James Wilson HasoloanManik1, KiranaWardhani2, Adinda Amira Putri3, JeremiaBernardito4, Abi Wiranata5, Alberta YatiWulang6, Lucky Anggiat7
Corresponding Author:
7Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
Email: lucky.panjaitan@uki.ac.id
Authors:
1Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
2-6 Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
| ABSTRACT |
Background: Physiotherapists, as health care professionals, also have a role in providing main services in primary health care facilities. The practice of physiotherapy in the clinic can be done independently, or in collaboration or integrated with other health care professionals. Physiotherapy services with direct access will facilitate the patients to get physiotherapy services. This study aimed to observe one of physiotherapy service model with direct access in Indonesia.
Methods: This research is observational study and observed a clinic that provides direct access to the physiotherapy without having to go through a doctor or other health care professionals. The clinic being observed is the NT Clinic, which is an integrated clinic between general practitioners, medical specialists, and dentists.
Results: In a one-year service from January-December 2021, physiotherapists have handled 1,184 patient visits. The direct access to physiotherapy services at NT Clinic mostly treat patients with musculoskeletal conditions. Physiotherapists at NT Clinic also prioritize manual therapy with types of massage, joint mobilization, and stretching. Then intervention using ultrasound is also the most frequently used intervention and is followed by exercise therapy.
Conclusion.Physiotherapy services at NT Clinic are easy to reach by patients and are supported by medical specialists who can collaborate to provide optimal service to patients. Cases handled by physiotherapists at NT Clinic are musculoskeletal and neuromuscular. With direct access, physiotherapists can provide optimal services for patients based on the patient’s age, case, and appropriate intervention. Furthermore, physiotherapists can also provide referral options and receive referrals from medical specialists if needed.
Keywords: Physiotherapy, Direct Access, Primary Health Care, Clinic.
| Received on 4thFebruary 2022, Revised on 19thFebruary 2022, Accepted on 26thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.006 |
INTRODUCTION
Indonesia provides various health services, such as independent practice, community health centers, clinics, and hospitals1. Health services must include health promotion, preventive, curative, and rehabilitative. Health services consist of health care professionals who can work independently or in collaboration. Community health centers, clinics, and hospitals are health services with a collaborative work system. Clinical services are categorized into primary service facilities which are the foremost health services2.
According to the Regulation of the Minister of Health of the Republic of Indonesia Number 9 of 2014, a clinic is a health service facility that arranges individual health services and provides medical services or specialist3. Health service facility is a tool and/or place used to organize health service efforts, whether health promotion, preventive, curative or rehabilitative carried out by the government, local government, and/or the community. Physiotherapists, as health care professionals, also have a role in providing main services in primary health care facilities4.
Physiotherapy services are included to health services that provided to patients in terms of develop the body movement functions which include improvement, maintenance, and recovery using modalities such as exercise therapy, electrical modalities, and others5,6. In physiotherapy services, there are some patients with various disorders such as musculoskeletal (orthopedic or sports injuries), neuromuscular (neurological disorders), pediatrics (child development, neurology), cardiovascular and respiratory, integumentary and women’s health (SPA, beauty care)7. Physiotherapy services are also found in health centers, general hospitals, specialist hospitals and/or independent practice2,8.
The practice of physiotherapy in the clinic can be done independently, or in collaboration or integrated with other health care professionals such as medical specialists and pharmacy services8.
Physiotherapy services focus on patients through flow that can be accessed directly or through referrals from other health care professionals or fellow physiotherapists. Referrals for physiotherapy to other health care facilities/hospitals are made if the patient/client refuses physiotherapy services, requires further examination, or requires other interventions that are not available at the clinic2,9.
Physiotherapy services with direct access will facilitate the patients to get physiotherapy services. This solution was initiated by the Indonesian government4,7. In line with this regulation, the World Physiotherapy organization also states that physiotherapist can work an important role in direct health promotion, preventive, curative and rehabilitative activities10.
Several countries also already implemented similar rules so that the public’s health status can be improved properly with direct access to physiotherapy services11–13.
This study aimed to observe one of physiotherapy service model with direct access in Indonesia. The results of this study are indispensable as initial research because of the absence of research data on direct access to physiotherapy in Indonesia. This research was conducted at a clinic in North Jakarta, Indonesia which is integrated with the services of general practitioners, medical specialists, dentists and physiotherapist. In addition, the results of this study can be used as a reference for physiotherapists to build direct access physiotherapy services that integratedwith other health care professionals in primary health care service clinic.
METHODOLOGY
This research is observational study and observed a clinic that provides direct access to the physiotherapy without having to go through a doctor or other health care professionals. The clinic being observed is the NT Clinic, which is an integrated clinic between general practitioners, medical specialists, and dentists. The clinic provided us access to information related to direct access to physiotherapy services and a brief profile of the clinic.
The first information was the clinic profile, which is the vision and mission of the NT Clinic. Then, we continued to collect information on the flow of direct access physiotherapy services in the form of tables and descriptions. Next, we collected the data of active physiotherapists, physiotherapists’ level of education, and the availability of existing modalities and facilities.
The next data was the demographics of active patients that cover the number of patients who come directly to the physiotherapist both referrals and independent arrivals, age range, gender. The last data was the classification of cases handled by physiotherapists, some details of cases that are often found, and interventions carried out by physiotherapist. All data were processed using Microsoft Excel and presented in the form of tables and graphs.
RESULTS AND DISCUSSION
NT Clinic Profile: The vision of NT Clinic is to become a health clinic that is trusted by the community and its mission is to provide the best, affordable, and quality health services. The NT Clinic is a primary health care clinic led by a neurologist. Other services available are pediatricians, obstetricians, internal medicine specialists, neurologists, dentists, and physiotherapists. In addition, NT Clinic also hires nurses to help the health services run properly. Even though NT Clinic is led by a neurologist, all services provided by them can be accessed by patients directly based on the patient’s preference without having to go to the doctor, including physiotherapy.
Physiotherapy Direct Access Service Flow: The flow of physiotherapy services at NT Clinic as an outpatient clinic is in accordance with the Regulation of the Minister of Health of the Republic of Indonesia year 2015 Number 654. The service flow starts from registration via the website, telephone/WhatsApp, or face to face. Patients can come with a referral from a doctor or independently. New patients must register at the receptionist by providing an identity card. If the patient uses insurance, the insurance card must be given to the receptionist. The receptionist will fill in the patient identity section on the “Physiotherapy Patient Status Card”.
After registering, the receptionist will fill in patient data and tell the patient to go to the physiotherapy service. Furthermore, the physiotherapist will conduct an assessment to determine the appropriate physiotherapy intervention based on the diagnosis. If there is no indication to get physiotherapy services, the patient will be referred back to the referrer or the appropriate health care professionals (general or medical specialist) or after undergoing a series of physiotherapy processes. After receiving the therapeutic procedure, the patient returns to the receptionist to complete the administration.
Physiotherapy Service Profile: Physiotherapists who work in direct access physiotherapy services consist of 3 physiotherapists.
Led by a physiotherapist with a master’s degree with 2 physiotherapists who become general physiotherapists with diploma education. The availability of modalities is also quite complete. All profiles are presented in the following table1.
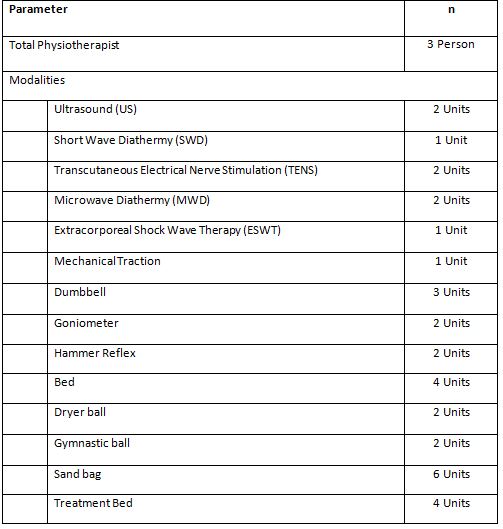
It can be seen in the table 1 physiotherapists are supported with various modalities. As well as several exercise therapy tools and treatment beds that support the best interventions for patients (Figure 1).

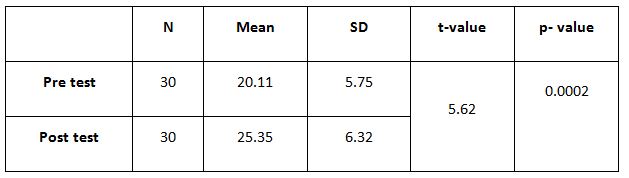
In a one-year service from January-December 2021, physiotherapists have handled 1,184 patient visits. Detailed demographic data on the number of patients per month can be seen in table 2.
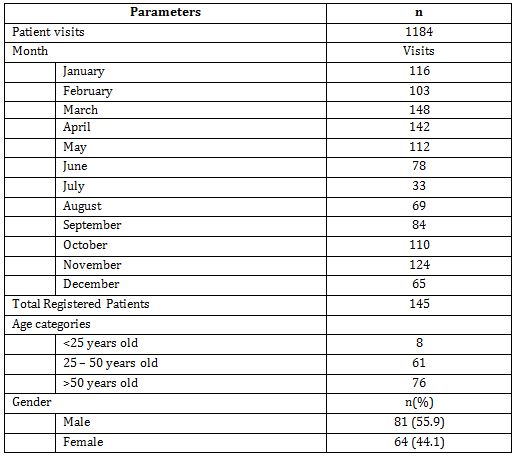
From the data, we can see that patients are quite high, indicating that patients are disciplined to take part in the physiotherapy program. Seen in June and July, there was a decrease in the number of patients to below 80 people in 1 month due to the second wave of COVID-19 in Indonesia. With a total of 145 patients registered in 1 year, it is also seen that active patients are dominated by patients over 50 years of age with mostly male (55.9%).
The next data is the classification of cases handled with detailed case diagnosis for the 10 most cases. In addition, the data related to the use of physiotherapy interventions were also presented for each patient who came to physiotherapist.
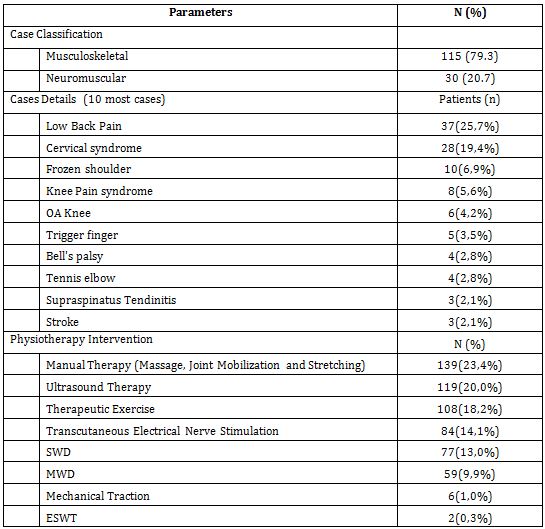
From the data in table 3, it can be seen that the direct access to physiotherapy services at NT Clinic mostly treat patients with musculoskeletal conditions, but there is also a large proportion of neuromuscular disorders both centrally and peripherally. This is also in line with research conducted by Demont et al. (2021) that it is true that physiotherapists in primary care have more patients with musculoskeletal conditions14. Physiotherapists will work an important role in reducing musculoskeletal disorders in the community through primary health services. Physiotherapists will be more efficient in treating patients. In fact, it was further explained that it would be able to improve the quality of life of patients, reduce disability in the community, and reduce the cost of health services. With direct access, patients can immediately go to a physiotherapist and get the right treatment, without having to spend time seeing a medical specialist15,16. Moreover, other studies have also concluded that patients with musculoskeletal conditions get better results and require less other services to improve their health conditions1715. However, taking into account the condition of the patient’s case, which may require a referral to a medical specialist, both at the beginning of the examination and after therapy9,12,14.
Physiotherapists at NT Clinic also prioritize manual therapy with types of massage, joint mobilization, and stretching. Then intervention using ultrasound is also the most frequently used intervention and is followed by exercise therapy. Research by Anggiat et al. also shows that physiotherapists use manual therapy more than other modalities18. However, exercise therapy is also the most popular intervention and is very often used in direct access physiotherapy practice8,19. From the intervention, the physiotherapists can use manual therapy and exercise to be the main intervention, supported by various modalities such as ultrasound and electrical stimulation. Diathermy interventions in several studies have been abandoned because of their high cost and low effectiveness compared to manual therapy and exercise20,21. However, interventions based on electro physical agents still dominate in Asia.
This study is an initial study that only made observations in one clinic. In the future, larger studies are needed and involve many clinics or health care services that provide direct access to physiotherapy.
CONCLUSION
NT Clinic is a primary health care clinic that integrates physiotherapy, medical specialist, and support direct access to physiotherapy services. Thus, physiotherapy services at NT Clinic are easy to reach by patients and are supported by medical specialists who can collaborate to provide optimal service to patients.
NT Clinic’s physiotherapy patients are dominated by patients over 50 years of age. Cases handled by physiotherapists at NT Clinic are musculoskeletal and neuromuscular such as low back pain, cervical syndrome, frozen shoulder, knee syndrome, and knee OA. The most frequently used physiotherapy modalities are manual therapy, US, exercise therapy, TENS, and MWD. With direct access, physiotherapists can provide optimal services for patients based on the patient’s age, case, and appropriate intervention. Furthermore, physiotherapists can also provide referral options and receive referrals from medical specialists if needed.
As a recommendation, the current physiotherapy service system at NT Clinic can be an example for colleagues to provide direct access physiotherapy services. With the intervention of manual therapy, exercise therapy, and ultrasound, the physiotherapist is sufficient to provide optimal services supported by other facilities such as bed treatment and exercise equipment.
Acknowledgements: The researcher would like to thank Kirana Wardhani, Adinda Amira Putri, JeremiaBernardito, Abi Wiranata, Alberta YatiWulang, and all NT Clinic’s physiotherapists for collecting and providing the data.
Conflict of interest: The author has no conflict of interest to declare.
Funding of study; This study was self-funded study
Compliance with Ethics: This study does not provide intervention and endangers the respondents so that it does not use ethical studies. However, data collection in this study was carried out with the acceptance of the university with reference no. 351/UKI.F8.PF/PP.5.1/2021 and permission from the clinic.
REFERENCES
1. Kementerian Kesehatan Republik Indonesia. Peraturan Pemerintah No. 47 Tahun 2016 Tentang Fasilitas Pelayanan Kesehatan.; 2016:1-16.
2. Holdsworth LK, Webster VS. Direct access to physiotherapy in primary care: Now? – And into the future? Physiotherapy. 2004; 90(2):64-72.
3. Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia no.9 Tahun 2014 tentang Klinik. Republik Indones. 2014;9:1-16.
4. Kemenkes RI. Peraturan Menteri Kesehatan Republik Indonesia Nomor 65 Tahun 2015 Tentang Standar Pelayanan Fisioterapi. Menteri Kesehat Republik Indones. 2015;16(2):39-55.
5. Manurung NSA. Manajemen Proses Fisioterapi Pada Satu Rumah Sakit Swasta Di Jakarta Timur. J Ilm Fisioter. 2020; 20(2):54-63.
6. World Confederation for Physical Therapy. Guideline for standards of physical therapy practice. Published online 2011:1-19. https://world.physio/sites/default/files/2020-07/G-2011-Standards-practice.pdf
7. Kemenkes RI. Peraturan Menteri Kesehatan No.80 Tahun, 2013;(1536):1-13.
8. Manurung NAS, Anggiat L. Entrepreneurship Models in Physiotherapy Practice: an Observational Study. Int J Med Exerc Sci. 2021;7(3):1088-1095.
9. Deyle GD. Direct Acces Physical Therapy and Diagnostic Responsibility: The Risk-to-Benefit Ratio. J Orthop Sport Phys Ther. 2006; 36(9): 632-634.
10. World Confederation for Physical Therapy. Direct access and patient/client self-referral to physical therapy: Policy Statement. Published online 2019.
11. Leemrijse CJ, Swinkels ICS, Veenhof C. Direct access to physical therapy in the Netherlands: Results from the first year in community-based physical therapy. Phys Ther. 2008;88(8):936-946.
12. Praestegaard J, Gard G, Glasdam S. Practicing physiotherapy in Danish private practice: An ethical perspective. Med Heal Care Philos. 2013; 16(3):555-564.
13. Bury TJ, Stokes EK. Direct access and patient/client self-referral to physiotherapy :A review of contemporary practice within the European Union. Physiother (United Kingdom). 2013; 99(4): 285-291.
14. Demont A, Bourmaud A, Kechichian A, Desmeules F. The impact of direct access physiotherapy compared to primary care physician led usual care for patients with musculoskeletal disorders: a systematic review of the literature. Disabil Rehabil. 2021;43(12): 16371648.
15. Ojha HA, Snyder RS, Davenport TE. Direct access compared with referred physical therapy episodes of care: A systematic review. Phys Ther. 2014;94(1):14-30.
16. Piano L, Maselli F, Viceconti A, Gianola S, Ciuro A. Direct access to physical therapy for the patient with musculoskeletal disorders, a literature review. J Phys Ther Sci.2017; 29(8):1463-1471.
17. Gagnon R, Perreault K, Berthelot S, et al. Direct-access physiotherapy to help manage patients with musculoskeletal disorders in an emergency department: Results of a randomized controlled trial. Acad Emerg Med. 2021; 28(8): 848-858.
18. Anggiat L, Altavas AJ, Budhyanti W. Joint Mobilization: Theory and evidence review. Int J Sport Exerc Heal Res. 2020;4(2):86-90.
19. Caparrós T, Pujol M, Salas C. General guidelines in the rehabilitation process for return to training after a sports injury. Apunt Med l’Esport. 2017; 52(196): 167-172.
20. Abe Y, Goh AC, Miyoshi K. Availability, usage, and factors affecting usage of electrophysical agents by physical therapists: A regional cross-sectional survey. J Phys Ther Sci. 2016; 28(11):3088-3094.
21. Panjaitan LA. Penggunaan Terapi Elektro-fisis Pada Satu Rumah Sakit Umum Swasta di Jakarta. J Fisioter.2020; 20(2):40-45.
| Citation: James Wilson HasoloanManik, KiranaWardhani, Adinda Amira Putri, et al. Direct access physiotherapy service model in primary health care facility: an observational study , International Journal of Medical and Exercise Science, March 2022; 8(1); 1210-1218. |