Swethaa. D1, Meena2, Tejaswee3
Corresponding Author:
1Associate Professor, Venkata Padmavathi Institute of Medical Sciences, Tirupati, Andra Pradesh, E. Mail Id: dswethaa3@gmail.com
Co Authors:
2MPT Graduates, Venkata Padmavathi Institute of Medical Sciences, Tirupati, Andra Pradesh
3MPT Graduates, AVM College of Physiotherapy, Kadapa, Andra Pradesh
Abstract
| Background of the Study: Aerobic exercises have shown effect on decrease severity and mortality in tolerant with heart valve illness. Aim of the study was to find the endurance and quality of life in patient with heart valve surgery. Methodology: This was an experimental study conducted in Post Surgical Cardiology Department of Sri Venkateswara Rama Narayana Ruya Government General Hospital, Tirupati. In this study, 60 patients are assigned into two Groups A and B, 30 in each group. Age group of 40-60 was selected for this study. Measurement tools and materials used for this study were Pulse oximeter, Sphygmomanometer, Cycle ergo meter, Stethoscope, Stop watch, Inch tape, Chair with arm rest, Cones, Shoes. Outcome measures used were 6 Minute walk and test, St. George’s respiratory questionnaire. Result: Endurance training and quality of life showed significant improvement in 6- minute walk test and St. George’s respiratory questionnaire between pre and post test. Conclusion: This study shows that endurance training is effective improving the aerobic capacity and quality of life in patient with heart valve surgery patients. |
Keywords: Quality of life; Heart valve surgery; Ergo meter; 6- minute walk test; St. George’s respiratory questionnaire
Received on 04th October 2021, Revised on 20th November 2021, Accepted on 24th November 2021 DOI:10.36678/IJMAES.2021.V07I04.002
INTRODUCTION
Heart Valve Disease represent one-third of all coronary illness and are expanding in predominance because of a old age and advances in treatment techniques. As of now, heart valve illnesses are generally degenerative in nature, but profoundly pervasive in non-industrial nations because of rheumatic coronary illness 1-4.
Heart valve sicknesses is either left sided (aortic and mitral valve illness) or a mixed. Heart valve sickness is frequently a suggestive with symptoms. At the point when indicative, that clinical show incorporates dyspnea, exhaustion, liquid maintenance and diminished physical capacity. Indicative heart valve infection is related with critical mortality and horribleness and seriously sway wellbeing related personal satisfaction and actual limit5-7.
Before valve surgery procedure dyspnea and physical in limit is normal. After the surgery procedure, individuals are regularly immobilized because of hospitalization, conceivable post-medical procedure difficulties and limitation intended to help sensation of sternum. Therefore, their physical capacity is in danger of more risk. Also, open heart medical procedure, personal satisfaction might be influenced with mental issues like burdensome manifestations and tension 8-10.
In rundown, after heart valve medical procedure not exclusively is there a danger of mortality and bleakness, incorporates emergency clinic readmissions and result medical care cost, yet significantly patients additionally experience actual mental or social recuperation issue that may adversely affect on their wellbeing related personal satisfaction11.
Aerobic exercise is related with useful and morphologic heart transformations which remember bradycardia and increments for valve thickness and size of every one of the four chambers. Various investigations have proposed that perseverance practice preparing can work on significant out come in quiet with heart valve medical procedure 12.
Aerobic exercise may likewise decrease grimness and mortality in tolerant with heart valve illness. Intense exercise activities of the ventilatory muscles in valve one more type of breathing activity utilized dominatingly to work on pneumonic capacity and increment exercise capacity 13.
The activity with cycle ergo meter in stage 2 of cardiovascular recovery can further develop fringe muscle strength and practical limit. It can expand oxygen transport and venous return as well as diminishing postoperative difficulties and furthermore modifies muscle work, forestalling greenery misfortune practices with or without obstruction by aloof way, dynamic helped or dynamic activities 14.
The adequacy of various methods of intense exercise on wellbeing, for example, cycle ergo meter training, walking or running has been shown in a few investigations. Among these mod of activities, cycle ergo meter preparing is especially elective since it is generally simple, safe purposes and causes no connected wounds15.
Cycle ergo meter preparing is generally a significant part of any perseverance practice program that looks to work on oxygen consuming limit and cardio vascular wellbeing. Cycling is a wellbeing type of perseverance practice and as a non weight bearing movement; less affects joints and is along these lines less unpleasant for the body. At long last, cycle ergo meter is attainable in any event, for fragile more established people 16.
Physiologically it works on cardiovascular wellbeing, directed glucose, helps in diminishing weight, reinforces resistance, and further develops muscle strength and expanding Range of movement. Chest versatility practices forestall pneumonic inconveniences and torment during in persistent phase. Post operatively respiratory disability and useful impediment found in quiet with heart valve medical procedure, for example, cut torment and seepage, diminished thoracic divider portability 17.
Aim of the Study: To improve the endurance and quality of life in patients with heart valve surgery.
METHOD:
This was an experimental study with 60 Subjects were taken 30 in each group. The study was conducted in post surgical cardiology department of Sri Venkateswara Rama NarayanaRuya Government General Hospital (SVRRGGH), Tirupati.
Materials and methods:
Material Needed: Pulse oximeter, Sphygmomanometer, Cycle Ergo meter, Stethoscope, Stop watch, Chair with armrest, Inch tape, Cones, Shoes.
Selection Criteria:
Inclusion Criteria: Both Female and male patients heart valve surgery , Age 40 to 60, Aortic Valve stenosis, Mitral Valve stenosis, Right or Left side heart valve surgery, Patients who are willing to participant actively in the study, Annular Valve disease.
Exclusion criteria : Ischemic Heart disease, Musculoskeletal system diseases, Pregnant or breast feeding woman, Non cooperative patients, Psychological patients, Malignancy.
Intervention:
Experimental Group: Experimental group received endurance training; 6Days/week, 2 sessions/day, 4 weeks, Cycle ergo meter- 10 minutes / 2 sessions/day, Chest mobility, exercise ; 8 -10 repetition/set.
Control Group: Control group receives chest mobility exercises; 3 Days/week, 2 sessions/ day, 4 weeks.
Outcome Measures
SIX (6) minutes walk test:
The 6 Minute Walk Test is a sub-maximal exercise test used to survey vigorous limit and perseverance. The distance covered throughout a period of 6 minutes is utilized as the result by which to think about changes in execution limit. The test was at first intended to help in the evaluation of patient with cardiopulmonary issues. Progressively, it was presented in various different conditions.
It assesses the practical limit of the individual and it gives important data in regards to every one of the frameworks during actual work, including respiratory and cardiovascular frameworks, blood course, neuromuscular units, body digestion, and fringe circulation.
Hardware Required: Stopwatch Measuring/trundle wheel to quantify distance covered, 30 meter stretch of unobstructed walkway. Two cones used to check the distance that should be covered. Pulse oximeter for estimating pulse and SpO2 (discretionary). Borg Breathlessness Scale (discretionary).
Set-Up:
Spot cones at one or the flip side of the 30 meter stretch as defining moments. Have seats set up one or the other side and most of the way along the walking 13.
Patient Instructions:
The object of this test is to stroll beyond what many would consider possible for 6 minutes. You will stroll to and fro in this corridor. Six minutes is quite a while to walk, so you will endeavor. You will likely escape breath or become depleted. You are allowed to dial back, to stop, and to rest as fundamental. You might incline toward the divider while resting; however continue strolling when you are capable. You will stroll to and fro around the cones. You should turn energetically around the cones and proceed back the alternate way without a second thought. Presently I will show you. Kindly watch the manner in which I turn decisively.”
Peruse this normalized consolation during the test: After the first moment: “You are progressing nicely. You have 5 minutes to go.” When the clock shows 4 minutes remaining: “Keep doing awesome. You have 4 minutes to go.”
At the point when the clock shows 3 minutes remaining: “You are progressing nicely. You are mostly done. At the point when the clock shows 2 minutes remaining: “Keep doing awesome. You have just 2 minutes left. At the point when the clock shows 1 moment remaining: “You are progressing nicely. You just have 1 moment to go.
With 15 seconds to go: “In a second I will advise you to stop; at the point when I do, stop right, where you are and I will come to you.” At 6 minutes: “Stop” In the event that the member stops whenever earlier, you can say: “You can incline toward the divider assuming you might want; keep strolling at whatever point you feel capable.”
Try not to utilize different inspirational statements (or non-verbal communication) to impact the patient’s strolling speed. Go with the member along the strolling course, however keep simply behind them. Try not to lead them.
In the event that accessible record the distance at which the oxygen immersion drops < 88%.
St. George Respiratory Questionnaire (SGRQ):
St George Respiratory Questionnaire is a sickness – explicit instrument intended to quantify sway on generally speaking wellbeing, day to day existence, and saw prosperity in tolerant with obstructive aviation routes infection.
An all out score of St George Respiratory Questionnaire determined from 0 (no wellbeing debilitation) to 100 (most extreme wellbeing Impairment). Notwithstanding the all out score, there is additionally a score for every space: side effects, movement, and effect which are scored 0 – 100 also.
Data analysis: Data was analyzed by using the SPSS 18.0 version and also excel package. Descriptive Statistics was used for both the groups. The relationship within the groups was analyzed by t-test for paired sample observation and between the groups was analyzed by independent two sample t-test.
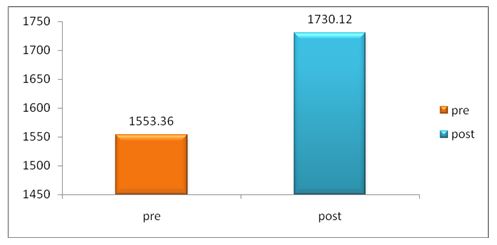
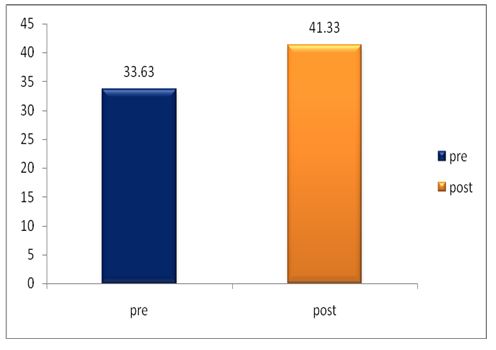
The pre and post difference of 6 MWT of experimental group of mean and standard deviation was analyzed statistically tested by paired t-test. The result is presented in table-1

From table-1, it is found that the mean value of 6MWT experimental group before application of Endurance Training mean value is 1553.36 The ‘P’ value is 0.0001 and after application of Endurance Training and is 1730.12The ‘P’ value is 0.0001 Since the P value is less than 0.001 it is concluded that there is a significant improvement in 6MWT experimental group.
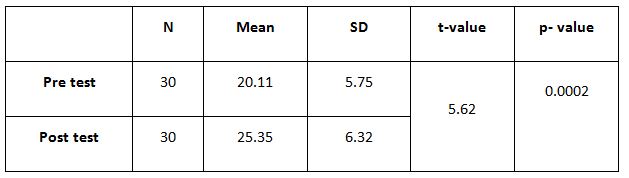
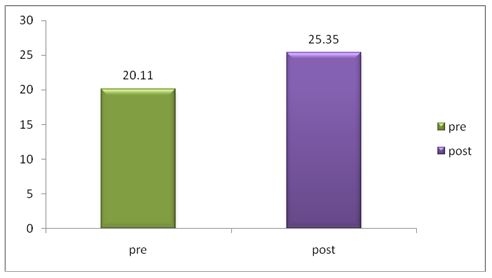
The pre and post difference of 6 MWT control group was analyzed statistically by paired t-test. The result is presented in table -2.
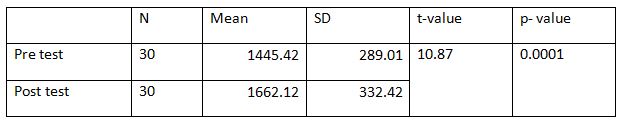
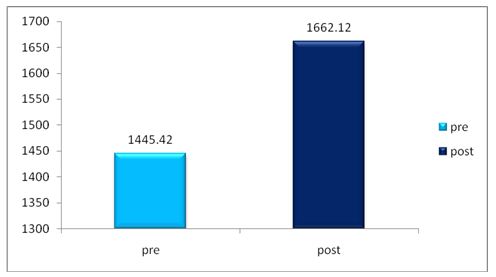
From table-2, it is found that the mean value of 6 MWT before application chest mobility exercise is 1445.42 and after application of chest mobility exerciseis 1622.12 The ‘P’ value is 0.0001. Since the P value is less than 0.001 it is concluded that there is a significant improvement in 6 MWT in the control group.
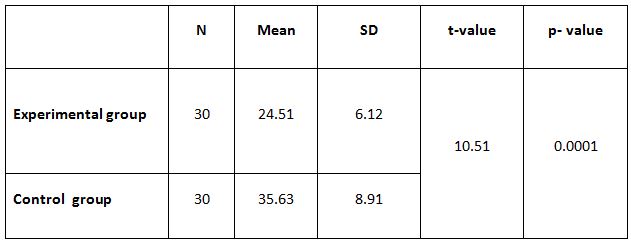
The pre and post difference of 6 MWT between groups was analyzed statistically by paired t-test. The result is presented in table -3.
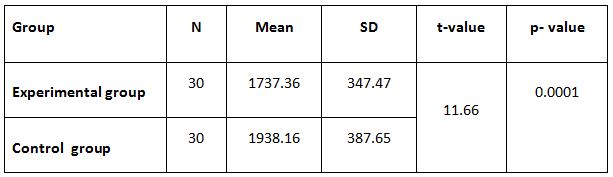
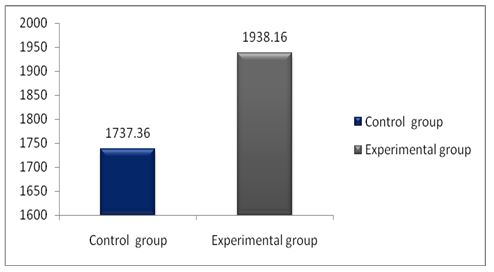
From table-3, it is found that the mean value of 6 MWT before application chest mobility exercises is 1737.36 and after application chest mobility exercises is 1938.16 The ‘P’ value is 0.0001. Since the P value is less than 0.001 it is concluded that there is a significant improvement in 6 MWT in the experimental group.
The pre and post difference of control group of mean and standard deviation was analysed statistically tested by paired tested by paired t-test. The result is presented in table 1.
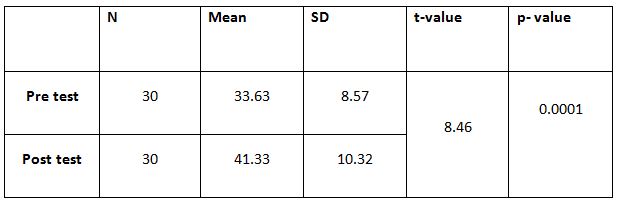
The pre and post difference of SGRQ of control group of mean and standard deviation was analysed tested by paired t-test.the result is presented in table-5.
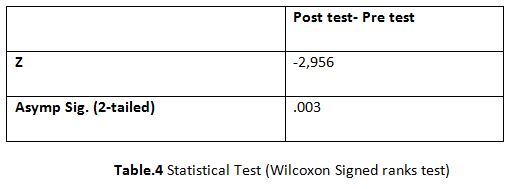
The post difference of dyspnoea in SGRQ between experimental and control group was analyzed statistically by using independent two sample t-test. The result is presented in Table-6.
RESULT
Endurance training and quality of life shows significant improvement in 6 minute walk test and ST George respiratory questionnaire in patients with heart valve surgery.
The result showed that there was significant difference between pre and post test training in experimental group.
DISCUSSION
Endurance training is a pattern helpful for patient with heart valve surgery. Endurance training improves muscle strength, venous return, and aerobic capacity and prevents complications. In experimental group and control group the endurance training was given in phase 2 of surgery.
The endurance training by cycle ergometer is given 10 minutes twice daily for 4 weeks along with chest mobility exercises 2 sessions per day. Chest mobility exercises are given for 3 days/week/ 2 sessions/ 4 weeks. The study found significant improvement in endurance training and quality of life in experimental group compared with the control group.
The parameters of 6 minute walk test and St George respiratory questionnaire showed significant improvement in experimental group compared with the control group.
The exercise component of cardiac rehabilitation is useful for reversing the symptoms associated with deconditioning. Women with mitral valve prostheses improved their peak metabolic equivalent capacity by 19% and their physical working capacity by 25% after undergoing an 8-week program, whereas control subjects did not improve 19.
Recurrent symptoms and hemodynamic decomposition are leading causes of hospital admission. One study showed that heart failure patients in cardiac rehabilitation reduced readmissions by 19% and mortality by 22% 20.
In stable patients with chronic class II and III heart failure who participated in exercise training for 14 months, survival was prolonged by an additional 1.82 years at a cost of $1,773 per life-year saved in the exercise group compared with non-exercising control subjects 21.
Ethical clearance: There was no risk of conducting this study.Ethical clearance was obtained from the ethical committee of Venkata Padmavathi Institute of Medical Sciences, Tirupati, Under the NTR University of Health Sciences, Vijayavada with reference No.198/A4/Diss/MPT/19-20 approval letter dated 25thFebruary 2021.
Conflicts of Interest: There is no conflict of interest to conduct this study.
Fund for the study: This is self-funded study.
CONCLUSION
In present study there was significant difference found in the post test of control and experimental group. Comparison of pre and post test of experimental and control groups respectively showed significant difference however the post test comparison between control and experimental group had shown high statistical difference.
The experimental group treated with endurance training, showed greater improvement in aerobic capacity and quality of life. The study concludes that endurance training is effective in improving aerobic capacity, cardiovascular health and quality of life in patient with Heart Valve Surgery.
REFERENCES
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M: Burden of valvular heart diseases: a population-based study. Lancet. 2006, 368: 1005-1011. 10.1016/S0140-6736(06)69208-8.
- Sire S: Physical training and occupational rehabilitation after aortic valve replacement. Eur Heart J. 1987, 8: 1215-1220.
- Davies EJ, Moxham T, Rees K, Singh S, Coats AJ, Ebrahim S, Lough F, Taylor RS: Exercise based rehabilitation for heart failure. Cochrane Database Syst Rev. 2010, 4: CD003331
- Newell JP, Kappagoda CT, Stoker JB, Deverall PB, Watson DA, Linden RJ: Physical training after heart valve replacement. Br Heart J. 1980, 44: 638-649. 10.1136/hrt.44.6.638
- Gohlke-Barwolf C, Gohlke H, Samek L, Peters K, Betz P, Eschenbruch E, Roskamm H: Exercise tolerance and working capacity after valve replacement. J Heart Valve Dis. 1992, 1: 189-195.
- Lim HY, Lee CW, Park SW, Kim JJ, Song JK, Hong MK, Jin YS, Park SJ: Effects of percutaneous balloon mitral valvuloplasty and exercise training on the kinetics of recovery oxygen consumption after exercise in patients with mitral stenosis. Eur Heart J. 1998, 19: 1865-1871. 10.1053/euhj.1998.1146.
- Piotrowicz E, Baranowski R, Bilinska M, Stepnowska M, Piotrowska M, Wojcik A, Korewicki J, Chojnowska L, Malek LA, Klopotowski M, Piotrowski W, Piotrowicz R: A new model of home-based telemonitored cardiac rehabilitation in patients with heart failure: effectiveness, quality of life, and adherence. Eur J Heart Fail. 2010, 12: 164-171. 10.1093/eurjhf/hfp181.
- Stessman J, Hammerman-Rozenberg R, Cohen A, Ein-Mor E, Jacobs JM. Physical activity, function, and longevity among the very old. Arch Intern Med. 2009; 169:1476–83. doi: 10.1001/archinternmed.2009.
- Vogel T, Brechat PH, Leprêtre PM, Kaltenbach G, Berthel M, Lonsdorfer J. Health benefits of physical activity in older patients: a review. Int J ClinPract. 2009; 63:303–20. doi: 10.1111/j.1742-124.
- Wen CP, Wai JP, Tsai MK, Yang YC, Cheng TY, Lee MC, et al. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet. 2011; 378:1244–53.
- Ekelund U, Franks PW, Sharp S, Brage S, Wareham NJ. Increase in physical activity energy expenditure is associated with reduced metabolic risk independent of change in fatness and fitness. Eur Diabetes Care. 2007; 30:2101–6. doi: 10.2337/dc07-0.
- Acree LS, Longfors J, Fjeldstad AS, Fjeldstad C, Schank B, Nickel KJ, et al. Physical activity is related to quality of life in older adults. Health Qual Life Outcomes. 2006; 4:37. doi: 10.1186/1477-7525-4-37.
- Davis MG, Fox KR. Physical activity patterns assessed by accelerometry in older people. Eur J Appl Physiol. 2007; 100:581–9. doi: 10.1007/s00421-006-0320.
- Santos PMR, Riccia NA, Sustera EAB, Paisani DM, Chiavegato LD. Effects of early mobilisation in patients after cardiac surgery: a systematic review. Physiotherapy. 2017;103(1)
- Needham DM, Truong AD, Fan E. Technology to enhance physical rehabilitation of critically ill patients. Crit Care Med [Internet]. 2009; 37(10 Suppl): S436– 41.
- Hopkins RO, Mitchell L, Thomsen GE, Schafer M, Link M, Brown SM. Implementing a mobility program to minimize post-intensive care syndrome. AACN AdvCrit Care. 2016; 27(2):187-203.
- Wahab R, Yip NH, Chandra S, Nguyen M, Pavlovich KH, Benson T et al. The implementation of an early rehabilitation program is associated with reduced length of stay: A multi-ICU study. Journal of the Intensive Care Society 2016, Vol. 17(1) 2–11.
- Sommers J, Engelbert RH, Dettling-Ihnenfeldt D, Gosselink R, Spronk PE, Nollet F, van der Schaaf M. Physiotherapy in the intensive care unit: an evidence-based, expert driven, practical statement and rehabilitation recommendations. Clin Rehabil. 2015; 29(11):1051-63.
- Habel-Verge C, Landry F, Desaulniers D, et al. Physical fitness improves after mitral valve replacement. Can Med Assoc J 1987; 136:142–147.
- Belardinelli R, Georgiou D, Cianci G, et al. Randomized controlled trial of long-term moderate exercise training in chronic heart failure: effects on functional capacity, quality of life, and clinical outcome. Circulation 1999; 99:1173–1182.
- Georgiou D, Chen Y, Appadoo S, et al. Cost-effectiveness analysis of long-term moderate exercise training in chronic heart failure. Am J Cardiol 2001; 87:984-988.
| Citation: Swethaa. D, Meena, Tejaswee (2021).The comparative study of endurance training and quality of life in patient with heart valve surgery, ijmaes; 7(4); 1122-1134. |