Beriman Rahmansyah1, Lucky Anggiat2
Corresponding Author:
Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
Email : beriman.rahmansyah@uki.ac.id
Author:
Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia
| ABSTRACT |
Background: In applying the physiotherapy interventions, physiotherapists frequently use electro physical agent (EPA) which is therapeutic modalities that have indeed become one of the popular therapies besides exercise therapy and manual therapy. This study aimed to identify the availability and usage of EPA by physiotherapists in East Jakarta, Indonesia.
Methods: This study used online survey research method. The target population was physiotherapists in East Jakarta who joined in the WhatsApp group of the Indonesian Physiotherapy Association, East Jakarta Branch. From 189 target respondents, only 73 respondents were willing to fill out the questionnaires given by the researchers.
Results:In the view from the availability of EPA modalities, most respondents or 91.8% answered the availability of electrical stimulation. It is followed by ultrasound therapy (84.9%). The least EPA modalities found in the respondent’s workplace were paraffin bath (23.3%). From the results, the use of EPA modalities in the form of ultrasound therapy and electrical stimulation was the most widely used. Subsequently, as many as 49.3% of respondents used the ultrasound therapy modality every day. A total of 45.2% of respondents used electrical stimulation modality.
Conclusion. The EPA modalities are quite widely available among physiotherapists in East Jakarta, Indonesia. The most widely available modalities are electrical stimulation, ultrasound therapy, and infrared radiation and in addition to the diathermy modality, which is also quite widely available. The availability of EPA tools is also in line with the frequency of use dominated by ultrasound therapy, electrical stimulation, and Microwave Diathermy.
Keywords: Electro Physical Agents; Modality, Intervention; Physiotherapy
| Received on 4thFebruary 2022, Revised on 19thFebruary 2022, Accepted on 26thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.008 |
INTRODUCTION
In clinical practice, physiotherapists carried out all physiotherapy processes from examination, planning, physiotherapy interventions and evaluations, to developing, maintaining, and restoring body movement and function1. Physiotherapists can provide interventions to patients with various options, such as manual therapy, therapeutic exercise, and interventions with physical equipment as well as electrophysical and mechanical modalities2. In applying the physiotherapy interventions, physiotherapists frequently use electro physical agent (EPA) which is therapeutic modalities that have indeed become one of the popular therapies besides exercise therapy and manual therapy3.
Electrophysical agent is defined as the use of physiotherapy modalities for evaluation, treatment, prevention of activity disturbances, and participation restrictions. With EPA, physiotherapist can help establish a physiotherapy diagnostic and evaluate treatment outcomes4. Furthermore, EPAis an important component of physiotherapy and consists of the application of various forms of EPA for therapeutic purposes3. Electro physical agents modalities are generally categorized as thermal (hot and cold), electromagnetic (diathermy, ultraviolet, and infrared light), or mechanical (traction and compression)5,6. Electro physical agents is very widely used in physiotherapy interventions because it has become a standard in hospitals, such as Micro Wave Diathermy (MWD), Short Wave Diathermy (SWD), Infra-Red Radiation, and Laser Therapy and Ultrasound therapy (US)7. There are also electrical stimulations such as Transcutaneous Electrical Nerve Stimulation (TENS), Interferential Therapy (IFT), and Neuromuscular Electrical Stimulation (NMES). However, there are also types of non-thermal applications, namely variations in the use of Pulsed MWD, Pulsed SWD, Pulsed Laser Therapy, and Pulsed Ultrasound therapy. However, scientific results related to the frequency of using EPA device are still rare8,9.
There are not many studies on the use of EPA in Indonesia. Therefore, the development of EPA in Indonesia is not known4,8. From that background, this study is needed to be able to identify the use of EPA by physiotherapists. However, this study is a preliminary study in the East Jakarta area because it is close to the researchers’ university (Universitas Kristen Indonesia) and there are quite a number of representative hospitals. In addition, it is suggested that future studies are conducted more comprehensively. This study also aims to see the availability of EPA modalities used by physiotherapists so that they can be used as a reference in teaching and learning EPA at universities.
METHODOLOGY
This study used online survey research method. The target population were physiotherapists in East Jakarta who joined in the WhatsApp group of the Indonesian Physiotherapy Association, East Jakarta Branch with 189 respondents. The questionnaires were distributed to all respondents. However, only 73 physiotherapists were willing to fill them out. The data were collected using survey questionnaires to obtain responses from the respondents. The questionnaire consisted of 14 questions. The questions in the questionnaire were divided into several parts, firstly profile part which includes the identity of the physiotherapist and their education level. However, the respondent’s detailed identity was not displayed to maintain the respondent’s privacy. Subsequently, the second part was related to the physiotherapist’s work experience, namely the length of years of work, the number of patients treated in one day, and the condition of the patients often encountered. After that is the last part related to the availability and frequency of using EPA modalities. Before distributing the questionnaires, the questionnaires were tested by physiotherapists and made improvements if needed. The questionnaires were distributed within 3 months, namely December 2021 to February 2022. After the distribution was the processing of the survey results from the questionnaires. At the end, the results were reported and discussed.
RESULTS AND DISCUSSION
From 189 target respondents, only 73 respondents were willing to fill out the questionnaires given by the researchers. The physiotherapist’s identity is in the following table of respondent profiles.
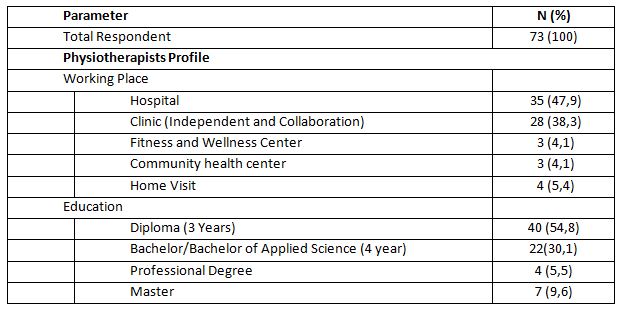
It can be seen that of 73 physiotherapists as respondents in this survey, 35 people or around 47.9% worked in hospitals and only 4 people or around 4.1% worked in community health centers. The previous study also stated that in a hospital, there were more than 10 physiotherapists8. The workplace of physiotherapists in some countries is also dominated by hospitals and clinics10,11. In terms of education level of the respondents, as many as 40 respondents or around 54.8% had a diploma which is three-year study in university level.
There were 7 people or around 9.6% who had a master’s degree. In Indonesia, those who are given the authority to practice physiotherapy are physiotherapists starting at the diploma level to the professional level2. This is already in line with the provisions of the World Physiotherapy Organization, although there is still a national government that gives authority to physiotherapists at the diploma level1. Thus, physiotherapists in East Jakarta are considered to meet the minimum qualifications to practice physiotherapy. Likewise, in some countries, it is found that the qualifications for physiotherapy education are quite varied and still follow the national regulations of each country10,11.
The following result of the questionnaire is about the physiotherapists’ work experience which describes the range of work of physiotherapists, the average number of patients treated in one day, and the condition of patients treated by the physiotherapists. The data are presented in the following Table 2.
The following result of the questionnaire is about the physiotherapists’ work experience which describes the range of work of physiotherapists, the average number of patients treated in one day, and the condition of patients treated by the physiotherapists. The data are presented in the following Table 2.
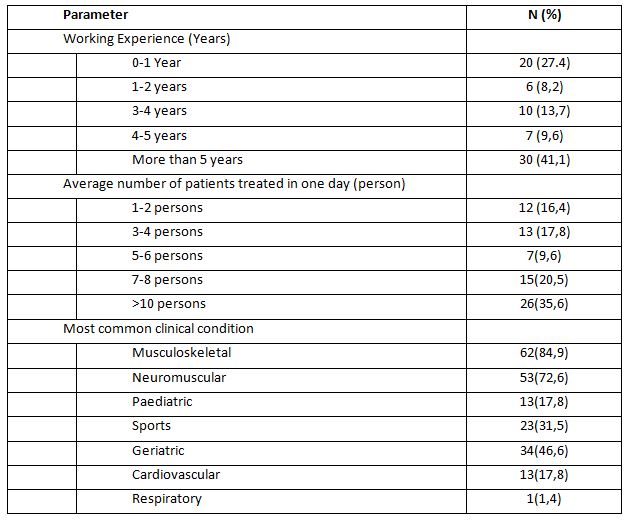
In the table, it can be seen that the majority of respondents who have worked for more than five years are 41.1%, which indicates that the physiotherapists have experienced in working and using EPAmodalities. Physiotherapists with more than five years of experience will indeed provide better patient satisfaction12.
As many as 35.6% physiotherapists treated more than ten patients daily and around 16.4% treat one to two patients every day. From these data, it can be seen that some physiotherapists still treat too many patients in one day, that is, more than ten patients daily. If there are more than 10 patients treated daily by the physiotherapist, assuming one patient is an hour, it indicated that the physiotherapist in providing services is not optimal, because in general, the number of daily working hours is only about 8 hours11–13. However, there are not many studies that support this. It can also cause harm to the physiotherapist who is likely to experience fatigue. Thus, the number of physiotherapists must be increased in order to provide optimal services14.
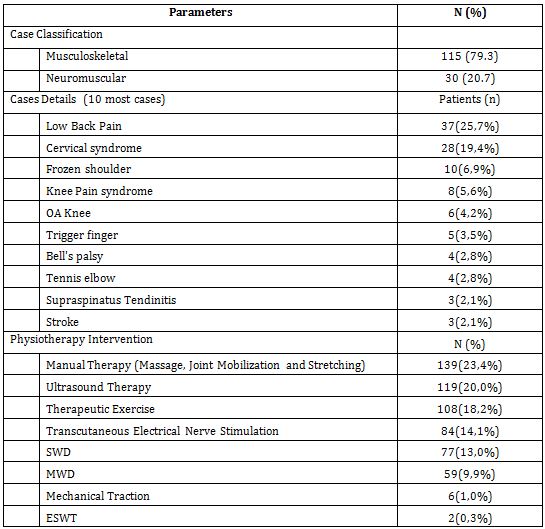
Most respondents or 84.9% treated patients with musculoskeletal condition and the least treated were patients with respiratory condition. Several studies also support this. As in a study by Jahan et al., (2021) who found that physiotherapists mostly treated musculoskeletal patients. Likewise, in a study in a hospital, physiotherapists generally dealt with various types of patients with musculoskeletal disorders8. In addition, a study in a certain region also stated that musculoskeletal cases were very dominant in the physiotherapy practice15.
The following result is related to the availability of EPA modalities as well as the frequency of use. Table 3 shows the available modalities in each physiotherapist’s workplace.
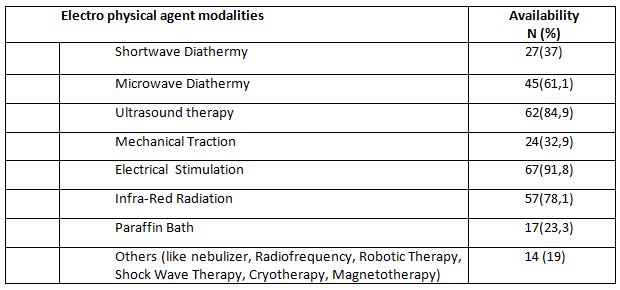
In the view from the availability of EPA modalities found in each respondent’s workplace, most respondents or 91.8% answered the availability of electrical stimulation. It is followed by EPA modalities in the form of ultrasound therapy (84.9%). The least EPA modalities found in the respondent’s workplace were paraffin bath (23.3%). The availability of diathermy modalities in the form of Micro Wave Diathermy at the respondents’ workplace had a considerablevalue of around 61.1%, including Short Wave Diathermy which had a considerable percentage (37%).
There are also heat therapy modalities that are quite popular among physiotherapists, namely Infrared Radiation device which was answered by 50% of the total respondents. A study in Australia also shows that ultrasound therapy is a modality that has considerable availability16. Furthermore, the use of EPA interventions is still a trend among physiotherapists in Asia4,17.
However, apart from Asia, in America there is also a trend in the use of EPA18. The most widely available modality tools are cold and hot agents, with electrical stimulation therapy and ultrasound therapy. It was also found that in America, there are very few diathermy modalities available.
From the results of this study, it can be seen that physiotherapists in East Jakarta have the availability of adequate EPA modalities in accordance with the needs of the patients. Nevertheless, the needs for EPA must really be acknowledged and the latest research developments should keep up with the effectiveness of existing EPA modalities(Belanger, 2015; Bellew et al., 2016;
Goh &Abe, 2015). There are also some EPA modalities in the table 3 that tend to be new and have very little availability.In addition, the existing modalities data can also be a reference for lecturers to continue to provide updates on the science of EPA modalities. By understanding the availability, the lecturer needs to provide understanding to physiotherapy students at the university in order to be more critical in the use of electrophysical instruments in clinical practice. Previous studies also used the survey results in the availability of physiotherapy modalities for teaching purposes at universities18.
The last results of this study were related to the frequency of the use of EPA. In this study, we only prepare the types of modalities that are popularly used by physiotherapists, which are SWD, MWD, US, IRR, Mechanical Traction, Electrical Stimulation, LASER, and paraffin bath. It is also based on the availability of such modalities at the physiotherapists’ place of practice. Moreover, we conducted a survey related to how many combinations of EPA modalities were used by physiotherapist for each patient with certain condition.
The time frame we chose was one week to make it easier for the physiotherapists to remember the modalities they used on average. Frequency classification was also made using the range: always (everyday), often (four to five times a week), rarely (one to three times a week), and none (not using the modality or the modality is not available). All usage and frequency data are shown in Table 4.
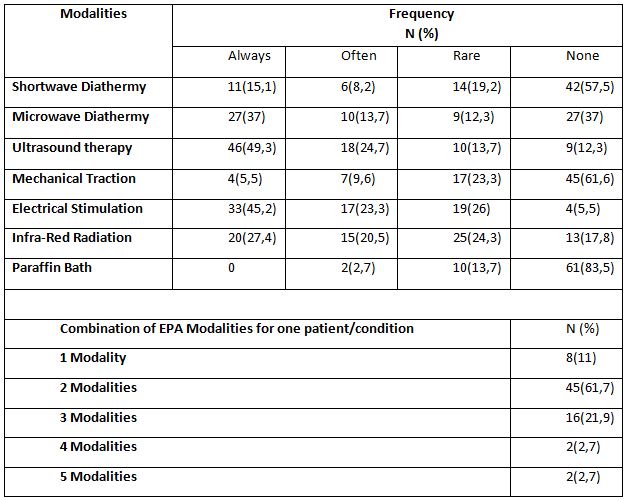
From the results above, it can be seen that the use of EPA modalities in the form of ultrasound therapy and electrical stimulation was the most widely used. Subsequently, as many as 49.3% of respondents used the ultrasound therapy modality every day and only 12.3% never used the ultrasound therapy modality. A total of 45.2% of respondents used electrical stimulation modality and only 5.5% never used it. The modalities of paraffin bath and mechanical traction were the least used EPA modalities. As many as 83.5% of respondents never used paraffin bath and 61.6% of respondents never used mechanical traction.
The use of electrical stimulation is believed to reduce neuromusculoskeletal disorders. As in the results of a previous study by Manik & Rahmansyah (2021), it mentioned that EPA modalities in the form of electrical stimulation can reduce pain in neuromuscular and musculoskeletal conditions20. In line with this, a study by Abe et.al (2016), which surveyed 1099 respondents from 170 hospitals/clinics showed that the use of electrical stimulation in the form of low frequency currents and ultrasound therapy ranked second and third below the modality in the form of hot pack4. Furthermore, a study by Greco et al. (2018) also found that the use of electrical stimulation was quite dominant, along with ultrasound therapy and thermal modality (cold or hot). In addition, we should take attention to the results of the existing research is that despite the availability of diathermy physiotherapy tools, it does not guarantee that they are often used. The trend that is developing in the world is that diathermy modality should be abandoned and replaced with more effective modality 9,18,19.
In this study, it was also found that physiotherapists used more than two modalities in one patient with one condition. This shows that physiotherapists very often used EPA modalities. The use of more than two modalities is possible if the patient’s condition requires intensive intervention and there are more than two symptoms in one condition19,21. Knowledge of the use of appropriate and effective interventions needs to be carried out in the future to be able to provide optimal services to the patients22,23.
This study is a very simple survey as a preliminary study. More complex analysis in the existing data can be done as a development of future research. Likewise, the survey in this study was only conducted in one city, so more detailed research using a larger population is needed as a development in the future. This study also has many limitations, one of which is the willingness of the physiotherapist to fill out the questionnaire. Therefore, it is possible to conduct more interesting research that can attract the attention of the physiotherapist to fill out the questionnaires in the future. The reasons for selecting interventions related to the condition of the patients have not been captured in this study, so further research development is needed.
CONCLUSION
The EPA modalities are quite widely available among physiotherapists in East Jakarta, Indonesia, both in health facilities and independent clinical practices. The most widely available modalities are electrical stimulation, ultrasound therapy, and infrared radiation and in addition to the diathermy modality, which is also quite widely available. The availability of EPAtools is also in line with the frequency of use dominated by ultrasound therapy, electrical stimulation, and Microwave Diathermy. Physiotherapists also quite often use EPA because in one patient with one condition, physiotherapists frequently use more than one modalities.
Recommendation: Physiotherapists in East Jakarta should pursue their education to a higher level to find out the latest developments in electrophysical interventions. The use of diathermy should also be reduced by its decreasing use abroad. The number of patients handled by one physiotherapist in one day is too many, so it is necessary to add the number of physiotherapists who work in a hospital. Based on the result, it also suggested that at universities, it is still necessary to provide scientific development in EPA, especially the frequent modalities like ultrasound therapytherapy, electrical stimulation, and diathermy so that when the students graduate, they can practice well.
Acknowledgement: The researcher would like to thank every physiotherapist who is willing to participate in this research. Furthermore, we also thank the of the Indonesian Physiotherapy Association, East Jakarta Branch, for allowing us to collect data from the organization members.
Conflict of interest: The author has no conflict of interest to declare.
Funding of study: This study was funded by Universitas Kristen Indonesia.
Compliance with Ethics: This research does not provide anything that is harmful to the respondents so that it does not use ethical research. However, this research was conducted with the permission of the university and the permissionfrom chairman of the Indonesian physiotherapy association, East Jakarta branch, with reference number 03/IFI-JAKTIM/XI/2021.
REFERENCES
1. World Confederation for Physical Therapy. Guideline for standards of physical therapy practice. Published online 2011:1-19. https://world.physio/sites/default/files/2020-07/G-2011-Standards-practice.pdf
2. Kementerian Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan No.80 Tahun 2013.; 2013.
3. Watson T. The role of electrotherapy in contemporary physiotherapy practice. Man Ther. 2000;5(3):132-141.
4. Abe Y, Goh AC, Miyoshi K. Availability, usage, and factors affecting usage of electrophysical agents by physical therapists: A regional cross-sectional survey. J Phys Ther Sci. 2016;28(11):3088-3094. doi:10.1589/jpts.28.3088
5. Starkey C. Therapeutic Modalities. Fourth Edi. (McDonald Q, ed.). F. A. Davis Company; 2013. www.fadavis.com
6. Belanger A-Y. Therapeutic Electrophysical Agents. Lippincott Williams & Wilkins; 2015.
7. Kementerian Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia Nomor 65 Tahun 2015 Tentang Standar Pelayanan Fisioterapi. Vol 16.; 2015.
8. Panjaitan LA. Penggunaan Terapi Elektrofisis Pada Satu Rumah Sakit Umum Swasta di Jakarta. J Fisioter. 2020;20(2):40-45.
9. Goh A-C, Abe Y. New directions in electrophysical agents : where do we go from here? Japanese J Electrophysical Agents VO – 22. 2015;(April):4.
10. Khairy WA, Bekhet AH, Sayed B, Elmetwally SE, Elsayed AM, Jahan AM. Prevalence, profile, and response to work-related musculoskeletal disorders among egyptian physiotherapists. Open Access Maced J Med Sci. 2019;7(10):1692-1699.
11. Nkhata L a, Zyaambo C, Nzala SH, Siziya S. Work-related Musculoskeletal Disorders : prevalence , contributing factors and coping strategies among Physiotherapy personnel in Lusaka , Kitwe and Ndola districts , Zambia. Physiotherapy. 2010; 37(4):262-267.
12. Jahan AM, Rwaiha AE, Gusaibat SR, Al-Ahwal NA, Al-Jafairi ZM, Al-Rashidi MA. Patient Satisfaction With Physiotherapy Services in Libya: A Cross-Sectional Study. J Patient Exp. 2021;8:1-7.
13. Hima Bindu P, Thiruppathi A. Work Related Musculoskeletal Discomfort (WRMSD) among Physiotherapists. Int J Physiother. 2014;1(4):200.
14. Manurung NSA, Sunaryo T, Gunawan I, Anggiat L. Analysis of the need for Physiotherapists in a private hospital in Indonesia using the workload indicator of staffing need referring to the implementation of the physiotherapy process as risk mitigation of services. Int J Med Exerc Sci. 2020;06(01):697-705.
15. Odumodu IJ, Olufunlayo TF, Ogunnowo BE, Kalu ME. Satisfaction With Services Among Attendees of Physiotherapy Outpatient Clinics in Tertiary Hospitals in Lagos State. J Patient Exp. 2020;7(4):468-478.
16. Chipchase LS, Williams MT, Robertson VJ. A national study of the availability and use of electrophysical agents by Australian physiotherapists. Physiother Theory Pract. 2009;25(4):279-296.
17. Shah SGS, Farrow A. Trends in the availability and usage of electrophysical agents in physiotherapy practices from 1990 to 2010: a review. Phys Ther Rev. 2012;17(4):207-226.
18. Greco JL, Lamberg EM, McKenna RF, Muratori LM. Trends in availability and usage of biophysical agents among physical therapists in the United States. Phys Ther Rev. 2018;23(2):116-123.
19. Bellew JW, Michlovitz SL, Nolan TP. MODALITIES For Therapeutic Intervention. F. A. Davis Company; 2016.
20. Manik JWH, Rahmansyah B. The effect of nerve mobilization on the median nerve in pain perception of electrical stimulation. Int J Med Exerc Sci |2021;7(3). 2021; 7 (August):1104-1112.
21. Kim MK, Ji SG, Cha HK, Chang JS. Effects of electromagnetic diathermy in conjunction with nerve mobilization in the management of lower back pain. J Phys Ther Sci. 2012;24(12):1337-1339.
22. Beales D, Mitchell T, Holthouse D. Stepped care for musculoskeletal pain is ineffective: A model for utilisation of specialist physiotherapists in primary healthcare management. Aust J Prim Health. 2021;27(6):431-436.
23. Tiktinsky R, Chen L, Narayan P. Electrotherapy: Yesterday, today and tomorrow. Haemophilia. 2010;16(SUPPL. 5):126-131.
| Citation: Beriman Rahmansyah, Lucky Anggiat. Availability and usage of electro physical agentmodality by Physiotherapist in East Jakarta, International Journal of Medical and Exercise Science, March 2022; 8(1); 1228-1237. |