk of fall in
older adults. This result could be due to the effect of strengthening
exercises, which is mainly on improving the strength of leg musculature than on
improving balance, which is the most important reason to reduce risk of fall in
older adults with bilateral knee osteoarthritis. As stated by Julie M Chandler
(1997)22 the lower extremity strength gain with the help of strengthening
exercises is associated with gains in chair rise performance, gait speed, and
in mobility tasks, but not with improved balance, endurance, or disability. It
is likely that impaired balance is a stronger risk factor for fall than poor
muscle strength. Some studies have found the similar results that the strength
training is more effective in improving the leg strength than improving balance
in elderly people31,32. Similar results observed by Foley et.al.(2003)33,28
showed that the 8 of strength exercises on individual with lower extremity
osteoarthritis improves strength, walking distance and physical function.
Robert Topp et.al. (2002)18 also found that the resistance training improves
the strength and functional ability of patients with bilateral knee OA.
In addition to the above reason, inclusion of walking in the
exercise program, also showed improvement in results, and other studies have
shown that walking programs have health benefits including improved fitness,
weight loss, and lower blood pressure34. With appropriate prescription and
supervision, exercise that challenges balance can be administered safely in the
elderly population.
For example, it has been
demonstrated that the Otago Exercise Program is feasible and safe for older
people to undertake at home and have produced 35% reduction in fall and
fall-related injury37.
Hence, the present study provides
strong evidence that Otago exercise program has its effect both in reducing the
risk of fall and increasing the leg strength in older adults with bilateral
osteoarthritis of knee than compared with Strength Training Programme group.
CONCLUSION
This present study provides
promising results in reducing risk of fall and improving leg strength with the
help of Otago Exercise Program which is the combination of strength training,
balance retraining and walking program, as compared with the Strength training
Program in the older adults with bilateral knee osteoarthritis. So on the basis
of the present study, it can be concluded that the Otago Exercise Program is
effective in improving the leg strength and reducing the risk of fall, and can
be used in the exercise program of older adults with bilateral osteoarthritis
of knee.
REFERENCES
Felson DT, Lawrence RC, et al. (2000). Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med.. 8;133,635-646.
Wolf AD, Pfleger B, et.al. (2003). Burden of Major Musculoskeletal Conditions. Policy and Practice. Special Theme-Bone and Joint Decade 2000-2010. Bulletin of the World Health Organization. 81;9, 646-656.
R. Altman, E. Asch, et al. (1986). The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the knee. Arthritis Rheum. 29:1039–1049.
Benjuya N, Melzer, I, et.al. (2004). Aging-induced shifts from a reliance on sensory input to muscle co-contraction during balanced standing. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences, 59; 2, M166.
Tibor Hortoba, et. al. (2004). Aberrations in the Control of Quadriceps. Arthritis Care & Research. 51; 4, 562–569.
Fitzpatrick R, Mc Closkey D., et.al. (1994). Proprioceptive, visual and vestibular thresholds for the perception of sway during standing in humans. Journal of Physiotherapy. 478;1, 173-86.
Lord S R, Lloyd D G, et.al. (1996). Sensori-motor function, gait patterns and fall in community-dwelling women. Age Ageing. 25, 292-9.
Schot, Knutzen, Poole, et.al. (2003). Sit-to-Stand Performance of Older Adults following Strength Training Research Quarterly for Exercise and Sport. 74;1
Lord S, Ward JA, et.al. (1995). The effect of a 12-month exercise trial on balance, strength, and fall in older women: a randomised controlled trial. Journal of the American Geriatrics Society, 43;1198-1206.
Campbell A.J, Borrie M.J, et.al. (2010). Circumstances and consequences of fall experienced by a community population 70 years and over during a prospective study. Age and Ageing, 19;2,136-141.
Yusuke Maeda et al. (2011). A Preliminary study of static and dynamic standing balance and risk of falling in an independent elderly population with a particular focus on the limit of stability test. J.Physical.Therapy.Science. 23;803-806.
Odenheimer G, Funkenstein HH, et.al. (1994). Comparison of neurologic changes in ‘successfully aging’ persons vs. the total aging population. Archives of neurology. 51;573-580.
Perta von Heideken Wagert, Yngve Gustafson, et.al. (2009). Large variations in walking, standing up from a chair, and balance in women and men over 85 years: an observational study. Australian Journal of Physiotherapy; 55;39-45.
Wolfson C. Wentzel, et.al. (2001). Progression of impairment in patients with vascular cognitive impairment without dementia. Journal of Neurology. 28, 57;4, 714-716.
Podsiadlo D, Richardson S, et.al. (1991).The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 39;142–148.
Shumway-Cook A, Brauer S, et.al. (2000). Predicting the probability for fall in community-dwelling older adults using the Timed Up & Go Test. Phys Therapy. 80;896 –903.
Jones CJ, Rikli RE, et.al. (1999). A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. J Am Geriatric Soc. 70;2,113-9.
Robertson, Campbell, Gardner, et.al. (2002). Preventing Injuries in Older People by Preventing Fall: A Meta-Analysis of Individual-Level Data Journal of the American Geriatrics Society. 50;5, 905-911.
Rubenstein LZ, Josephson KR, et.al. (2002).The epidemiology of fall and syncope. In: Kenny RA, O’Shea D, eds. Fall and Syncope in Elderly Patients Clinics in Geriatric Medicine. Philadelphia: W. B. Saunders Co. 28, 513-518.
M. Province, Evan C. Hadley et al.(1995). The Effects of Exercise on Fall in Elderly PatientsA Preplanned Meta-analysis of the FICSIT Trials. JAMA. 273;17,1341-1347.
Campbell AJ, Robertson MC, Norton RN, et.al. (1999).Fall prevention over 2 years: a randomized controlled trial in women 80 years and older. Age and Ageing. 28,513-518.
Julie M. Chandler, Pamela W. Duncan, et.al. (1998). Is lower extremity strength gain associated with improvement in physical performance and disability in frail, community-dwelling elders. American Congress Of Rehabilitation Medicine And The American Academy Of Physical Medicine And Rehabilitation. 003-9993/98/7901-4303.
Joshua N. Farr, Scott B. Going, et.al. (2010). Progressive Resistance Training Improves Overall Physical Activity Levels in Patients With Early Osteoarthritis of the Knee: A Randomized Controlled Trial. J Physical Therapy. 90:356-366.
Cathy M Arnold, Robert A. Faulkner, et.al. (2010). The Effect of Aquatic Exercise and Education on Lowering Fall Risk in Older Adults With Hip Osteoarthritis Journal of Aging and Physical Activity, 18;245-260.
Marie-Louise Bird, Keith Hill, et.al. (2009). Effects of Resistance- and Flexibility-Exercise Interventions on Balance and Related Measures in Older Adults. Journal of Aging and Physical Activity, 17;444-454.
M. Van der esch, M. Steultjens, et.al. (2007). Joint proprioception, muscle strength, and functional ability in patients with osteoarthritis of the knee. American college of rheumatology. 57,5,787–793.
Julie C. Whitney, Stephen R. Lord, et.al. (2005). Streamlining assessment and intervention in a fall clinic using the Timed Up and Go Test and Physiological Profile Assessments. Age and Ageing. 34;567–571.
Robert Topp, Sandra Woolley, et.al. (2002). The effect of dynamic versus isometric resistance training on pain and functioning among adults with osteoarthritis of the knee. American Congress of Rehabilitation Medicine and the American Academy of Physical Medicine and Rehabilitation. 83;1187-95.
Campbell, A.J., Borrie, M.J., et.al. (1990). Circumstances and consequences of fall experienced by a community population 70 years and over during a prospective study. Age and Ageing. 19;2,136-141.
Moreland JD, Richardson JA, et.al. (2004). Muscle weakness and fall in older adults: a systematic review and meta-analysis. Journal of the American Geriatrics Society. 52,1121-1129.
Orr R, Raymond J, Fiatarone Singh M, et.al. (2008). Efficacy of progressive resistance training on balance performance in older adults: A systematic review of randomized controlled trials. Sports Med 38;317-343.
Latham N, Anderson C, Bennett D et al. (2003). Progressive resistance strength training for physical disability in older people. Cochrane Database Syst Rev. The Gerontolo Society of America. 2;33-36.
33. Foley A, Halbert J, et.al. (2003). Does hydrotherapy improve strength and physical function in patients with osteoarthritis: a randomised controlled trial comparing a gym based and a hydrotherapy based strengthening programme. Ann Rheum Dis; 62,1162–7.
Murphy MH, Nevill AM, et al. (2007). The effect of walking on fitness, fitness and resting blood pressure: A meta-analysis of randomized, controlled trials. Prev Med 44,377-385.
Ruth Defrin, Efrat Ariel, et.al. (2005).Segmental noxious versus innocuous electrical stimulation for chronic pain relief and the effect of fading sensation during treatment. Science, Direct., 115;1-2,152–160.
36. Michael V Hurley, David L Scott, et.al. (1997).Sensorimotor changes and functional performance in patients with knee osteoarthritis. Annals of the Rheumatic Diseases. 56;641-648.
Robertson MC, Campbell AJ, Gardner MM et al. (2002). Preventing injuries in older people by preventing fall: A meta-analysis of Individual-Level Data Journal of the American Geriatrics Society. May 50;5, 905-911.
Citation:
Kanchan A. Katre, Vijayakumar Pushparaj, Jibi Paul (2019). Effect of Otago Exercise Program (OEP) and Strength Training Program (STP) on leg strength and risk of fall among bilateral knee osteoarthritis patients, ijmaes, 5(1), 536-551.
2 Faculty of Physiotherapy, DR MGR Educational and Research Institute, Velappanchavadi, Chennai,India
Corresponding Author:
1MPT student, Faculty of Physiotherapy, DR MGR Educational and Research Institute, Velappanchavadi, Chennai, India.
Email: nicoluasnikky@gmail.com
ABSTRACT
Background of the study: Overweight and obesity are due to
abnormal or excessive fat accumulation which causes problems in health. Body
mass index (BMI) is a simple tool which is used for the classification of
overweight and obesity in adults. It is defined as a person’s weight in
kilograms divided by the square of his height in meters (kg/m2). The sole motto
of this study would be to compare the self-image on body shape among college
students and corporate sector employees.
Methodology: Subjects fitting into the inclusion criteria
were selected and screened for their BMI after obtaining a proper consent. They
were allocated into two groups, among which, one group with college students
and the other group with employees of corporate sector (White Collars). Study
Setting did at TCS, Chennai and Faculty of Physiotherapy, Dr. MGR. Educational
and Research Institute University, Velappanchavadi, Chennai. Subjects were
provided with a BSQ-34 questionnaire and asked to respond to each items. At the
end, final scores were arrived, which were analyzed & compared
statistically between the groups. Body Shape Questionnaire (BSQ)-34 score used
as Outcome measure to collect the data.
Result: The result of the study shows that there is a
considerable difference between the BSQ- 34scores of obese college students and
employees of corporate sector. Since the P value is <0.05, the difference is
significant.
Conclusion: The present study shows that there is a
significant difference between the self image of obese college students and
employees of corporate sector. The corporate sector employees being affected
more on self image of obesity.
Keywords: Self image on body shape, Obesity, corporate
sector, Body Shape Questionnaire
Received on 20thJanuary 2019,
Revised on 19th February 2019, Accepted on 28th February 2019
INTRODUCTION
Overweight and obesity are linked to cause more deaths
worldwide than underweight. Most of the world’s population live in developed
countries where overweight and obesity to kill more people than underweight
(this includes all high-income and most middleincome countries). Changes in
dietary and physical activity results in the environmental and societal changes
along with the development have role in obesity of people1, 2 .
Self image is the person’s own mental picture, generally of a
kind that is quite resistant to change, that depicts not only details that are
potentially available to objective investigation by others (height, weight,
hair color, gender, I.Q scores, etc…). Among women over 18 looking at
themselves in the mirror, research indicates that at least 80% are unhappy with
what they see in some studies up to 80% of women over- estimated their size 3,
4 .
Research confirms what most of us already know: that the main
focus of dissatisfaction for most men and women looking in the mirror is the
size and shape of their bodies, particularly their hips, waist and thighs.
Weightstigmatization is a common experience for obese subjects seeking weight
loss treatment; this is associated with poor psychological adjustment that may
hinder successful weightreduction. Long-term weight problems have an adverse
impact on self-esteem 5, 6 .
Aim of the study was to screen the self image with regards to
body shape in obese college student and employees of corporate sector. This
study has employed on self image in obese college students and obese corporate
sector employees. Self image gets affected due to obesity, which might be
characterized by stress, depression, and neglecting their own health. It is
prevalent among young women 7, 8, 9, 10 .
METHODOLOGY
This was an Observational study with Comparative design. 40
Subjects were included foe this study based on selection criteria. Convenient
sampling method used to collect the samples. Sample size: n=40 (college
students=20no’s, corporate employees=20no’s). The study conducted for 5 months.
Unmarried Women, College students aged 18 to 23 years and corporate employees
aged 25 to 30 years were Included for this study. Any surgeries, Diabetes
mellitus, Hypertension, Any treatment taking for obesity were excluded from
this study. Subjects fitting into the inclusion criteria were selected and
screened for their BMI after obtaining a proper consent. They were allocated
into two groups, among which, one group with college students and the other
group with employees of corporate sector (White Collars).
Study Setting did at TCS, Chennai and Faculty of Physiotherapy,
Dr. MGR. Educational and Research Institute University, Velappanchavadi,
Chennai. Subjects were provided with a BSQ-34 questionnaire and asked to
respond to each items. At the end, final scores were arrived, which were
analyzed & compared statistically between the groups. Body Shape
Questionnaire (BSQ)-34 score used as Outcome measure to collect the data 11, 12
. Procedure: After obtaining informed consents from subjects, they were divided
in two groups. One group was with college students and another group with
corporate employees. After a detailed explanation of questionnaire, which given
to the subjects they were asked to mark the Questionnaires form, later analyzed
statically to drive the conclusion.
Data analysis: The data obtained were tabulated and analyzed using descriptive and interferential statistical methods.
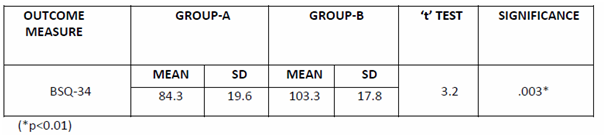
Table-1:
Comparison
of the bsq-34 scores between obese college students and employees of corporate
sector of self images.
The
above table reveals the mean, standard deviation (SD), t-test value of BSQ-34
scores. There is a significant difference between the Group-A and Group-B.
(*p<0.01)
RESULT
The result of the following study (BSQ-34) shows that there
is significant difference between GROUP-A (84.3) and GROUP-B (103.3) at P<0.01.
DISCUSSION
This is an observational study which aimed at
compare the self image in college student and employees of corporate sector
BSQ-34. The study shows that corporate sector employees have poor self image
when compared to college students. Self image is the mind set or opinion one
has about them. Which when affected considerably would result in behavioral
changes. One’s own physique (Obese/Lean/Moderate) would influence on self image
13, 14.
Research on the relationship between body
image and obesity is relatively new. Several areas await additional
investigation. Many obese individuals have body image concerns, but these
concerns are not universal. Furthermore, there appears to be little
relationship between the degree of obesity and the intensity of the
dissatisfaction. The nature of the obesity and its effect on body size and
shape may moderate the relationship with the degree of body image
dissatisfaction. Similarly, obesity-related co morbidities, such as
osteoarthritis, may contribute to body image dissatisfaction further15, 16.
Among obese women, body image dissatisfaction
appears to be related to lower self-esteem and increased symptoms of
depression. For most people, it does not appear to be related to clinically
significant depression. Furthermore, such body image dissatisfaction cannot be
equated with body image disturbance necessarily, which entails dissatisfaction
that also produces significant distress and psychosocial impairment 17, 18.
Weight control program as such have gained popularity among society but this very concept of self image is less concentrated. Hence, this study would fix this lag and thus make weight management therapies as holistic.
Limitation of the study: More Questionnaires and test may be used for better evaluation. Sample size may be increased for evaluation. Less women are working in non-cooperate sector; since obese women in corporate sector having stress and poor self image when compared to the obese women in college.
CONCLUSION
This study shows that there is significance
difference between college students and employees of corporate sectors
suffering from poor self image due to obesity. The BSQ-34 examination which was
conducted shows that the employees of corporate sector having poor self image
when compared to college students
REFERENCES
Annis NM, Cash TF, Hrabosky JI. (2004). Body image and psychosocial differences among stable average-weight, currently overweight, and formerly overweight women: the role of stigmatizing experiences. Body Image: An International Journal of Research;1:155–67.
Cash TF, Henry P. (1995). Women’s body images: the results of a national survey in the USA.; 33:19–28.
Elgar FJ, Roberts C, Tudor-Smith C, Moore L. (2005). Validity of self-reported height and weight and predictors of bias in adolescents. J Adolesc Health;37(5): 371-5.
Erickson SJ, Robinson TN, Haydel KF, Killen JD. (2000). Are overweight children unhappy? Body mass index, depressive symptoms, and overweight concerns in elementary school children. Arch Pediatr Adolesc Med;154: 931-5.
Flood V, Webb K, Lazarus R, Pang G. (2000). Use of self-report to monitor overweight and obesity in populations: some issues for consideration. Aust N Z J Public Health; 24: 96-9.
Feingold A, Mazzella R. (1998). Gender differences in body image are increasing. Psychol Sci; 9:190–5.
Foster GD, Wadden TA, Vogt RA. (1997). Body image before, during, and after weight loss treatment. Health Psychol;16:226-9.
Heatherton TF, Nichols P, Mahamedi F, et al. (1995). Body weight, dieting, and eating disorder symptoms among college students, 1982 to 1992. Am J Psychiatry; 152:1623-9.
Hill AJ, Williams J. (1998). Psychological heath in a nonclinical sample of obese women. Int J Obes; 22:578-83.
Matz PE, Foster GD, Faith MS, et al. (2002). Correlates of body image dissatisfaction among overweight women seeking weight loss. J Consult Clin Psychol; 70: 1040-4.
John U, Hanke M, Grothues J, Thyrian JR. (2006). Validity of overweight and obesity in a nation based on self-report versus measurement device data. Eur J ClinNutr; 60: 372-715.
Sarwer DB, Wadden TA, Foster GD. (1998). Assessment of body image dissatisfaction in obese women: specificity, severity and clinical significance. J Consult Clin Psychol; 66(4):651-4.
Stunkard AJ, Mendelson M. (1967). Obesity and body image: I. Characteristics of disturbances in the body image of some obese persons. Am J Psychiatry; 123:1296-300.
Schwartz MB, Brownell KD. Obesity and body image. Body Image: An International Journal of Research 2004; 1: 43–56.
Foster GD, Matz PE. (2003). Weight loss and changes in body image. In: Cash TF, Pruzinsky T,editors. Body image: a handbook of theory, research, and clinical practice. New York: Guilford Press; p. 405-13.
16. Sarwer DB, Thompson J K.(2002). Obesity and body image disturbance. In: Wadden TA Stunkard AJ, editors. Handbook of obesity treatment. New York: Guilford Press; p. 447-64.
17. Cash TF. (2002). A negative body image: evaluating epidemiological evidence. In: Cash TF, Pruzinsky T, editors. Body image: a handbook of theory, research, and clinical practice. New York: Guilford Press; p. 269-76.
18. McCabe MP, Ricciardelli LA. (2004). Weight and shape concerns of boys and men. In: Thompson JK, editor. Handbook of eating disorders and obesity. New York: Wiley; p. 606-34.
Citation:
D. Paul Nicoluas, Jibi Paul (2019). Comparative analysis of self image on body shape among obese college students and employees of corporate sector, ijmaes, 5(1), 531-535.
Authors: 1 Faculty of Physiotherapy, DR MGR Educational and Research Institute, Velappanchavadi, Chennai, India Corresponding Author: 1* Faculty of Physiotherapy, DR MGR Educational and Research Institute, Velappanchavadi, Chennai, India. Email: moorthympt@yahoo.co.in
ABSTRACT
Background of the study: Knee joint stiffness is one of the commonest complications in patients who had fractures in the femur and upper tibia. Stiffness, restrict range of motion of joint caused by soft tissue tightness and intra articular adhesions. The aim of study is to understand the effects of Muscle Energy Techniques on early knee joint mobilization to improve the range of motion by reducing post traumatic stiffness.
Methodology: A pretest-post test control group design was used for this study. Thirty patients from orthopedic physical therapy outpatient department of Sri Gokulam hospital, Salem were selected for this study and equally divided into two groups. Patients in group-A (Experimental) received wax therapy, static quadriceps exercise, active assisted mobilization and muscle energy techniques. Patients in group-B (control) who received wax therapy, static quadriceps exercise and active assisted knee mobilization. Pain was measured by Visual Analogue Scale, Range of motion by Universal Goniometer and muscle strength by Manual Muscle Testing.
Result: The mean post test values for group A and group B are 2.2 and 4.4 for Pain, 103 and 78 for Active Knee Flexion, 7.7 and 6.2 for Quadriceps strength respectively.
Conclusion: The study concluded that Muscle Energy Technique is more effective in improving range of motion, strength of quadriceps muscles and reducing pain in knee joint.
Keywords: Knee joint stiffness, Visual Analogue Scale, Range of motion, Goniometer, Manual Muscle Testing, Muscle Energy Technique
Received on 11th January 2019, Revised on 15th February 2019, Accepted on 27th February 2019
INTRODUCTION
Knee joint stiffness is one of the commonest complications in patients who have fractures in the femur and upper tibia finding difficulty in locomotion. Stiffness or restricted range of motion of a joint caused by both soft tissue tightness and intra articular adhesions 1 . Previously the stiffness due to muscle spasm treated with hot packs and active mobilization techniques. Currently muscle energy techniques have implemented along with routine had better prognosis. Soft tissue tightness caused by painful spasm that result in decreased mobility and desire to move the joint affecting normal range of motion to the joint 2 . Most of the joint restriction is the result of muscular shortening and tightness. Shortening of muscles due to spasm seems to be a self perpetuating phenomenon which results from an overreaction of the gamma neuron system3. Muscle energy techniques is one such approach which targets the soft tissues primarily although it also makes a major contribution towards joint mobilization, muscle energy techniques otherwise called active muscular relaxation techniques 4, 5 .
The main purpose of this study is how far the muscle energy techniques are effective in normalizing muscle spasm and improving strength and keep the normal range of motion compared with the other routine treatment for joint stiffness. Objectives: To study the effectiveness of standard treatments for post operative knee stiffness, to study the effectiveness of standard treatments with muscle energy techniques for post operative knee joint stiffness and also to compare the effects between standard treatment and standard treatment along with muscle energy techniques to find out the significance of muscle energy techniques.
MATERIALS AND METHODOLOGY
Design: A pretest, post test control group design was used for this study. Sampling method: Thirty patients attending the orthopedic physical therapy outpatient department of Sri Gokulam hospitals were selected for this study that had consideration of the following criteria. Inclusion criteria: Irrespective of gender aged between 20-50 years, patients referred by an orthopaedic surgeon for physiotherapy those who had fractures at femoral shaft and upper tibia. Fracture shaft of femur managed surgically by an open reduction with closed interlocking nailing, plate and screw fixation.
Fracture at intercondylar region of tibia managed by an open reduction with plate and screw fixation. Exclusion criteria: Arthritis at knee joint (OA and RA), Osteoporosis (brittle bone disease), Bone infections(osteomyelitis), Osteochondritis dissicans (loose bodies), Traumatic effusion, Bone tumors, Fractures with closed reductions, Chondromalacia patella, Traumatic synovitis, Un co-operative psychiatric patients were excluded from the study. Sample allocation: Informed consent was obtained from subjects meeting inclusion criteria were divided into two groups A and B with fifteen patients in each group, based on odd even allocation. Patients in group-A (Experimental) received wax therapy, static quadriceps exercise, active assisted mobilization and muscle energy techniques.
Patients in group-B (control) who received only wax therapy and static quadriceps exercise and active assisted knee mobilization. Materials: Wax bath unit, temperature controlled by automatic thermostat maintaining optimum temperature of 42–44 degree Celsius. Goniometer plastic half circle (180 degree) used to measure both active knee flexion range of motion. Outcome parameters: Pain measured by visual analogue scale, which was popularized by Huskisson in the 1970 s, consist of a straight line, 10cm ling, that represents the range of pain to be rated. The scale on one end marked 0 represents “no pain” the other end marked 10 represents “severe pain” the patients were asked to mark on the scale according to the amount of pain perceived. Range of motion by a Universal Goniometer plastic half circle (180 degree) used to measure active knee flexion range of motion. Muscle strength by manual muscle testing was developed by Wright and Lovett in 1912 as a means of testing and grading muscle strength based on gravity and manually applied resistance. Generally the patient is positioned so that the muscle or muscle group being tested has to hold or move against the resistance of gravity. If this is well tolerated, the examiner applies manual resistance gradually to the distal end of the body part in which the muscle inserts, and in a direction opposite to the torque produced by muscle or muscle groups. Kendall et.al., suggest to measuring manual muscle testing grades from a 0 to 10 scale 6, 7 .
Measurement tools: Visual analogue scale, Goniometer plastic half circle(180 degree), Manual muscle testing grading. Procedure: Patients in each group underwent an initial evaluation procedure and the following measurements were done.
Measurement of pain: Baseline measurement of pain was taken using visual analogue scale and subsequent measurements were taken on the fourth and seventh day after therapy.
Measurement of knee range of motion: The available active knee flexion range of motion was measured initially and subsequent measurements were taken on fourth and seventh day after therapy. Knee motions both active flexion measured by positioning the patient in prone lying and the femur was stabilized to prevent rotation abduction and adduction at the hip.
Fulcrum of the Goniometer placed over the lateral condyle of the femur, stable arm over the lateral midline of the femur and moveable arm over the lateral midline of the fibula using the lateral malleolus and fibular head for reference 10, 11 .
Measurement of strength: The initial strength of both quadriceps and hamstrings was measured on day one and subsequent measurement was taken on day four and seven after treatment by using manual muscle testing grades described by “kendall et.al.,” 0 to 10 scale.
Intervention:
Muscle Energy Techniques (MET): MET methods all employ variations on a basic theme. This primarily involves the use of the patients own muscular efforts in one of the number of ways usually in association with the efforts of the therapist. The operator force may exactly match the effort of the patient (so producing an isometric contraction) allowing no movement to occur and producing as a result a physiological neurological response (via the Golgi tendon organs) involving a combination of Reciprocal inhibition of the antagonists of the muscles being contracted. Types of muscle energy Post isometric relaxation:
The patient is positioned in prone lying and the therapist standing at the side of the couch the patient knee is flexed until the initial barrier or resistance palpated, the operator hand is placed on the ankle the patient is instructed “press your leg gentoly against my hand”. This contraction is held for a full three to five seconds. Direct the patient to relax, simultaneously ceasing your counter force, wait two seconds for the tissue to relax, then further flex the knee until a new restriction barrier is met. This maneuver is repeated three to five times 8 .
Reciprocal inhibition: The patient is positioned in prone lying and operator standing at the side of the couch hold one hand at the ankle behind ask the patient to press the ankle against the operator hand maintain the contraction for a full period of 3 to 5 seconds. Then direct the patient to relax simultaneously ceasing your counter force, waiting for 2 seconds to relax the tissues then further flex the knee until a new barrier is met again this maneuver repeated for three to five times 9 .
Wax bath: The most widely used method of application for the extremity joints is “dip and wrap” method. The nature of wax treatment is explained and area to be treated is checked for contraindications the temperature of the wax also checked the treatment part is washed and thoroughly dried to prevent water being introduced in the wax bath. A patient is positioned to be able to wrap the part in wax in a convenient and comfortable way. The bandages of suitable size and mesh can be soaked in hot wax and then wrapped around the joint; the additional wax can then be brushed over the bandages. There are six to twelve wrappings used alternatively 12, 13 .
Static isometric exercise for the knee: Three methods which may be used to obtain this contraction. The contraction is taught on the unaffected leg and is seen and felt by the patient who then attempts a similar contraction on the other side. In lying one hand gives compression on the sole of the foot and resists plantar flexion strongly while the other hand placed under the knee joint. The therapist put one hand on the muscles and the other under the patients heel the patient is then asked to feel the pressure and attempt to relive it by lifting the leg. No movement takes place but the muscles are thrown into a state of strong contraction. Active Assisted Knee Mobilization: Active assisted knee mobilization performed either the assistance given by the therapist or by the patient himself. Position the patient in supine lying, instructs the patient to initiate the motion by lifting up the involved knee with the normal foot. Another method is to position the patient in high sitting, asks the patient to bend his knee maximum the effort of the patient can be assisted by the therapist or by the patients opposite leg.
Fig.3 Subject receiving wax bath treatment
RESULT
Independent t test is used to comparing Post Test Vas Values Of Group A and Group B. On day 4 the post test VAS value of group A is 4.6 and group B is 5.8. the calculated t value is (10.18) is greater than the table value (t=2.048) at 5% level of significance for two-tailed test, showing that there is a significant difference between two groups, reject the null hypothesis. On day 7 the mean post test VAS value of group A is 2.2 and group B is 4.4. the calculated t value is (11.66) is greater than the table value (t=2.048) at 5% level of significance for twotailed test, showing that there is a significant difference between the two groups, reject the null hypothesis 14, 15 .
Dependent t test is used to comparing initial, day 4 and day7 vas values of Group A. The mean pre test VAS value is 6.8 and post test values are 2.2 and 4.6. Calculated t values are (20.9) & (35.88) is greater than the table value (t=2.145) at 5% level of significance for twotailed test, showing that there is a significant difference between the values. Dependent t test is used to comparing initial, day 4 and day 7 vas values within the Group B. The mean pre test VAS value is 6.9 and post test values are 1.1 and 2.5. Calculated t values are (16.5) & (19.5) is greater than the table value (t =2.145) at 5% level of significance for two-tailed test, showing that there is a significant difference between the values.
Independent t test is used to comparing post test active knee flexion values of Group-A and Group-B. On day 4 post test mean active knee flexion of group-A is 78 and group-B is 63.3. Calculated t value (4.831) is greater than the table value (t=2.048) at 5% level of significance for two-tailed test, showing that there is asignificant difference between two groups reject the null hypothesis. On day 7 post test mean active knee flexion of group-A is 103 and group-B is 78. Calculated t value (8.515) is greater than the table value (t=2.048) at 5% level of significance for two-tailed test showing that there is a significant difference between two groups reject the null hypothesis. Dependent t test is used compare initial, day 4 and day 7 values of Group-A. The mean pre test active knee flexion value is 56.3 and post test values are 21.7 and 46.7. Calculated t values are (16.15) & (27.2) is greater than the table value (t=2.145) at 5% level of significance for two-tailed test, showing that there is a significant difference between the values.
Dependent t test is used to comparing initial, day 4 and day 7 values of Group-B. The mean pre test active knee flexion value is 50.3 and post test values are 13.3 and 27.7.Calculated t values are (11.4) & (18.045) is greater than the table value (t=2.145) at 5% level of significance for two-tailed test, showing that there is a significant difference between the values. Independent t test is comparing post test quadriceps strength values of Group-A and Group-B. On day 4 post test mean of quadriceps strength of group-A is 5.8 and group-B is 4.9. Calculated t value (16.11) is greater than the table value (t=2.048) at 5% leve of significance for two-tailed test, showing that there is a significant difference between two groups reject the null hypothesis. On day 7 post test mean of quadriceps strength of group-A is 7.7 and group-B is 6.2. Calculated t value (6.0) is greater than the table value (t=2.048) at 5% level of significance for twotailed test, showing that there is a significant difference between two groups.
Dependent t test is used to compare initial, day 4 and day 7 values of Group-A. The mean pre test quadriceps strength value is 3.9 and post test values are 1.9 and 3.8. Calculated t values are (12.35) & (20.6) is greater than the table value (t=2.145) at 5% level of significance for two-tailed test, showing that there is a significant difference between the values. Dependent t test is used to compare initial, day 4 and day 7 values of Group-B. The mean pre test quadriceps strength value is 3.7 and post test values are 1.2 and 2.5. Calculated t values are (14.3) & (19.5) greater than the table value (t=2.145) at 5% level of significance for twotailed test, showing that there is a significant difference between the values.
Independent t test used to compare post test hamstring strength values of Group-A and Group-B. On day 4 post test mean of hamstring strength of group-A is 6.3 and group-B is 5.2.Calculated t value (5.714) is greater than the table value (t=2.048) at 5% level of significance for two-tailed test, showing that there is a significant difference between the two groups reject the null hypothesis.
On day 7 post test mean of hamstring strength of groupA is 8 and group-B is 6.4, Calculated t value (t=7.222) is greater than the table value (t=2.048) at 5% level of significance for twotailed test, showing that there is a significant difference between two groups. Dependent t test is used to comparing initial, day 4 and day 7 values of Group-A.the mean pre test hamstring strength value is 4.3 and post test mean values are 2 and 3.7. calculated t values are (26.0) & (24.45) greater than the table value (t=2.145) at 5% level of significance for two-tailed test, showing that there is a significant difference between the values.
Dependent t test is used to compare initial, day 4 and day 7 values of Group-B. The mean pre test hamstring strength value is 4 and post test values are 1.2 and 2.4. Calculated t values are (11.7) & (18.72) greater than the table value (t=2.145) at 5% level of significance for twotailed test, showing that there is a significance between the values.
DISCUSSION
Analysis of mean change in pain, active knee flexion and mean strength changes of both quadriceps and hamstrings revealed that there is significant difference between group-A who received muscle energy technique, wax bath, static quadriceps exercises and active assisted mobilization exercises, when compared with the group-B who received wax bath, static quadriceps exercises and active assisted mobilization exercises. Results obtained after analysis shows that there is decrease in pain score and increase active knee flexion, increase muscle strength respectively, which is statistically significant in post operative fracture stiffness patients who received muscle energy techniques when compared with the control group at the end of day 4 and day 7.
This permits rejection of null hypothesis. Analysis of results between pretest and post test values of experimental group shows that there is improvement in pain score, active knee flexion, and quadriceps, hamstrings strength following muscle energy techniques at the end of day 4 and day 7. Analysis of results between pretest and post test values of control group shows that there is significant improvement in pain score, active knee flexion and muscle strength following standard treatment at the end of day4 and day7. Hence the post analysis of results shows the superiority of muscle energy techniques along with standard treatment to reduce pain and increase range of motion and muscle strength. The better result in experimental group could be due to the muscle energy techniques decrease muscular spasm, reduce muscular shortening, prevents inter fiber adhesions influences the greater reduction of pain, increase range of motion, isometric exercise nature of this technique at various angle of restriction increase strength throughout the range of motion 16, 17.
Reason for decrease of pain and increase of range of motion, strength of muscle by muscle energy techniques: The most important causative factor for limiting joint range of motion after an injury is muscular shortening due to muscle spasm (Bourdilon, 1982).The restriction which takes place as a result of tight, shortened muscles usually accompanied by some degree of lengthening and weakness of antagonist, muscle energy technique targets these muscle tissues to promote relaxation, increase circulation, affecting Gamma motor neuron system in order to reduce pain and spasm 18.
In muscle energy technique a combination of both Post isometric relaxation and Reciprocal inhibition can effectively be employed to lengthen the shortened tissues and to strengthen the weak overlong muscles. When a muscle is isometrically contracted its antagonist will be inhibited and relaxed, similarly the agonist or shortened muscle also inhibited to achieve a degree of ease and additional movement of the shortened tissue 19 .
CONCLUSION
The study concluded that the standard treatment and standard treatment along with muscle energy technique both have an effect to reduce pain, increase range of motion, and strength of muscle after post immobilization fracture stiffness. The study also concluded that the Muscle energy technique was producing greater improvement in gaining range of motion and strength of muscles than other standard treatments.
REFERENCES
J.Maheshwari, (1997). Essential Orthopaedics, 2nd revised edition, interprint, New delhi.
Leon chaitow, et al. (2006). Muscle energy techniques Churchil Livingston, Singapore publishers (Pvt) Ltd.
Carolyn kishner, Lymn Allen golby, Therapeutic exercise, 3rd edition, Jaypee brothers New delhi. (1996)
M.Natarajan, N.Mayilvahanan, (1994). Orthopaedics and Traumatology, 4th edition, published by M.N. Orthopaedic hospital.
Jayant joshi and Prakash kotwal (1999). Essential of orthopaedics and applied physiotherapy B.I.Publications New delhi.
Susan.B.O’Sullivan (2001). Physical rehabilitation assessment and treatment, Jaypee brothers 4th edition, New delhi.
David J. Magee (1997). Orthopaedic physical therapy assessment, 4th edition C.V.Mosby, Company, philadelphia.
M.Dena gardener, (1985). Principles of exercise therapy, 4th edition, CBS publishers & distributors, New delhi.
Leon chaitow (1993). Integrated neuromuscular inhibition techniques in the treatment of pain and trigger points.
Cynthia C.Norkin, (2001). Joint structure and function, 3rd edition, Jaypee brothers New delhi.
Cynthia C.Norkin, (1998). Measurement of joint range of motion, Jaypee brothers New delhi.
John low, Ann Reed (1990). Electrotherapy explained, 3rd edition, ButterworthHeinmann, Oxford.
Barbara J. Behrens, Physical agents, (1959). F. A. Davis company Philadelphia; 45.
Kothari C.R., (2004). Research methodology, 2nd edition, new age international (pvt) ltd. New delhi.
P.S.Sundar Rao and J.Richard, (2004). An introduction to biostatistics, 3rd edition, Prentice hall of India, New delhi.
Lewit.K, Simons D.G., (1984). Myofascial pain; relief by post isometric relaxation, Archieves physical medicine and rehabilitation.
Lewit.K, (1985). Muscular and articular factors in movement restriction, manual medicine.
Liebenson C (1989). Active muscular relaxation techniques, journal of manipulative and physiological therapeutics.
Lewit. K. (1986). Post isometric relaxation in combination with other methods of muscular facilitation and inhibition in manual medicine.
Citation:
Moorthy A, Jibi Paul, G Muthuraj (2019). Effects of muscle energy techniques on knee joint mobilization in an early stage following fracture shaft of femur and upper tibia , ijmaes, 5(1), 518-525.
2 Asst. Professor, Tamilnadu Physical Education and Sports University, Chennai, Tamilnadu, India. 3 Research scholar, Tamilnadu Physical Education and Sports University,Chennai, Tamilnadu, India. 4 Associate Professor, School of Physiotherapy, Vels Institute of Science & Technology, Chennai, Tamilnadu, India.
Corresponding Author:
1Research scholar, Tamilnadu Physical Education and Sports University , Chennai, Tamilnadu, India, Mail id: rraaddss@yahoo.com
ABSTRACT
Purpose: The purpose of this study was to find out the effectiveness of Dynamic Core Stability Exercises and stretching in improving the flexibility of overweight persons who lack flexibility.
Methods: Fifteen (N=15) overweight middle aged male subjects who had not been into regular exercising and lack flexibility were selected based on the BMI who scored more than 25. All were basically screened out for their lifestyle and work related factors. All the samples were put into flexibility test by using modified sit and reach test. All had received dynamic core stability exercises and stretching of hamstring muscles and the outcome measure was measured using manual muscle testing and modified sit and reach test.
Results: The outcome measures of muscle power assessed using manual muscle testing (MMT) method 0-5 grading scale system. The mean value of Pre test MMT score is 3.7 and that of the post test mean value is 4.4 which shows a significant improvement (P<0.0001).The flexibility was measured using modified sit and reach test and its mean pre test value is 9.3 and that of the post test value is 12.3 which shows a highly significant improvement in the flexibility (P<0.0001).
Conclusion: This study showed that person who was identified as overweight based on BMI, were found to be lacking of their body flexibility mainly of back muscles and hamstring muscles. It is concluded that Dynamic core stability exercises and stretching was found to be useful in improving the muscle strength and flexibility.
Keywords: Overweight, BMI, Lack of Flexibility, Dynamic Core Stability Exercises, Stretching, Modified Sit and Reach Test
1 Physiotherapy Department, School of Health Sciences, KPJ Healthcare University College, 71800 Nilai, Negeri Sembilan, Malaysia.
Corresponding Author:
1* Physiotherapy Department, School of Health Sciences, KPJ Healthcare University College, 71800 Nilai, Negeri Sembilan, Malaysia.Email: izham@kpjuc.edu.my
ABSTRACT
Background and objectives: Smartphone is ubiquitous in this digital era and the remarkably evolved of technologies is an evident of heavy usage of such gadget in daily life. Recent evidence indicate that there is significant association between upper arm discomfort and smart phone user. However, there is limited finding on the smart phone addiction on upper body discomfort. Therefore, this study aimed to investigate level of smartphone addiction among Kuala Lumpur young adults.
Methods: This is a cross sectional analytical type of study. Self-administer questionnaire is used to determine the level of smartphone addiction level and body discomfort.
Results: A total of 290 subjects (80.7% females and 19.3% males) are involve in this study. Majority of respondents (69.7%) suffer mild smartphone addiction and there is significant association with neck and shoulder discomfort (p<0.05). Respondent’s belief that the discomfort experience were due to prolonged smartphone usage (74.1%). Furthermore, 84.5% of respondents noted that discomfort experienced was relieved when not using smartphone. There is significant differences between between time spent on smartphone with age categories, gender, occupation and smartphone addiction level (p<0.05).
Conclusion: Time spent on smartphone is consistent to smartphone addiction level. A higher level of smartphone addiction will increase the risk in developing upper body discomfort.
Keywords: Smartphone Addiction, upper body, Young Adults.