Amjad Annethattil1, Mirshad Ali2, Ayman Sabbagh3
Coresponding Author
| 1Physiotherapy Specialist, Qatar Rehabilitation Institute, Qatar, E Mail: amjus2001@yahoo.co.in |
Co-Authors
2Physiotherapist, Qatar Rehabilitation Institute, Qatar 3Physiotherapy Specialist, Qatar Rehabilitation Institute, Qatar
ABSTRACT
| Background: In 2019 severe acute respiratory syndrome by corona virus 2 emanated at Wuhan, China and causes Corona Virus Disease-2019 (COVID-19).This global pandemic has put our world upside down and almost unprecedented global public health and economic crisis. The main mode of transmission was contact and droplet of inhaled 2019-n Co V. This virus is transmitted through respiratory secretions with 2019- n CoV. Large droplets from coughing, sneezing or a runny nose land on surfaces within two meters of the infected person. Many countries have a complete lock down, which most probably prevents participation in a regular rehabilitation program in outpatient centers and/or delivery of in-home physical therapy or other face-to-face treatment by primary care healthcare professionals with COVID-19 survivors in need for rehabilitative interventions. Recent studies show that being active during adulthood decreases systematic inflammation, an underlying factor in multiple chronic diseases. The anti-inflammatory impact of daily physical activity helps in lowering C-reactive protein, total blood leukocytes interleukin-6 and other inflammatory cytokines that may play a role in decreasing certain types of cancer, type two diabetes, cardiovascular diseases, sarcopenia and dementia. Aim: Aim of this knowledge practically helps us to counteract the consequences of increased physical inactivity and sedentary lifestyle during the lock-down period thereby lowering cardiovascular diseases and other commodities. Method: A literature search was done in electronic database using the key words exercise, physical activity, immunity, COVID 19 on 6th Jun 2020. Result: In a decennium, a lot of evaluation has substantiated the benefits of health related to regular physical activity. The normal functioning of the immune system is boosted with regular exercise. The anti-inflammatory influence of regular exercise is examined through various pathways; it functions as an immune system adjuvant, which improves defense reaction and metabolism. Conclusion: Proper physical activity helps in decreasing the need of critical care that directs us to hospital re-admission. Early mobilization and re-engagement in physical activity is important in the prevention of systemic consequences of a critical care and hospital admission. Patients should workout in proportion to their functional status. Keywords: Corona virus-2019, Respiratory syndrome, Sarcopenia, Dementia |
| Received on 14th September 2020, Revised on 22th October 2020, Accepted on 28th November 2020 DOI:10.36678/IJMAES.2020.V06I04.008 |
INTRODUCTION
Globally, millions of people are infected with the severe acute respiratory syndrome corona virus, causing the corona virus disease 19 (COVID-19). A proportion of the confirmed COVID- 19 patients are admitted to the hospital for acute care, due to severe respiratory symptoms and in some cases even acute respiratory distress requiring prolonged mechanical ventilation. It is very likely that a proportion of the COVID-19 patients will have a need for rehabilitative interventions during and directly after the hospitalization. This approach is also recommended by the World Health Organization. However, data on safety and efficacy of rehabilitation during and after hospitalization in these patients are lacking 1.
Equally, healthcare professionals cannot wait for well-designed randomized controlled trials to be published before they can start these rehabilitative interventions in daily clinical practice, as the number of COVID- 19 patient’s increases rapidly every day. Experts commented that recommencing daily physical activity as early as possible may positively affect functional recovery. However, patients may vary in physical, emotional and cognitive functioning. So, further assessment needs to be performed. Moreover, the encouragement to do regular daily activities should be in line with the local regulations for physical distancing and should go along with an advice to take time for recovery and rest periods, also taking an acceptable level of perceived exertion and dyspnea and oxygen de-saturation into consideration. Many countries have a complete lock down, which most probably prevents participation in a regular physical activities and rehabilitation program in most outpatient centers and/or delivery of in-home physical therapy or other face-to-face treatment by primary care healthcare professionals with COVID-19 survivors in need for rehabilitative interventions.
Physical activity continues to take on an increasingly important role in the prevention and treatment of multiple chronic diseases, health conditions, and their associated risk factors. It is one in all the foremost important things in improving health and reduces the danger of major illness and it depends upon overload, progression, and specificity of the exercise1. Physical activity is defined any bodily movement produced by skeletal muscles that needs energy expenditure. It shouldn’t be missed with “exercise”. Exercise, could be a subcategory of physical activity that’s planned, structured, repetitive, and purposeful within the sense that the development of one or more components of good condition is that the objective like walking, cycling and dancing 2, 3.
Many experts considered the measurement of exercise capacity to be very important in COVID-19 survivors, but some experts believe that this measurement should be limited to patients who remain physically limited 6-8 weeks following hospital discharge and who are tested negative at the time testing the exercise capacity. After discharge, patients with COVID-19 should be encouraged to do low/moderate intensity physical exercise at home in the first 6 to 8 weeks. Usually, these tasks range between 1.5 and 6 metabolic equivalents. Please see Ainsworth and colleagues for numerous examples 32, 33.
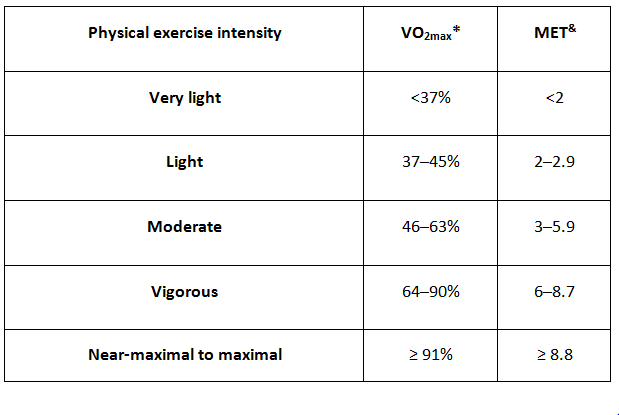
MET: Metabolic equivalent of task (index of energy expenditure, 1 MET = 3.5 mL/kg/min oxygen uptake). *VO2max: Combined capacities of the pulmonary and cardiovascular systems to deliver oxygen to contracting skeletal muscles, and the ability of those muscles to utilize it.
Impact of Exercise on immune system and anti-inflammation process: Molecular pathways have been examine the past period to divulge the means by which practice of workout uphold neuro-protection and decreases the risk of evolving communicable and non-communicable chronic diseases.4 Practicing workout has an anti-inflammatory influence mediated through multiple pathways. And it works as system adjuvant that improves defense activity and metabolic health and it has shown that increased physical activity is related to lower mortality risk in individuals with type 2 diabetes, hypertension and cholesterol 4, 5.
Evidence says repeated moderate intensity exercise improve the immune function response, as an acute exercise stimulates the interchange of innate system cells and components between lymphoid tissues and also the blood compartment. Although transient, a summation effect occurs over time, with improved immune surveillance against pathogens and cancer cells and thus decreased systemic inflammation. COVID-19 (corona virus disease 2019) could be a disease answerable for the continued global pandemic and its spreading everywhere the planet 7, 8, 9, 10.
Recent studies have demonstrated that COVID-19 impair the system response by with rising in inflammatory cytokines including IL2, IL7, IL10, GCSF, IP10, MCP1, MIP1A, and TNFα 9 .The local response to infections or tissue injury involves the assembly of cytokines that are released at the location of inflammation, a number of these cytokines facilitate an influx of lymphocytes, neutrophils, monocytes, and other cells. The effect of exercise could also be ascribed to the anti-inflammatory response elicited by an acute bout of exercise, which is partly mediated by muscle-derived IL-6. The regular practice of moderate intensity of exercise has been extensively recommended to counteract sustained low-grade chronic inflammation within the periphery and also within the brain 11.
Effect of Physical Exercise on Cardio – Respiratory system: Workout has many health benefits and plays an important role to reduce obesity, commodities and other ailments. Physical activity helps to improve metabolic health, decrease the risk of cardiac disorder and improve overall existence.12The prognosis of COVID 19 depends on the function and strength of cardio respiratory system of the infected individual which therefore affect the function of total system. On the basis of data analysis COVID 19 patients have a high level protein inflammatory cytokines and this is because SARS-COV2 binds with ACE2 receptor. The cytokine profile which plays as an anti-inflammatory task is induced because of workout and marks the increase of several potent anti-inflammatory cytokines like IL10, IL-1 receptor, antagonist IL1-ra and IL-6. Cytokine IL-6 increases the anti-inflammatory effects by exercise training. The anti-inflammatory response by the activation of protein inflammatory TRL4 on the surface of monocytes which help to maintain lung functioning properly is the benefit of proper workout. Daily workout helps to increase the lung functioning and lowers the risk of respiratory disorders. It also improves the maximal oxygen uptake resulting from both central and peripheral adaptations 13, 14.
Benefits and Risk related to physical exercise: There is still little known about the course of recovery, the physical capacity and physical limitations in patients who have had an active COVID-19 infection. Therefore, we should be careful while assessing and treating these patients32. Being active has been shown by many strong evidence and national health institutes to have many health benefits, both physically and mentally and it may lead to an individual live longer with less prevalence of chronic diseases and disabilities 33. In general, exercise does not provoke cardiovascular events in healthy individuals with normal cardiovascular systems. The probability of cardiac arrest or myocardial infarction is very less in individuals performing moderate intensity activity15, 25. Patients diagnosed with occult cardiovascular disease may have the risk of cardiac arrest or myocardial infarction if they perform vigorous exercise18, 19, 26, 27, 28, 29.
As a result of heavy vigorous exercise, in people having occult cardiovascular disease may result the prevalence of cardiac disease in the population. The Centers for Disease Control and Prevention currently recommends 30 min of moderate- to high-intensity exercise for at least 5 days a week for all healthy individuals. Physical fitness has multiple components, including cardio-respiratory fitness (endurance or aerobic power), musculoskeletal fitness, flexibility, balance, and speed of movement. Benefits of regular physical activity and/or exercise improve in cardiovascular and respiratory function by increasing maximal oxygen uptake resulting from both central and peripheral adaptations. The ERS/ATS suggests that patients with COVID-19 should be encouraged to do low/moderate intensity physical exercise at home (rather than high intensity physical exercise) in the first 6-8 weeks after hospital discharge, if a formal exercise assessment with measures of exertional desaturation has not been conducted 34, 35 .
Types of physical exercises: Regular physical activity is one of the most important things people can chose to improve their health. Moving more and sitting less have generous benefits for everybody, irrespective of age, sex, race, ethnicity, or current fitness level. The Centers for Disease Control and Prevention indorse physical activity according to the age on the other hand the American Physical guidelines second edition says that we can stimulate health benefits by 150-minute exercise every week by doing aerobics in a minimum of two days every week and muscle strengthening exercise for all age groups. Individuals with better capacity can do vigorous aerobic exercise by 75 minutes a week 16, 17.
Walking fast, doing aerobic exercises like swimming, and riding on a motorbike are examples of moderate aerobic exercise.6
- Examples of moderate intensity aerobic exercises are: Walking fast, doing water aerobics, riding a bike on level ground or with few hills, playing doubles tennis, Pushing a lawn mower
- Examples of vigorous intensity aerobic activity are: Jogging or running, swimming laps, riding a bike fast or on hills, playing singles tennis, Playing basketball
Disclaimer: This content is based on Guidance and Rehabilitation inside the hospital and outside, for a healthy population which has been documented to enable health professionals to make decisions in their daily clinical practice. The main goal is to homogenize care by improving upshots and enabling research. It summarizes and evaluates currently available rehab-relevant that gives indication by helping health professionals.
CONCLUSION
In a decennium, a lot of evaluation has substantiated the benefits of health related to regular physical activity. The normal functioning of the immune system is boosted with regular exercise. The anti-inflammatory influence of regular exercise is examined through various pathways; it functions as an immune system adjuvant, which improves defense reaction and metabolism. Proper physical activity helps in decreasing the need of critical care that directs us to hospital re-admission. Early mobilization and re-engagement in physical activity is important in the prevention of systemic consequences of a critical care and hospital admission. Patients should workout in proportion to their functional status.
REFERENCES
- Hawley J.A., Hargreaves M., Joyner M.J., Zierath J.R. Integrative biology of exercise. Cell. 2014:738-749.
- Petersen A.M.W., Pedersen B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005:1154-1162.
- Nieman D.C., Wentz L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019:201-217.
- Singhal T. A Review of Coronavirus Disease-2019 (COVID-19). Indian J Pediatr. 2020; 87(4):281‐286.
- Favalli EG, Ingegnoli F, De Lucia O, Cincinelli G, Cimaz R, Caporali R. COVID-19 infection and rheumatoid arthritis: Faraway, so close!.Autoimmun Rev. 2020; 19(5):102523.
- Kokkinos P. Physical activity, health benefits, and mortality risk. ISRN Cardiol. 2012; 2012:718789.
- Sun, P, Lu, X, Xu, C, Sun, W, Pan, B. Understanding of COVID‐19 based on current evidence. J Med Virol. 2020; 92: 548-551
- Zhou P, Yang XL, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020; 579:270-3.
- Pedersen BK, Febbraio MA. Muscle as an endocrine organ: focus on muscle-derived interleukin-6. Physiol Rev 2008; 88:1379-406.
- Vuori I. The cardiovascular risks of physical activity. Acta Med Scand Suppl. 1986; 711:205-14.
- Gibbons LW, Cooper KH, Meyer BM, Ellison RC. The acute cardiac risk of strenuous exercise. JAMA. 1980; 244(16):1799-1801.
- Mittleman MA, Maclure M, Tofler GH, Sherwood JB, Goldberg RJ, Muller JE. Triggering of acute myocardial infarction by heavy physical exertion: protection against triggering by regular exertion. Determinants of Myocardial Infarction Onset Study Investigators. N Engl J Med. 1993; 329(23):1677-83.
- Siscovick DS, Weiss NS, Fletcher RH, Lasky T. The incidence of primary cardiac arrest during vigorous exercise. N EnglJ Med. 1984; 311(14): 874-7.
- Thompson PD, Funk EJ, Carleton RA, Sturner WQ. Incidence of death during jogging in Rhode Island from 1975 through 1980. JAMA. 1982; 247(18):2535-8.
- Willich SN, Lewis M, Lowel H, Arntz HR, Schubert F, Schroder R. Physical exertion as a trigger of acute myocardial infarction. Triggers and Mechanisms of Myocardial Infarction Study Group. N Engl J Med. 1993; 329(23):1684-90.
- Whang W, Manson JE, Hu FB, et al. Physical exertion, exercise, and sudden cardiac death in women. JAMA. 2006; 295(12):1399-1403.
- Giri S, Thompson PD, Kiernan FJ, et al. Clinical and angiographic characteristics of exertion-related acute myocardial infarction. JAMA. 1999; 282(18):1731-6.
- American Thoracic Society; American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med 2003; 167: 211-277.
- . Hill K, Dolmage TE, Woon L, Coutts D, Goldstein R, Brooks D. Comparing peak and submaximal cardiorespiratory responses during field walking tests with incremental cycle ergometry in COPD. Respirology2012; 17: 278-284.
- Holland AE, Hill K, Alison JA, Luxton N, Mackey MG, Hill CJ, Jenkins SC. Estimating peak work rate during incremental cycle ergometry from the 6-minute walk distance: differences between reference equations. Respiration 2011; 81:124-128.
- Luxton N, Alison JA, Wu J, Mackey MG. Relationship between field walking tests and incremental cycle ergometry in COPD. Respirology, 2008; 13:856-862.
- Sillen MJ, Vercoulen JH, van ’t Hul AJ, Klijn PH, Wouters EF, van Ranst D, Peters JB, van Keimpema AR, Franssen FM, Otten HJ, et al. Inaccuracy of estimating peak work rate from six-minute walk distance in patients with COPD. COPD 2012; 9:281–288.
- Spruit MA, Vanderhoven-Augustin I, Janssen PP, Wouters EF. Integration of pulmonary rehabilitation in COPD. Lancet 2008; 371: 12-13.
- Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett DR, Jr., Tudor-Locke C, et al.
2011 Compendium of Physical Activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011; 43(8):1575-81. - Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000; 32(9 Suppl): S498-504.
- Vitacca M, Carone M, Clini EM, Paneroni M, Lazzeri M, Lanza A, et al. Joint Statement on the Role of Respiratory Rehabilitation in the COVID-19 Crisis: The Italian Position Paper. Respiration. 2020:1-7.
- Thomas P, Baldwin C, Bissett B, Boden I, Gosselink R, Granger CL, et al. Physiotherapy management for COVID-19 in the acute hospital setting: clinical practice recommendations. J Physiother. 2020; 66(2):73-82.
| Citation: Amjad Annethattil, Mirshad Ali. Ayman Sabbagh (2020). The Reality of Covid 19 Pandemic and Its Implication on Physical Activity and Exercise , ijmaes; 6 (4); 909-915. |