This book is the product of the thoughts and views of various physiotherapy teachers and clinical therapists. Every chapter in this book covers multiple neurological disorders in children, adults and elders. The clinician’s point of view on the various neurological conditions is elaborated well in this textbook. This book promotes the interest of the students and teachers to study neurology efficiently and is also helpful for them to appear in various examinations.
By
Dr. D. ANANDAN, MPT, (PhD)
Dr. B. ARUN, MPT, PhD
Dr. Jibi Paul
1Professor, Faculty
of Physiotherapy, DR MGR Educational and Research Institute, Deemed to be
University, Chennai, India
Corresponding Author:
2Physiotherapist, Ergon Physiotherapy and fitness lifestyle, Thiruvanmiyur, Chennai, India, Mail id: marsanirudh80@gmail.com
ABSTRACT
Background and objective of the study: Cricket is the most popular team sport in Indian subcontinent. Hand grip strength plays a vital part in all roles of cricket which may be associated with Body Mass Index. Grip strength is the force applied by the hand to pull or suspend from objects and is a specific part of hand strength. BMI is an attempt to quantify the amount of tissue mass (muscle, fat and bone) in an individual to categorize a person as underweight, normal weight, overweight or obese based on values. Objective of the study was to find out the association between BMI and hand grip strength in university level cricketers.
Methodology: This was an experimental and cross-sectional type study carried out at Faculty of physiotherapy, Dr. M.G.R. Educational and research institute, Chennai. Total 30 male cricketers, with age group of 18 to 25 years were included in this study. Cricketers with upper limb fractures or dislocations within one year were excluded from the study. Hand grip dynamometer, weighing machine and inch tape were the materials and measurement tools used for the study. 30 University level cricketers were divided into 4 groups, Group A, Group B, Group C and Group D based on BMI level. Body Mass Index and Hand grip strength are the outcome measures. Body mass index were calculated by measuring the height and weight of the individuals. Hand grip strength was measured for their dominant side by using the hand grip dynamometer.
Result: There is a positive association and strong correlation between Body Mass Index and Hand Grip Strength between the Groups at (r = 0.523) & (P ≤ 0.05).
Conclusion: The study concluded that cricket players with Obese Body Mass Index have more Hand Grip Strength. The study also reported a strong association of Hand Grip Strength with Body Mass Index.
Keywords: Body Mass Index (BMI), Hand grip strength, Cricketers, Hand grip dynamometer.
Received on 22nd April
2020, Revised on 22nd May
2020, Accepted on 29th May 2020
1Physiotherapy Program, Fakultas Vokasi, Universitas Kristen
Indonesia, Jakarta, Indonesia
Corresponding Author:
*Physiotherapy Program, Fakultas Vokasi, Universitas Kristen Indonesia, Jakarta, Indonesia. E-mail id: maksimus.bisa@uki.ac.id
ABSTRACT
Background of study: The strength of a straight punch, uppercut and hook is needed by a professional boxer to knock down his opponent. Therefore, in the training program for a boxer, it is necessary to analyze the biomechanical characteristics and bio motoric components, which influence its, strength, endurance, and speed by not ignoring psychological factors and the degeneration process that occurs. Degeneration is a natural process, which occurs in every individual, from the cellular level to the level of movement. It functions since 30 years of age characterized by the disappearance of the ability of cells and tissues to repair and replace themselves and maintain normal structure, as well as resulting a decrease in all body functions for 1% every year.
Methodology: This article is a qualitative description with a literature study which analyzes various theories by experts in bio motoric components, degeneration processes, and psychological factors in the form of anxiety.
Result: A balance between physical can slow the degeneration process, psychological, and environmental factors including the life style of a boxer, the factors of strength, endurance, speed, and psychological factors in the form of anxiety influence each other, both directly and indirectly against peak performance in the achievement of a boxer.
Conclusion: Periodic measurements and evaluations of bio motoric components and mental training have to be considered, so that during the golden age, boxers can achieve optimally.
Keywords: Bio motoric, degeneration process, golden age, professional boxer.
Received on 18th May 2020, Revised on 26th May 2020, Accepted on 29th May 2020
1Physiotherapy Department, School of Health Sciences, KPJ Healthcare University College, 71800 Nilai, Negeri Sembilan, Malaysia.
2Medical Imaging Department, School of Health Sciences, KPJ Healthcare University College, 71800 Nilai, Negeri Sembilan, Malaysia.
Corresponding Author:
1*Physiotherapy Department, School of Health Sciences, KPJ Healthcare University College, 71800 Nilai, Negeri Sembilan, Malaysia. Mail id: ucn.nabilah@kpjuc.edu.my
ABSTRACT
Background and objectives: Dynamic warm-ups prepare the body for activity by helping to increase blood flow and muscle temperature. By calculating the muscle elongation, muscle thickness and pennation angle, it will show the effectiveness of the dynamic elongation task. Ultrasound imaging involves the use of a transducer (probe) and ultrasound gel placed directly on the skin. Ultrasound images of the musculoskeletal system provide the pictures of muscles, tendons, ligaments, joints, and soft tissues throughout the body. Therefore, this study aimed to determine the changes in the muscle tendon unit displacement among healthy male subjects in dynamic task of a gastrocnemius muscle.
Methods: This experimental studywas participated by 32 healthy male subjects among KPJUC students. Musculoskeletal Ultrasound (MSK Ultrasound) performed to collect the databefore and after the dynamic task. The measurement was taken for pre and post dynamic elongation task. Paired sample t-test and paired samplecorrelation were used as a statistical analysis.
Results: This study shows that there is a changes in muscle architecture after the dynamic elongation task. There is significant difference in pennation angle and muscle elongation between pre dynamic elongation task and post dynamic elongation task. For muscle thickness, there is no significant different between pre dynamic elongation task and post dynamic elongation task.
Conclusion: There is a change in muscle tendon unit displacement for gastrocnemius muscle between pre dynamic elongation task and post dynamic elongation task and the obvious changes can be seen in pennation angle of the muscle. Dynamic elongation task seems to be an effective stretching for rehabilitation purposes because it can produce the changes in muscle architectures.
Received on 20th February 2020, Revised on 26th February 2020, Accepted on 29th February 2020. DOI:10.36678/ijmaes.2020.v06i01.007
INTRODUCTION
Abnormal muscle tendon
elongation occurs when the injury to the muscle happens. For management and
prevention of the injuries there is an important components to understand of
muscle tendon elongation. During any sort of movement, muscle tendon unit is
the one which generates force production of a particular muscle 1.
The force production
can be either active or passive force, which relies on length of the muscle. It
is based on the length amount of sarcomeres will be recruited. There is no
previous study examined the pattern of elongation and structural changes at the
level of muscle tendon unit. It is believed that understanding such mechanism
of muscle tendon unit explains the science behind the injury mechanism. The
regular elongation to a muscle contribute to a defined movement of muscle tendon
and joints 2, 3.
Ultrasonography is a
valid tool which shows any changes in muscle tendon length properties. The
drawback of the usage of ultrasonography tool is its unclear how the elongation
mechanism occurs in dynamic elongation. Therefore, uncertain prevails on types
of elongation task is required for rehabilitation outcome. Thus, there is a
need to understand the elongation mechanism for dynamic task on a muscle. Muscle
imaging was used to show that the ultrasonography could properly estimate muscle
activity. They measured architectural parameters which included the pennation
angle, fascicle lengths and the muscle thickness. Ultrasonography is used to
understand biological and bioelectrical characteristics of muscle. An
ultrasound is a proper non-invasive real time imaging for muscle structures.
Collected data will answer properties of the muscle tendon unit elongation
mechanism through displacement of the tendon. This study prescribes either of
the elongation task for a variety of patients as well for normal subjects in
order to improve social well-being 4, 5.
METHODOLOGY
This experimental
study was conducted in KPJ Healthcare University College (KPJUC), Nilai. A
total of 32 healthy individuals was recruited and subjected to undergo the
dynamic elongation technique with enough rest periods. The normal healthy
individuals for this study was identified among the students who are studying
in KPJUC. The subject recruitment were based on the established inclusion
criteria.
The measurement was
taken for pre dynamic elongation task and post dynamic elongation task. Real
time ultrasound imaging (Mylab Touch, Esaote, Italy) 15-MHz linear type probe
with 38 mm wide field of view (FOV) were used to measure tendon displacement,
muscle thickness, pennation angle and muscle elongation. Another tool is
treadmill machine, which is used to do the warming up maneuver and the
metronome for monitoring the number of beats while performing dynamic
elongation.
Subjects were asked to
walk in the treadmill for 5 minutes as a warming up. Then, the subjects made to
perform dynamic elongation on their dominant legs only then they were stand
with dominant leg and to raise the entire foot off the floor, which lead to hip
flexion. Then the subjects were instructed to perform active movement of foot
to a rhythm of 60 beats per minutes (60 BPM) with the help of metronome and
each movement was performed for 1 second. The dynamic elongation was done for
30 second and will be repeated for 5 times. Elongation maneuver pre and post
measurement of the subject’s muscle-tendon unit displacement, fascicle length
and pennation angle were obtained.
The measurement
starting on 30 mm below the fossa popliteal and about 20 mm medial of the line
separating the medial and lateral gastrocnemius muscle. In this location the
muscle fibers have a distinctly visible pennation angle and muscle structure
seems to be well-define. Each subject instructed to stand upright with feet
parallel, looking at the same point on the front wall. Prior to stretching, the
middle of the monitor display was marked with a white string. A rectangular
plastic foam frame (proximal frame) through which the ultrasound probe could
pass was placed onto the right calf of each subject to obtain measurements from
the same location, a quarter proximal to the distance between the popliteal
crease and center of the lateral malleolus.
Myotendinous junction
(MTJ) was defined as where the superficial and deep aponeuroses of medial
gastrocnemius (MG) met. Another rectangular plastic foam frame (distal frame)
was put on the right calf where the middle of the MTJ of the MG aligned with
the midline of the ultrasound monitor, which was defined as the baseline of the
MTJ. After the dynamic stretching, the probe was set in the same place and the
image was taken. The MTJ then calculated by measuring the distance between the
white reference line and the new MTJ position. The proximal displacement of the
MTJ will show in ultrasound image. The pennation angle of the MG and fascicle
length (Lf) were also assessed from the images, which were taken at the
proximal frame. The pennation angle of MG was measured as the angle of
insertion of the muscle fiber fascicles into deeper aponeurosis. Fascicle
length (Lf) was defined as the length of the fascicular path between the
insertions of the fascicle into the upper and deeper aponeuroses.
RESULTS
A total of 32 healthy
young man participated in the study. The demographic data obtained include male
subjects who are aged between 20 – 25 years old. The male subjects who does not
have any lower limb injury such as ligament or muscle tear and who have normal
Body Mass Index which in range 18.5-24.9𝑘𝑔/𝑚2. Subjects was
categorized into two groups; right dominant leg and left dominant leg.
Majority of the healthy
young man participated were right dominant leg (94%), and the remaining healthy
young man were left dominant leg (6%). The p value for muscle elongation (p=0.00) which is<0.05, therefore
reject the null hypothesis and there is a significant difference. There is a
significant difference of mean score between Pre Muscle Elongation and Post
Muscle Elongation after an intervention. The significant relationship of score
between Pre Muscle Elongation and Post Muscle Elongation which is strong
(0.814).The p value for muscle thickness (p
= 0.606)>0.05, therefore not reject the null hypothesis and there is no
significant difference.
There is no significant difference of mean score between Pre Muscle Thickness and Post Muscle Thickness after an intervention. The significant relationship of score between Pre Muscle Thickness and Post Muscle Thickness, which is strong (0.776).The p value for pennation angle (p = 0.012)<0.05, therefore reject the null hypothesis and there is a significant difference. There is a significant difference of mean score between Pre Pennation Angle and Post Pennation Angle after an intervention.
The significant relationship of score between Pre Pennation Angle and Post Pennation Angle, which is strong (0.711).
Table 1. Score Pre-Muscle Elongation and Post Muscle Elongation Table 2. Correlations Pre-Muscle Elongation and Post Muscle Elongation Table 3. Score Pre-Muscle Thickness and Post Muscle Thickness Table 4. Correlations Pre-Muscle Thickness and Post Muscle Thickness Table 5. Score Pre-Pennation Angle and Post Pennation Angle Table 6. Correlations Pre-Pennation Angle and Post Pennation Angle
DISCUSSION
The age of subjects
was fixed in the range of 20 to 25 years old because of the composition of
Skeletal Muscle Mass might be stable during the age of 20 to 40 years old and
at the age of 45 years old it begins to decrease significantly. Due to
decreases in the amount and diameter of muscle fibers it caused the decrease in
Skeletal Muscle Mass occurs with aging process as a physiological change. Dominant
leg for the subjects also have to consider because of the scanning need to be
done on the dominant leg. Leg dominance has been determined by which hand
dominant is dominant. If the person is left-handed, the he must be left leg
dominant6.
The definition of
muscle power is the amount of work a muscle can produce per unit of time. High
muscle power understood as the capacity to exert high levels of strength as
quickly an explosively as possible. No statistical difference in maximal power
between the dominant and non-dominant legs in healthy young adults, whether
they are non-athletes or professional, single-leg-dominant athletes and the
reason younger group of healthy man was chosen in my study is because muscular
power development reaches its peak between 18 and 30 years of age, so
theoretically I had the best chance to find asymmetries in this age range7.
The results shows the
dynamic elongation task is an effective stretching since there is a different
length of gastrocnemius muscle between pre and post, this results supported by
the study of Knudson et al., 2006 which is when a muscle or muscle group is
passively stretched using techniques like in static, dynamic, or proprioceptive
neuro-muscular facilitation (PNF) stretching there might be some short-term
changes in the muscle. The short-term or acute effects of stretching on muscle
relate to the initial performance changes in the first few hours after
stretching.
Therefore, the acute
effects following stretching then depends on the biomechanical performance
variables like a range of motion (ROM) have been shown to improve following
stretching, while some of it appear to be unaffected such as stiffness and
others are significantly reduced which means strength. The acute effect of the
stretching on flexibility is clear. Stretching an acute increase in joint range
of motion that tends to persist for 60 to 90 minutes. For rehabilitation
purposes, passive stretching of the injured muscle helps elongate the maturing
inter-muscular scar and prepares the muscle for strengthening. Dynamic training
exercises can be added in a consecutive manner as each type of exercise is
completed with painless to the patient8.
The muscle thickness
slightly decreased after stretching was performed. A study from Simpson, Kim,
Bourcet, Jones &Jakobi, et al. (2017) main findings were novel to human
stretch training studies and included an increase in the thickness of
gastrocnemius muscle, and increase in the fascicle lengths at both the MTJ and
muscle belly with extent of the lengthening greater in the lateral
gastrocnemius muscle compared with medial gastrocnemius muscle. The findings
were contradict with the results from this study where the muscle thickness was
slightly decreased.
The pennation angle
was slightly decreased after the dynamic elongation task was performed. A
review of literature of pennation angle and fascicle length of human skeletal
muscles to predict the strength of an individual muscle using Real-Time
Ultrasonography. found that The pennation angle defined as the pattern of
arrangement of muscle fibers in relation to the axis of the force generation by
the same muscle which is crucial component to determining muscle performance9.
The only study we
found in the literature that investigating the effects of dynamic stretching
exercises on muscle morphology demonstrated that dynamic stretching performed
before exercise activities was not effective on fascicle length and pennation
angle of the gastrocnemius muscle10.
In this study, the
correlation between each parameters were not investigated. Therefore, it is
recommended for future research to measure the correlation between each parameters.
The age range of this study was limited from 20 years old to 25 years old, to
overcome this limitation future study should wide the age gap.
Ethical Clearance: Received approval letter from
the Research Ethics Committee, School of Health Sciences, KPJ Healthcare
University College with reference number:
KPJUC/RMC/ MPT/ EC/ 2018 /129 dated 19/03/2018.
Fund for the
study: Research
Management Center, Department of Physiotherapy, School of Health Sciences, KPJ
Healthcare University College, Malasia.
Conflict of Interest: All authors have no conflict of
interest to declare on conduct of this study.
CONCLUSION
The aim of this study
is to determine the changes in the muscle tendon unit displacement among
healthy male subjects in dynamic task of a gastrocnemius muscle. The data was
collected on pre dynamic elongation task and post dynamic elongation task. The
investigation of this study show that there is a changes in muscle tendon unit
displacement for gastrocnemius muscle between pre dynamic elongation task and
post dynamic elongation task and the obvious changes can be seen in pennation
angle of the muscle. The results may be influence by subject BMI, height,
weight and daily lifestyle. Moreover, for rehabilitation purposes, this dynamic
elongation task seem to be an effective stretching because it can produce the
changes in muscle architectures.
REFERENCES
Hodges, P., Pengel, L., Herbert, R. and G andevia, S. (2003). Measurement of muscle contraction with ultrasound imaging. Muscle & Nerve, 27(6), 682-692.
Vaisman, A., Guiloff, R., Rojas, J., Delgado, I., Figueroa, D., & Calvo, R. (2017). Lower limb symmetry: Comparison of muscular power between dominant and nondominant legs in healthy young adults associated with single-leg-dominant sports. Orthopaedic Journal of Sports Medicine, 5(12), 232-236.
Knudson, Duane (2006). The biomechanics of stretching. Journal of Exercise Science and Physiotherapy, Vol. 2 : 3-12.
Rekabizadeh M, Rezasoltani A, Lahouti B, Namavarian N.(2016). Pennation Angle and Fascicle Length of Human Skeletal Muscles to Predict the Strength of an Individual Muscle Using Real-Time Ultrasonography: A Review of Literature. J Clin Physio Res, 1(2): 42-48.
Samukawa, M., Hattori, M., Sugama, N., & Takeda, N. (2011). The effects of dynamic stretching on plantar flexor muscle-tendon tissue properties. Manual Therapy, 16(6), 618-622.
Miura, K., Yamamoto, M., Tamaki, H., &Zushi, K. (2010). Determinants of the Abilities to Jump Higher and Shorten the Contact Time in a Running 1-Legged Vertical Jump in Basketball. Journal of Strength and Conditioning Research, 24(1), 201-206.
Wattimena, R., Vitriana, V., &Defi, I. (2017). Correlation between body mass index, gender, and skeletal muscle mass cut off point in Bandung. International Journal of Integrated Health Sciences,5(2), 47-51.
Brukner, P., & Khan, K. Brukner& Khan’s (2002).Clinical sports medicine. Revised 2nd ed. McGraw-Hill, Australia.
Zhou, G., Chan, P. and Zheng, Y. (2015). Automatic measurement of pennation angle and fascicle length of gastrocnemius muscles using real-time ultrasound imaging. Ultrasonics, 57, 72-83.
Simpson, C., Kim, B., Bourcet, M., Jones, G., & Jakobi, J. (2017). Stretch training induces unequal adaptation in muscle fascicles and thickness in medial and lateral gastrocnemii. Scandinavian Journal of Medicine & Science in Sports, 27(12), 1597-1604.
Citation: Nabilah Ahmad, Siti Aishah Abdullah Suhaimi, Najiah Anuar (2020). Effect of dynamic stretching on elongation of Gastrocnemius muscle, International Journal of Medical and Exercise Science, 6 (1): 713-719.
V. P. Lakshmikanth1, T. Yamini2, N. M. Basheer Ahamed3
Authors:
2B.P.T. Graduate, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India.
3 Professor, JDT Islam College of Physiotherapy, Kozhikode, Kerala, India
Corresponding Author:
1Asst. Professor, JDT Islam College of Physiotherapy, Kozhikode, Kerala, India. Mail id: laksh.anee@gmail.com
ABSTRACT
Background: In recent years, the number of smart phone users has progressively increased worldwide. Using smart phone for prolonged time will cause faulty posture or poor posture such as forward head posture and rounded shoulders.The structural problems caused by faulty posture can also lead to respiratory dysfunction. The objective of the study was to determine the effect of exercise on posture and respiratory function among smart phone users.
Methods: This study was an experimental with conventional type. The study was carried out in faculty of physiotherapy at A.C.S Medical College And Hospital. 100 samples were taken and assessed posture and respiratory function. Subjects with poor posture and respiratory dysfunction were trained with exercise for 4 weeks. Both male and female aged between 18 -25 years using smart phone more than 4 hours were included in the study. Individuals with any cervical deformity were excluded in the study. Craniovertebral angle, Scapular index and PEFR were the outcome measures used in this study.
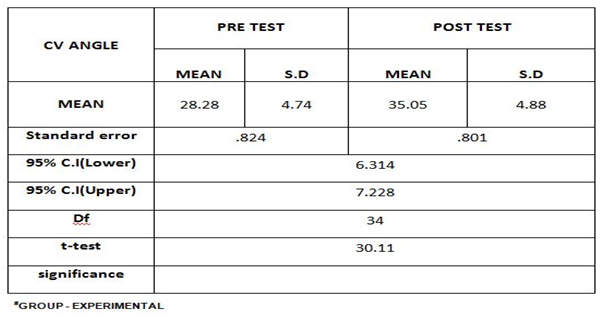
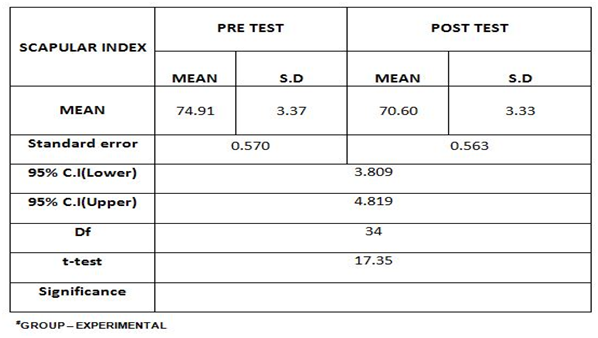
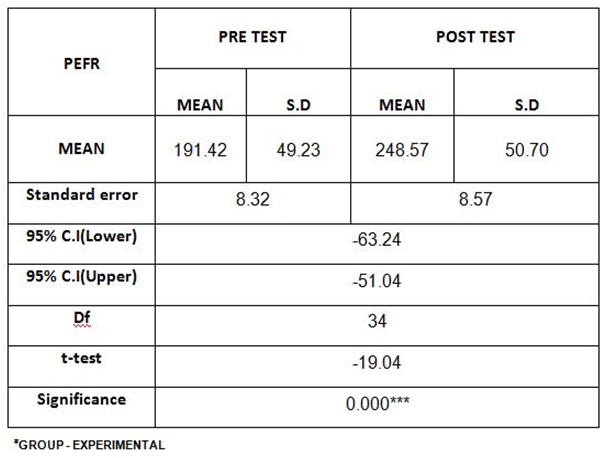
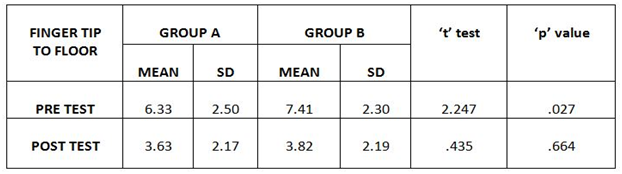
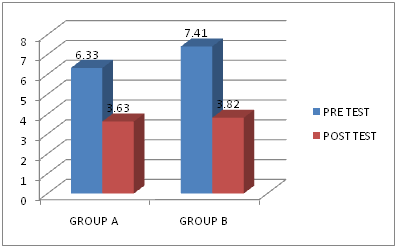
Results: On comparing the mean values of Pre Test & Post Test on Craniovertebral Angle, it shows significant difference between Pretest (28.28) & Posttest (35.05) at P ≤ 0.001. On comparing the Pre Test & Post Test on Scapular Index, it shows significant mean difference between Pretest (70.60) & Posttest (74.91) at P ≤ 0.001. On comparing the Pre Test & Post Test on Peak Expiratory Flow Rate(PEFR), it shows significant mean difference between Pretest (191.42) & Posttest (248.57) at P ≤ 0.001.
Conclusion: The study concluded that stretching and breathing exercise has considerable effects in improving the posture and respiratory function among Smartphone users.
Received on 15 th February 2020, Revised on 22nd February 2020, Accepted on 29th February 2020. DOI:10.36678/ijmaes.2020.v06i01.006
INTRODUCTION
In the past decade, there has been a rapid increase in the use of mobile devices, particularly Smartphone for communication, gaming and internet browsing. A mobile phone is no longer just a telephone and has become an integral part of modern living for many people. Mobile phone production rise from 450 million per year in 2011 to 984 million per year in 2013 and more than 50% population in many western countries, as well as in Taiwan, own mobile phones 1,2.
Smartphone have become the essential mobile devices in our daily living and people demonstrate different posture while using Smartphone. Smartphone have become not only an example of modern high-tech equipment, but also a daily necessity. Smartphone, unlike computer features a small screen that is likely to induce a more slouched posture toward a line of sight below eye level 3.
If people have used a smart for a long time, a video terminal such as a Smartphone might therefore induce an improper posture or slouched posture or rounder shoulders. Forward head posture is defined as a posture that adopts upper cervical extension and lower cervical flexion 4, 5.
Forward neck posture is become increasingly common, as it is becoming leaning forward posture, particularly with popularization of smart phones. Forward head posture is one of the most common deviation from normal cervical posture and may lead to a n increase in gravitational load and mechanical stress to cervical facet joints, altered neck extensors muscles activity and length of cervical muscles6.
In recent years, the number of smart phone users has progressively increased worldwide. Using smart phone for prolonged time will cause faulty posture or poor posture such as forward head posture and rounded shoulders.The structural problems caused by faulty posture can also lead to respiratory dysfunction. The objective of the study was to determine the effect of exercise on posture and respiratory function among smart phone users.
METHODOLOGY
This study was an experimental with conventional type. The study was carried out in faculty of physiotherapy at A.C.S Medical College And Hospital. 100 samples were taken and assessed posture and respiratory function. Subjects with poor posture and respiratory dysfunction were trained with exercise for 4 weeks. Both male and female aged between 18 -25 years using smart phone more than 4 hours were included in the study. Individuals with any cervical deformity were excluded in the study. Craniovertebral angle, Scapular index and PEFR were the outcome measures used in this study.
Procedure: Subjects using smart phones for more than 4 hours were selected based on inclusion and the exclusion criteria. They were assessed for forward head posture and respiratory dysfunction by using craniovertebral angle and peak flow meter.
The subjects were asked to sit comfortable on back supported arm less chair with both feet flat on floor, hip and knees positioned at 90 degree angle and buttock positioned against the back chair. The subjects were asked to rest their hands on their lap and to keep their shoulder against the back of the chair. Adequate exposure of neck up to shoulder level to clearly define anatomical landmark was done. The most prominent spinous process at the base of the cervical spine was palpated. Skin over the anatomical landmark was wiped with cotton soaked in spirit to remove skin secretions for proper fixation of adhesive markers. Anatomical landmarks were marked with marker pen, thereafter adhesive markers were fixed over the anatomical landmark. Then the craniovertebral angle was measured by angle between midpoint of the adhesive marker at the tragus of right ear and midpoint of the reflective marker at C7.
After the subjects were assessed for Scapular index by using inch tape. The resting position the scapula was determined by measuring the distance from the midpoint of the sternal notch to the medial aspect of the coracoids process (the length of the chest side) and the horizontal distance from the posterolateral angle of the acromion to the thoracic spine (the length of the back side).
Then the subjects were assessed for respiratory functions by peak flow meter. By blowing hard through a mouth piece on one end the peak flow meter can measures force air in liters per minute and gives the reading on a built in numbered scale.
EXERCISE INTERVENTION
1. For posture deviation:
Forward head posture:
Chin tuck exercise: Ask the subject sit upright, gently tuck the chin and to feel a gentle lengthening sensation at the back of the neck. Make sure that the eyes and jaw stay level and move the head horizontally backwards and hold for 5 seconds with 30 repetitions.
2. For Rounded shoulder:
Stretching exercises:
Pectoralis stretch: Ask the subject to stand in the middle of a door way with one foot in front of the other and bend the elbow to 90-degree angle and place the forearms on each side of the doorways. And shift weight on to the front leg, leaning forward, until feel a stretch in the chest muscles.
Upper trapezius stretch: Ask the subject to sit upright, tuck the chin in to your chest and look down. Place the palm of the hand on the back of the head and press downward. Hold for 30 seconds. Then rotate the right ear down slightly, maintaining the download pressure with the hands, to stretch the left side. Hold for 30 seconds. Then rotate the left ear down, maintaining download pressure to stretch the right side. Hold for 30 seconds. Repeat the sequence for three times.
3. For Respiratory Dysfunction:
Breathing exercise:
Diaphragmatic breathing: Ask the subject to sit comfortably, with the knees bent and the shoulders, head and neck relaxed. Breathe in slowly through the nose.so that the stomach moves out against the hand. The hand on the chest should remain as still as possible. Place one hand on the upper chest and the other just below your rib cage. This will allow to feel the diaphragm while breathing. Tighten stomach muscles, letting them fall inward while exhale through pursed lips. The hand on the upper chest must remain as still as possible.
Pursed lip breathing: ask the subject to sit comfortably, and to relax the neck and shoulder muscles and breath in for 2 seconds through the nose, by keeping the mouth closed and then instructed to breath out twice through pursed lips.
Data Analysis : The collected data were tabulated and analyzed using both descriptive and inferential statistics. All the parameters were assessed using statistical package for social science (SPSS) version 24. Paired t-test wasadopted to find the statistical difference within the group.
Table-1. Comparison of craniovertebral angle between pre test and post testTable-2. Comparison of scapular index between pre test and post testTable-3. Comparison of peak expiratory flow rate(PEFR) between pre test and post test
RESULTS
On comparing the Mean values of Pre Test & Post Test on Craniovertebral Angle, it shows highly significant Mean differences between Pretest (28.28) & Posttest (35.05) at P ≤ 0.001.
On comparing the Mean values of Pre Test & Post Test on Scapular Index, it shows highly significant Mean differences between Pretest (70.60) & Posttest (74.91) at P ≤ 0.001.
On comparing the Mean values of Pre Test & Post Test on Peak Expiratory Flow Rate(PEFR), it shows significant Mean difference between Pretest (191.42) & Posttest (248.57) at P ≤ 0.001.
DISCUSSION
The present study was conducted to find out the effect of exercise on posture and respiratory function among smartphone users. The study measured CVA, SI and PEFR as parameters to demonstrate the effect of prolonged smartphone use on change in posture and respiratory function.
Previous study performed in other context and population, support our results FHP and rounded shoulder after an training protocol7,8.
Studies have reported decreased PSs in elite swimmers after an 8 week intervention including stretching of anterior musculature and strengthening of scapula stabilizers 9, 10.
This study indicates that a targeted exercises program, can result in the improvement of posture and respiratory functions. The mean values of CVA, SI and PEFR were analyzed 11,12.
The pre-test mean value of CVA was 28.28 and the post-test mean value was 35.05.The pre-test mean value of SI was 74.91 and the post-test mean value was 70.60.The pre-test mean value of PEFR was 191.42 and the post-test mean value was 248.57.
The result showed that statistically highly significant difference in the values of CVA, SI and PEFR.
Limitation of the study: Small sample size was analysed in this study. The duration of the study was short. Long term follow up of the subject was not possible.
Ethical Clearance: Ethical clearance has obtained from Faculty of Physiotherapy, DR. MGR Educational and Reasearch Institute, Chennai to conduct this study with reference number: IV B/ PHSIO/ IRB/ 2017-2018dated 08/01/2018.
Conflict of interest: There was no conflict of interest to conduct this study.
Fund for the study: It was aself financed study.
CONCLUSION
The study concluded that stretching and breathing exercise has considerable effects in improving the posture and respiratory function among Smartphone users.
REFERENCES
Liang H-W et al, (2016). Mobile phone use behaviours and postures on public transport systems. PLOS ONE 11(2): 0148419.
Sang In Jung et al, (2016). The effect of smartphone usage time on posture and respiratory function. J. Phys. Ther Sci. 28: 186-189.
Yong- Soo Kong et al (2017). The effect of modified cervical exercise on smartphone users with FHP, J. Phys. Ther Sci., 29(2): 328-331.
Jung-Ho Kang et al (2012). The effect of the forward head posture on postural balance in long time computer based worker; Ann Rehabil Med., 36(1): 98-104.
Korooshfard N et al, (2011). Relation of self esteem with FHP and rounded shoulder procedia soc., Beh. Sci., 15: 3698-3702.
Do Youn Lee et al (2017). Changes in rounded shoulder posture and FHP according to exercise methods. J. Phys. Ther Sci., 29(10): 1824-1827.
Greig AM et al, (2005). Cervical erector spinae and upper trapezius muscle activity in childernusing different information technologies. Phy Ther., 91.119-126.
Lynch SS et al (2010) The effects of exercises intervention on FHP and rounded shouder posture in elite swimmers. Br. J Sports Med., 44: 376-381.
Okuro RT et al (2011). Mouth breathing and forward head posture: effects on respiratory biomechanics and exercise capacity in children. J Bras pnemol., 37:471-479.
Repacholi MH. (2001). Health risks from the use of mobile phones. Toxicol Lett., 120 (1-3) : 323-31.
Hakala P T, Rimpela A H, Saarni L A, Salminen J J. (2006). Frequent computer-related activities increase the risk of neck-shoulder and low back pain in adolescents. Eur J Public Health., 16(5): 536-41.
Kim GY, Ahn CS, Jeon HW, Lee CR. (2012). Effects of the Use of Smartphones on Pain and Muscle Fatigue in the Upper Extremity. J Phys Ther Sci., 24(12): 1255-8.
Citation:
V. P. Lakshmikanth, T.Yamini, N.M. Basheer Ahamed (2020). Effect of exercise on posture and respiratory function among smartphone users, International Journal of Medical and Exercise Science, 6 (1): 706-712.
Authors: 2Lecturer,Post Graduate Studies, Master of Management Program, Universitas Kristen Indonesia, Jakarta, Indonesia 3Lecturer, Faculty of Vocational Studies, Physiotherapy Program, Universitas Kristen Indonesia, Jakarta, Indonesia Corresponding Author: 1Lecturer, Faculty of Vocational Studies, Physiotherapy Program, Universitas Kristen Indonesia, Jakarta, Indonesia, email : novlinda.manurung@uki.ac.id
ABSTRACT
Background: Physiotherapy service standards are used as a basis for risk management in preparing strategies to anticipate unexpected events that appear in the management of the physiotherapy process. This research aims to improve the quality of physiotherapy services through the calculation of the risk of the physiotherapy process and risk mitigation measures using the Workload Indicator Staffing Need (WISN) method from the World Health Organization (WHO).
Methods: The research uses the stages of risk management as a method of analysis and WISN as a method for risk mitigation. Risk analysis begins with the identification of risks and then measures the risks by calculating the probabilities and impacts of these risks and designing risk management as mitigation.
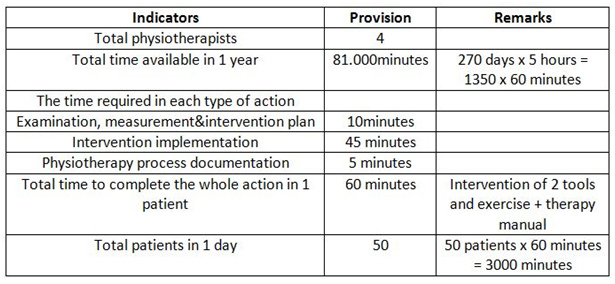
Results: Based on the research that has average 50-60/day, which is not proportional to the number of only 4 physiotherapists. In addition, there is a lack of physiotherapy intervention tools.
Conclusion: In this research it has concluded that to improve the qualityof physiotherapy services must be done by making policies to mitigate unexpected events and reducing the probabilities such as: increasing the number of physiotherapists and arranging the separation schedule of examination days for physiotherapy been done, events with the highest risk are found in the stages of examination and measurement, documentation, and physiotherapy intervention where there is an opportunity to reduce the type and duration of long or unsuccessful healing interventions. The trigger for the occurrence of potential risks is the number of patients on measurements from intervention days and increasing the number of physiotherapy intervention tools.
Keywords: Physiotherapy Process, Workload Indicator of Staffing Need, Risk Management
Received on 15 th February 2020, Revised on 22nd February 2020, Accepted on 29th February 2020, DOI:10.36678/ijmaes.2020.v06i01.005
INTRODUCTION
The
role of human resources (HR) in a company or hospital is very important because
HR is the main implementer of activities in order to meet the objectives of the
company or hospital 1,2,3.
One
of the human resources in the hospital is physiotherapists4,5. As a
profession that carries out physiotherapy service activities, a physiotherapist
uses references as the basis for carrying out their duties and functions as
stipulated by the Minister of Health in the Regulation of the Minister of
Health of the Republic of Indonesia number 65 of 2015 concerning physiotherapy
service standards containingthe duties and functions of a physiotherapist as
well as physiotherapy personnel service standards in the form of the stages of
the process of implementing physiotherapyor physiotherapy action is a normal
service of a physiotherapist, which can then be calculated and determined as a
guide or measuringtool to determine the need for physiotherapists in hospitals7.
Fulfillment
of physiotherapy human resources in health care facilities is based on workload
analysis and/or the ratio of patient/client services per workday, i.e. 1
physiotherapist : 8-10 patients/clients per workday taking into account the
need for appropriate qualifications of physiotherapists 6.
Based
on physiotherapy service standards, the elements of the physiotherapist’s
workload in the physiotherapy process should be observed. In the physiotherapy
process management, there are several stages of action, such as: Assessment of
the Patient, Making of Diagnosis, Intervention Planning, Intervention,
Evaluation/Revaluation, Communication and Education as well as Documentation 4,6.
From assessment to evaluation, the physiotherapist must also carry out the
report writing stage simultaneously which serves to document the data and
becomes the basis and the most important part in fulfilling the final stage
called physiotherapy documentation 6. The physiotherapy
documentation process serves as an integrated information tool from the
physiotherapist to all health workers involved in the process of handling a
patient.
Documentation
is also an accurate tool in providing work quality information as well as a
legal protection tool for a physiotherapist. With the implementation of the
National Health Insurance system by the government to realize the mandate of
the 1945 Constitution no. 28 part H, there is an increase in the number of
patients in the medical rehabilitation installation unit with a physiotherapist
as a service provider7. Increase in the number of patients is
closely related to an increase in the amount of service time per day in the
hospital 9. To avoid decreasing quality of services with an increase
in the number of patients, it is necessary to analyze the need for
physiotherapists in connection with the workload and the length of time of the
implemented physiotherapy process in one workday8.
The
need for physiotherapists can be analyzed by measuring the physiotherapy
workload using the “Workload Indicator of Staffing Need”(WISN) method 7,10.
The WISN method uses a measure or working time as an assessment indicator at
each stage of the human resource working process7.WISN is a tool
used to measure the workload of health workers released by WHO7.
This method is used to set the appropriate standard of the number of workers
needed in each working unit 10. Meeting the appropriate workforce
requirements will improve performance, service quality and service risk
mitigation.
A
physiotherapist’s workload isall activities carried out by the physiotherapist
in the course of their assignment in a physiotherapy service unit. The method
that can be used as a measurement for health workers is the Workload Indicator
of Staffing Need. This tool in its application uses analysis of the length of
time in carrying out a work activity of each HR in accordance with their duties
and functions 11. The WISN method helps to determine how many
specific types of health workforce are needed according to the workload
provided or available at a health facility and measures the workload pressure
of a health worker at that health facility 10,11.
The guidelines for using WISN software explain
the description of the application, and provide step-by-step instructions to
meet or complete a variety of tasks or data requirements. The tasks or data to
be analyzed and measured in WISN consist of: facilities, labor facilities, time
needed to do the work, workload statistics, activity standards, labor
comparisons, and calculation of remuneration costs10.
The
WISN method is a tool stipulated in the Minister of Health Decree Number: 81/ MENKES/
SK/ 2004 concerning Guidelines for Preparation of Health HR Planning at
Provincial, Regency/City and Hospital Levels to calculate HR needs at
Hospitals.Through the application of the WISN method, it is likely to know the
working unit and its HR categories, available working time for each HR
category, workload standards, tolerance standards, quantity of main activities
and finally, the HR needs in the working unit can be known 12.
Through
the above review, this research aims to analyze the risks of the physiotherapy
process by analyzing the need for human resources, which in this case are physiotherapist
in order to prevent the risks that may occur.
RESEARCH METHODOLOGY
This research is descriptive qualitative, by measuring the probabilities and impacts of time reduction in the physiotherapy process and measuring the need for human resources based on the Workload Indicator of Staffing Need method for risk mitigation.
a. The Risk Management Analysis Technique is carried out by means of; risk identification, risk measurement and risk management.
b. Population
and Sampling Technique;
The population of the research is the
physiotherapists and medical records of patients in 2017 in the period of 3
months from April to June 2017.
The sampling technique is all 4 physiotherapists
and data of medical records. The research samples are medical recordswith the
data of 62 patients per day.
c. Place and Unit of Research.
The
place of research is one of the general hospitals of Universitas Kristen
Indonesia in the medical rehabilitation installation unit, physiotherapy unit,
Jakarta, Indonesia.
d. Data and Sources of Data
1. Data of
physiotherapy process (medical records)
2. Data of probabilities of unexpected events
(physiotherapy questionnaire)
3. Data of
physiotherapy process impacts (review of medical records)
e. Data Collection Technique.
The instrument used was a questionnaire
to physiotherapists, interviews and observations of physiotherapy management
directly and through medical record documentation. The physiotherapy service
process data is taken from the physiotherapy process in the hospital for 3
months from April to June 2017.
1) Observation
This method is done by finding and
collecting data directly from the source by direct research on the
physiotherapy process in the hospital.
2) Interview
In order to obtain complete information
in this study, the authorsconducted a question and answer processwith
physiotherapists directly about the physiotherapy service process in the
physiotherapy unit.
3)
Documentation of physiotherapy process results in the hospital
In this process, various physiotherapy
service activities are recorded and documented as evidence of the
implementation of the physiotherapy process.
4) Library Study
This is the search for data with the
library study method as a guideline for collecting and reviewing existing
data.The library study method is done by reading the literature relating to
government regulations, especially those of the minister of health concerning
the physiotherapy service process standards in hospitals, theories about the
workload measuring tools and the need for health workersin the hospital, notes
and books relating to the risks of health services to produce maximum quality
health services.
RESULTS AND DISCUSSION
The
results of analysis and observation of the physiotherapy process in four
respondents showed
that
the management of physiotherapy has about 80% of direct contact with patients
where the time is included in the weight category or an indication of danger.
Based
on the time calculation in the physiotherapy workload diagram it appears that
the average time required is 101.75 minutes by a physiotherapist to carry out
physiotherapy services for one patient. The time is quite long with the number
of 40-60 patients per day, an indication of the physiotherapy process with the
risk of danger. These results are in Table 3.
Observation of Physical Examination Sheets
of Physiotherapy and Interview
Reports
on the results of examination and measurement are not written in full with the
type of examination and value of the measurement results before and after
therapy as well as the results of the evaluation. The process of implementing
physiotherapy interventions is not carried out in full according to the
intervention plan because it is limited by the quota of funding for treatment
of patients by the National Health Social Security Board, the waiting time for
therapeutic measures and the availability of intervention equipment facilities
that are not proportional to the number of patients who need the same tools and
also the implementation of interventions that takes a minimum of 15 minutes per
tool.
The
biggest condition is musculoskeletal cases and in the next sequence is
neuromuscular condition, where both conditions require at least 45 minutes of
physiotherapy services for long-standing patients with musculoskeletal problems
who are only undergoing therapy but still need to undergo a momentary
examination, while patients with neuromuscular problems must get complete
exercise that takes a minimum of 60 minutes.
In
contrast to old patients who come only to continue therapy, patients who have
just arrived for the first time will take longer examination if the
physiotherapy process is carried out in full according to the physiotherapy
service standards.
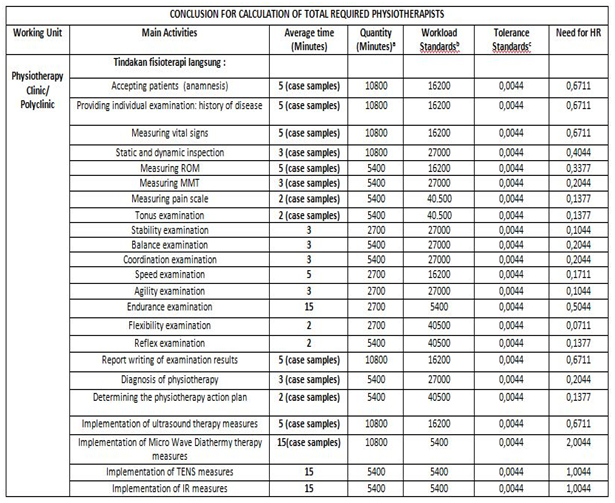
Analysis of Workload Indicator of Staffing Need
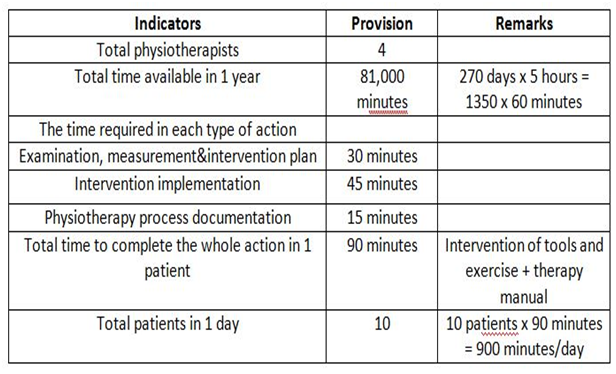
Based on the physiotherapy workload that is in the hospital’s medical rehabilitation installation unit, the need for physiotherapists must be calculated in order to achieve optimal performance in the implementation of physiotherapy services. The measuring instrument used to analyze the need for physiotherapists is WISN with a measurement method using components or elements of assessment, such as: the number of physiotherapists available to carry out activities as physiotherapists, the time required for each type of action or physiotherapy work activity, the total time available for each physiotherapist, the amount of time needed to complete the actions carried out by the physiotherapist and the number of patients and patient visits (Table 1 and Table 2).
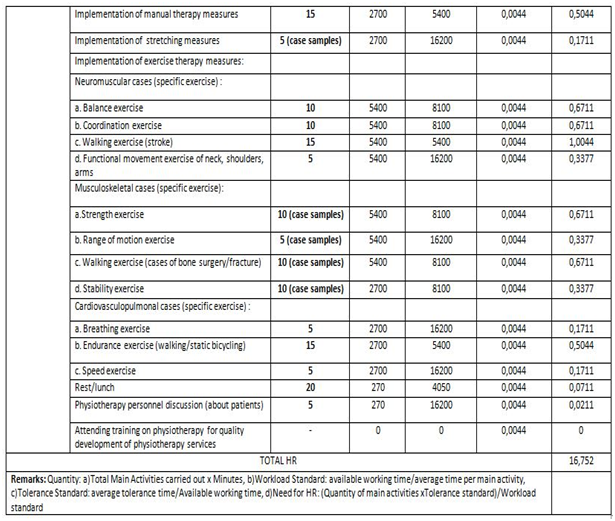
Table1. Indicators of physiotherapists’ workload assessment for new patientsTable2. Indicators of physiotherapists’ workload assessment for old patients Table 3. Calculation of total required physiotherapists (continued…) Table 3. Calculation of total required physiotherapists
Based
on the WISN method which divides the length of time to do activities by the
amount of time available for the physiotherapist and compared to the number of
patients and referring to the Minister of Health Regulation No. 65 of 2015
concerning physiotherapy service standards, and based on the analysis of
workload and/orservice ratio of patients/clients per working day (1
physiotherapist : 8-10 patients/clients per working day) with the assumption
that the available working time is 8 hours per dayand 1 hour of physiotherapy
processfor 1 patient 4,6,7. When seen from the data in the indicator
diagram based on the WISN method, then a calculation is made based on the
formula, by stating the total number of 40 patients per day in 1 year (average
visit), the result shows that the need for physiotherapists per day is16.75 or
rounded to be 17 in the medical rehabilitation unit of the Hospital (Table 3).
Based
on the results of review of the writing of the intervention time dose on the
patient card compared to the theory about the time of use of the physiotherapy
intervention device, there is a quite big differencein the implementation of
the intervention with the device, ranging from preparation, testing of
equipment, up to the intervention, as well as the provision of motion
exercises, and each experienced a reduction in time during the process by an
average of 15 to 20 minutes4,6,13. This happens to address all
patient needs in a relatively short period of time (5 working hours per day).
After
looking at the tables and risk interpretation diagrams interpretasiobtained
from interviews, questionnaires and review of patient medical records as well
as observation of intervention tools, figures are obtained indicating potential
risks in the physiotherapy processwith interpretation there is the influence of
the number of patients/workload on the physiotherapy process.
Likewise,
with the results shown in the conclusion table on the calculation of need for
HR, the result is obtained in the form of the amount of physiotherapists needed
in the medical rehabilitation unit of the Hospital X, with interpretation there
is a need for increased physiotherapists. Likewise, regarding the physiotherapy
device facilities specified in the Minister of Health Regulation number 65 of
2015 for Type B Hospitals and workload diagrams, there is a need for increased
physiotherapy intervention device facilities 6,8,13.
CONCLUSION
Based
on the measurement of risks in the stages of examination and measurement, there
is high risk of probabilities in the absence of examination and measurement as
well as in the mistake of report writing on the physiotherapy process; whereas
in the intervention stage,there is also high risk of probabilities in the
reduction of type and time of intervention with the impact of long or
unsuccessful healing process.
Based
on the workload calculation of the physiotherapy process with the Workload
Indicator Staffing Need, the mitigation policy taken is to add 13
physiotherapists so that the number of physiotherapists is 17 and supported by
arrangements for inspection days and the addition of intervention tools.
Recommendation: Hospitals are expected to analyze risks and work requirements using theWorkload Indicator Staffing Needboth in the physiotherapy unit and in other units. Analyzing this can reduce the risk of mistakes in patient documentation and adjust the workload of physiotherapists or other health professionals to work optimally.
Ethical
Clearance: Ethical aproaval letter
receivedfrom the Director of
General Hospital,Universitas
Kristen Indonesia to conduct this study with
reference number 295/DR/RSU UKI/05.2017 dated 19/05/2017.
Conflict of Interest: The Author has no conflict of
interest to declare.
Fund for the study: The study was fully funded by Universitas Kristen Indonesia.
Acknowledgement: The Author would like to thank the
General Hospital of Universitas Kristen Indonesia. Also, we would like to thank
the Universitas Kristen Indonesia which funded this study. Lastly, we extend
our gratitude to all physiotherapists who participated in this research.
REFERENCES
Andini, S, 2013, Analisa Kebutuhan Tenaga
Keperawatan di Instalasi Hemodialisa Rumah Sakit Umum Pusat Persahabatan
Berdasarkan Beban dan Kompetensi Kerja, Faculty of Public Health, Hospital
Administration Study Program, University of Indonesia, Depok.
Krisna, M 2012, Analisis Beban Kerja dan
Kebutuhan Tenaga di Instalasi Farmasi Rumah Sakit Jiwa Daerah Provinsi Lampung
Tahun 2012, Faculty of Public Health, Hospital Administration Study Program,
University of Indonesia, Depok.
Guspianto, 2012, Analisis Penyusunan Rencana
Kebutuhan Sumber Daya Manusia Kesehatan Puskesmas di Kabupaten Muaro Jambi,
Proceedings of National Seminar on Health, Department of Public Health, Faculty
of Medicine and Medical Science, Universitas Jenderal Soedirman, Purwokerto.
Ministry of Health. 2015. Minister of Health of
the Republic of Indonesia, Regulation No. 80 of 2013 concerningOperation of the
Work and Practice of Physiotherapists.
American Physical Therapy Association.
2013.Guide to Physical Therapist Practice, Second Edition, Virginia.
Ministry of Health. 2015. Minister of Health of
the Republic of Indonesia, Regulation No. 65 of 2015 concerning Physiotherapy
Service Standards.
World Health Organization 2016, Workload
indicators of staffing need (WISN): selected country implementation
experiences, (Human Resources for Health Observer, 15), World Health Organization,
20 Avenue Appia, 1211 Geneva 27, Switzerland.
Ministry of Health. 2004. Pedoman Penyusunan SDM
Kesehatan Di Tingkat Propinsi, Kab/Kota serta Rumah Sakit. Jakarta: Ministry of
Health of the Republic of Indonesia.
Winarti, W 2015, Hubungan Beban Kerja Perawat
Dengan Pelaksanaan Dan Pendokumentasian Asuhan Keperawatan Di ICURS PKU
Muhammadiyah Yogyakarta.
World Health Organization 2010, Software Manual
Workload Indicators of Staffing Need, Multilingual version, 2.2.169.1, World
Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland.
Ministry of Health of the Republic of Indonesia
and Deutsche Gesellschaft für Technische Zusammenarbeit 2009, Perlengkapan
Kerja WISN (Workload Indicators of Staffing Need).
Ministry of Health. 2004. Minister of Health of
the Republic of IndonesiaDecree Number: 81/MENKES/SK/2004 concerning Guidelines
for Formulation of Health HR Planning.
Behrens B, Michlovitz S, 2006, Physical Agents:
Theory and Practice, 2nd ed. Philadelphia, PA: FA Davis Company.
Citation: Novlinda Susy Anrianawati Manurung, et al (2020). Analysis of the need for physiotherapists in private hospitals in Indonesia using the workload indicator of staffing need referring to the implementation of the physiotherapy process as risk mitigation of services, International Journal of Medical and Exercise Science, 6 (1): 697-705.
S.Ramachandran1, C.J.Sivadharsini2, Jibi Paul3 Author: 1,3Pofessor, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India. Corresponding Author: 2B.P.T. Graduate, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India.Mail id: shivadharshini189@gmail.com
ABSTRACT
Background of the study: Obesity refers to a condition of excessive amount of body fat. The commonly known obesity are Central Obesity which occur due to the excess accumulation of fat in abdominal area. Various exercise have been designed for obesity but in particular exercise designed for abdomen are using mat, swiss ball and theraband exercise. Hence the study was to evaluate the effect by comparing mat, swiss ball and theraband exercise on abdominal obesity.
Methodology: It was an experimental study with comparative pre-post type. Study setting was conducted at Faculty of physiotherapy A.C.S Medical college and hospital, Chennai. 30 Subjects were randomly allocated equaly in to three groups. The sudy conducted for a duration of 12 weeks. Abdominal obesity female students ranges between the age of 18yrs-25yrs were selected for the study. Mat, Swiss ball, Theraband were used as materials for the study. Group A received mat exercise, Group B received swissball exercise and Group C received Theraband exercise. Body Mass Index (BMI), Waist circumferences were outcome measures for this study.
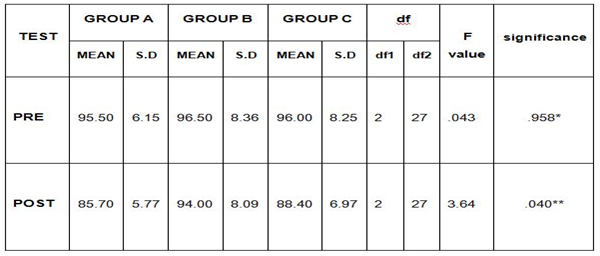
Result: On comparing Mean values of Group A, Group B & Group C; the Body Mass Index (BMI) shows significant decrease in the Post test Mean values. MAT Exercise with Group A shows mean value of 24.44 which is less effective than Theraband Exercise Group C value of 26.13 and Swiss Ball Exercise Group B with value of 40.09 shows significant difference between the group with P ≤ 0.001. On comparing Mean values of Group A, Group B & C on Waist Circumference shows significant decrease in the Post test Mean values; On MAT Exercise shows 95.50 which is lower mean value than Theraband Exercise Group C with 96.00 and Swiss Ball Exercise Group B with 96.50 shows significant difference between the group with P ≤ 0.001.
Conclusion: The study concluded that BMI and waist circumference of Group A shows better reduction when compared to Group B and C.
Keywords: Body Mass Index, Waist Circumference, Obesity, Exercise Mat, Swissball, Theraband
Received on 12 th February 2020, Revised on 19th February 2020, Accepted on 28th February 2020, DOI:10.36678/ijmaes.2020.v06i01.004
INTRODUCTION
The term
obesity is defined as cluster of non-communicable diseases called “New World
Syndrome” creating an enormous socio-economic and public health burden in
poorer countries. Abdominal obesity is also known as central obesity is where
excessive abdominal fat around the stomach and abdomen has built up to the
extent that it is likely to have negative impact on health 1.
Visceral
fat is composed of several adipose depots including mesentric epididymal white
adipose tissue (EWAT) and prenatal fat. An excess of visceral fat called
central obesity the “Pot Belly”or “Bear Belly” effects in which the abdomen
protrudes excessively. The body type is known as “apple shaped as Opposed to
pear shaped” in which the fat particularly develop in the hip region and
buttock region 2.
The obese
are at increased risk for cardio-vascular diseases and type 2 diabetics
however, somewho are affected with metabolic abnormalities. The regular
exercise would have a value rather than on scientific evidence and to reduce
the risk for metabolic disease through numerous mechanism 3.
The
regular exercise would have a value rather than on scientific evidence and to
reduce the risk for metabolic disease
through numerous mechanism. There are various exercise have been designed for
obesity such as aerobics exercise , yoga, palates etc 4.
Aim of study: The aim of the study
is to compare the effect of mat, Swiss ball and theraband exercise on reducing abdominal obesity among
college going female students.
Need of the study: The obesity refers
to the condition of having an excessive amount of body fat .The upper body fat is particular of carried with
in the abdomen various exercise have
been designed for obesity such as aerobics exercise, pilates ,yoga,and
others. Obesity also reduced by mat
exercises,swiss ball and theraband exercises.The study aim is to compare the
effect of mat ,swiss ball, theraband exercises on abdominal obesity patients.
METHODOLOGY
It was an experimental study with
comparative pre-post type. Study setting was conducted at Faculty of
physiotherapy A.C.S Medical college and hospital, Chennai. 30 Subjects were
randomly allocated equaly in to three groups. The sudy conducted for a duration
of 12 weeks. Abdominal obesity female students ranges between the age of 18yrs
-25yrs were selected for the study. Mat, Swiss ball, Theraband were used as
materials for the study. Group A received mat exercise, Group B received
swissball exercise and Group C received Theraband exercise. Body Mass Index
(BMI), Waist circumferences were outcome measures for this study.
Procedure : subject with 30
abdominal obesity female were selected and they were divided into two group and
each group contain 10 members.
GROUP A: MAT EXERCISES
1.Plank Exercise: Position: Quadriped position
initially or an exercise mat. Technique: From the starting position the patient
drops the buttock on the legs and extend the arms the a child position.Then
with palms and toes bearing the enhance weight, the head and trunk are from the
plank and this is repeated. Progression: 5-10 times per session and can be
progressed to 15-20 times as the patient
gains confidence.
2.Scissor Kicks : Position: Supine lying in an
exercises mat with legs fully extended and arms resting near the trunk . Technique:
Alternate legs are raised at a time in such a way that it resembles a
scissoring action the knees should not flex.
Progression:
20-25 times and then can be progressed 30-40 times per session .Thus exercise help to strengthen
the obliques.
3.Crunch Exercise: Crunches are performed to strengthening the core musculature. Position: Supine lying on a mat is the starting position. Technique: The knees are flexed in such a way that crook lying position attained. Hands are clapped around the chest or behind the neck.The patient tries to lift the shoulders from the floor and hold the position for a peak time. Progression: Initially performmed 8-10 times as the core gains strength the same can be repeated to 15-20 times.
4.Oblique Crunch Exercise : Position: Initially the position is side lying with one
leg on the other and the knees slightly bent.Technique: In this position , the patient tries to lift one
shoulder,trying to lateral rotate the trunk and the position is held for a peak
time. Progression:
Initially performed 8-10 times as the core gains strength , the same can be
repeated to 15-20 times.
GROUP B: SWISS BALL EXERCISES
1.Plank on Swiss Ball: Subjects lie in prone position with fore arm supported on swiss ball.
2.Back Extension on Swiss Ball: Subjects lie on prone lying swiss ball will be kept under abdomen. Arm should clasped behind head. Subjects
is instructed to trunk flexion and extension. This exercises is repeated for 5
times per day.
3.Swiss Ball Crunch: Subject will be allowed in supine
lying where swiss ball under lumbo sacral region with 90 degree of knee
flexion, Arms should kept along body
crossed on top of the chest.Lowering the torso into stretch position with
stationary neck will be starting position.Subjects will be instructed to flex
the hip by contracting abdomen and getting back into starting position.
4.Exercise Ball Abdominal Curl Up In Supine: Subjects will be allowed in supine lying where leg should placed on swiss ball.Hands are clasped in chest region .Subjects is allowed to lift the trunk upward until the shoulder region off, from the floor.
GROUP C: THERABAND EXERCISES
1.Theraband Abdominal Crunch In Supine: The subjects is asked to lie back and knees bent with the elbows straight
and lift the shoulder blades off the floor.The subjects is asked to hold 10
seconds and then relax practiced twice a
day for 10 days.
2.Therabandabdominal Oblique Crunch In Supine: After attaching the ends of the
band on the object .The subject is asked to extend one arm in front and grasp
the middle of loop,by keeping elbows straight .The subject is asked to hold 10
sec and then relax practised twice a day for 10 days .
3.Theraband Trunk Rotation In Sitting: The patient is askedto lifting the chair grasp the one end of the band and the other band at chest level. And asked to rotate the shoulders. The subjects is asked to hold for 10 sec and then relax practised twice a day for ten days.
4.Theraband Trunk
Extension inLong Sitting: The patient is asked
to sit in long sitting grasp the both end of bands with the hands at the chest
.The patient should keep the lumbar spine straight by extending the hips .The
subjects is asked to hold 10 seconds and then relax practised twice a days for
10days.
Fig. 5 Plank On Swiss Ball Fig. 6 Back Extension on Swiss Ball Fig. 7 Swiss Ball Crunch Fig .8 Exercise ball abdominal curl-up in supine
GROUP C: THERABAND EXERCISE
Fig.9 Theraband Abdominal Crunch in supine Fig.10 Theraband Abdominal Oblique Crunch in supine Fig.11 Theraband Trunck Rotation in sitting Fig.12 Theraband Trunk Extension in long sitting
Data Analysis : The collected data were tabulated and analyzed using both descriptive and inferential statistics. All the parameters were assessed using statistical package for social science (SPSS) Version 24. One way ANOVA includes of following test (Test Homogeneity of variance, ANOVA , post Hoc test Tukey HSD) (Multiple comparison) was adopted to find statistical difference between three groups .
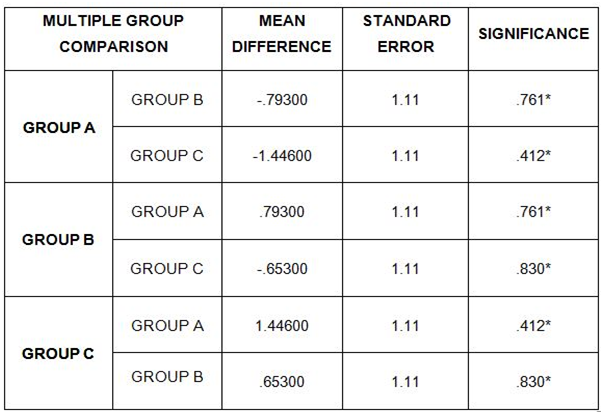
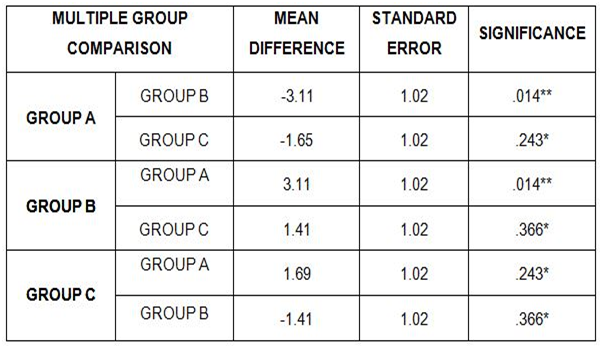
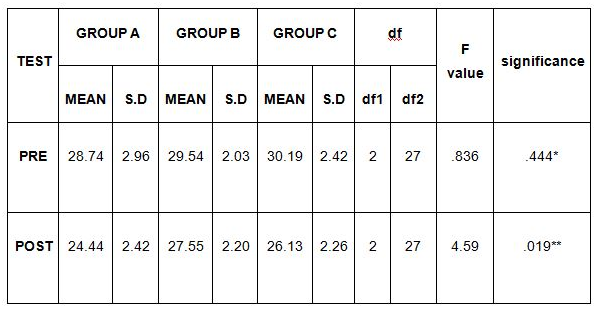
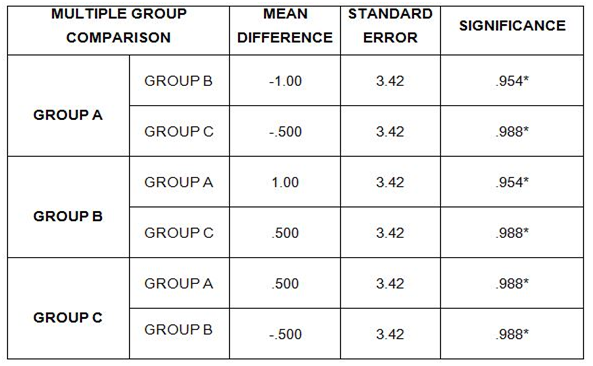
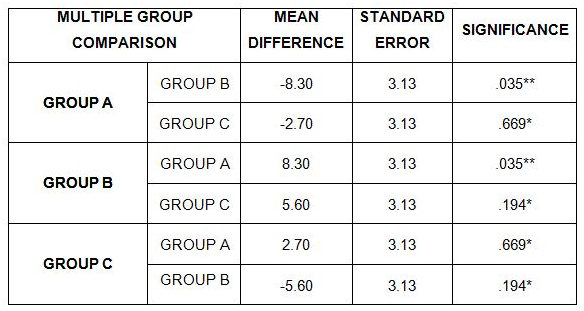
Table 1: comparison of pre test body mass index (bmi) using one anova multiplecomparison post hoc tukey hsd test between group a, group b and Group C Table2: Comparison of Post Test BMI score using One ANOVA multiple comparison Post Hoc Tukey HSD Test between Group A, Group B and Group C Table 3: Comparison of Pre & Post Body Mass Index (BMI) values using Test of Homogeneity of Variance & One way Anova Test between Group A , Group B and Group C Table 4: Comparison of Pre test Waist Circumference using One ANOVA multiple comparison Post Hoc Tukey HSD Test between Group A , Group B and Group C Table 5: Comparison of Post Test Waist Circumference Score using One ANOVA multiple comparison Post Hoc Tukey HSD Test between Group A , Group B and Group C Table 6: Comparison of Pre & Post Waist Circumference score using Test of Homogeneity of Variance & One Anova Test between Group A , Group B and Group C
RESULTS On comparing Mean values of
Group A, Group B & Group C on Body Mass Index (BMI) shows significant
decrease in the Post test Mean values,
but MAT Exercise in Group A shows mean value 24.44, which has the Lower Mean value is effective than Theraband Exercise
in Group C shows mean value 26.13
and followed by Swiss Ball Exercise in Group B shows mean value 40.09 at P
≤ 0.001.
On comparing Mean values of Group A, Group B
& Group C on Waist Circumference shows significant decrease in the Post test Mean values, but MAT Exercise in Group A shows mean value 95.50, which has the Lower Mean value
is effective than Theraband Exercise in Group C with mean value 96.00 and followed by Swiss Ball
Exercise in Group B with mean value 96.50
at P ≤ 0.001.
DISCUSSION
The present study was to compare the effects of twelve week
training program for reducing abdominal obesity between Group A with Mat with
Group B with Swiss ball and Group C with Theraband exercise.The purpose of this
study was take an indepth look at the use of weight control behaviours among
overweight and obese people Overweight adolescent were less likely to engage in
vigrous physical activity or to report healthy eating patterns behaviours that
create positive implication for weight management. In the present study age
group of 18-25 years which are divided into three group. And each group
assigned 10 members i.e Group A with Mat exercise contain 10 members, Group B
Swiss ball contain 10 members and Group C with Theraband exercise contain 10
members.
Metabolic
health risk was considered to include only categories of BMI, Hence keeping the
objective the present study into consideration waist circumference and BMI
measurement are considered as more valid and reliable outcome measures. The
most important findings of the study is to measure the abdominall obesity
demonstrated a strong response to effect of the mat, swiss ball and theraband
exercise by reducing abdominal fat5.
Mat
exercise which was performed to reduce abdominal obesity
and strengthens the abdominal muscles
and the subjects showed significant reduction in abdominal fat.
Swiss
ball exercise are performed on unstable surface the level of muscle activity
increases and in order to stabilize the spine muscle co-activation takes place.
The subjects shows better benefit in the study. Performing curl up and back
extension on swiss ball be a better method of strengthening core muscle and
resulting in increases the muscle activity6,7.
The
theraband exercise which is performed on reducing abdominal fat could be
because of the elastic resistance which does not rely on gravity and that it
provides continuous tension to the muscle being trained. Another unique benefit
could be the elastic resistance offers a linear variable resistance. Resistance
training requires more energy expenditure as a result it helps in reducing and
breaking of the abdominal fat. Maintanence of negative net energy balance
promotes weight loss. Hence theintensity
of exercise has to be increased progressively which was done in present study8,9.
In table 3 it reveals the Mean, Standard Deviation
(S.D), Homogeneity variance, ANOVA test, degree of freedom(df), F -value &
P value of the Pre & Post BMI score between Group A, Group B & Group C
in post test weeks. This table shows
that there is no significant difference in pre test values
of the BMI score between Group
A, Group B & Group C.
This table shows that there is in pre test weeks (P > 0.05) a significant difference in post test values
of the BMI score between
Group A,
Group B & Group C
in post
test weeks (P ≤ 0.05).
In table 6 reveals the Mean, Standard Deviation (S.D),
Homogeneity variance, ANOVA test, degree of freedom(df),F -value & P valve
of the Pre & Post waist circumference score between Group A, Group B & Group
C in post test weeks. This table shows that there is no significant difference in pre test values of the
waist circumference between Group A, Group B & Group C in pre test weeks P > 0.05.
This table shows that there is a significant difference in post test values of the
waist circumference between Group A ,Group B & Group C in post test weeks P
≤ 0.05.
The outcome measure of the study group namely mat,
swiss ball,and theraband exercise group
showed significant difference. When compared to pre and
post test. The stastics shows effectiveness of Group A with Mat exercise which
reduce the abdominal obesity. Thus present study was hypothesized that the mat
exercise showed more effective than the theraband and the Swiss ball.
Ethical
Clearance: Ethical
clearance has obtained from Faculty of Physiotherapy, DR. MGR Educational and
Reasearch Institute, Chennai to conduct this study with reference number: IV B/
PHSIO/ IRB/ 2017-2018dated 08/01/2018.
Conflict of interest: There was no conflict of interest
to conduct this study.
Fund for the study: It was aself financed study.
CONCLUSION
The result of the study concluded that 12 weeks
exercises program on mat, Swiss ball and theraband exercises are constitute to
reduce in abdominal obesity.
On comparing the post mean
value of BMI and waist circumference of Group A shows significant reduction
when compared to Group B and C. Hence this study suggest that mat exercises
more effective /beneficial to abdominal obesity patient.
REFERENCE
Kalra S Unnikrishnan A (2012). Obesity in india the weight of nation, Journel of medical nutritional and nutraceuticals, 1 (1): 37-41.
John M.Jakicic (2009). Department of health and physical activity and weight management research center, 17: 534.
Wilmore J. (1993). Physiology of sports and exercise, library of congress cataloging 3rd edition, 666-667.
Ludmila M. (2003). Effects of physio ball and conventional floor exercise on early phase adaptations in back and abdominal core stability and balance in women,Journal of strength and conditioning Reasearch, 17(4): 721-725.
Emil S. (2010). Swiss ball Abdominal Crunch with
added Elastic Resistance is an effective Alternative to Training Machine, International
Journal of sports Physical Therapy, 7: 372-376.
Escamilla (2010). Core Muscle Activation during
swiss ball and Traditional Abdominal Exercises Journal
ofOrthopaedics and sports
physio-therapy, 40: 265-276.
Vera – Gracia, F. J (2010). Abdominal muscles
response during curls ups on stable and labile surfaces journel of orthopaedics
and sports physiotherapy, 40:265-276.
Melissa J, (2001). Mayo Exercise- Induced Weight Loss Preferentially
Reduces Abdominal fat, Journal of physical Education and sports science., 9: 207-213.
Ross R, Pedwell H, Rissaneb J. (1995). Effects
of Energy Restriction and Exercise and exercise on skeletal muscle and adipose
tissue in women as measured by Magnetic Resonance Imaging American Journal of
clinical Nutrition, 61(11): 79-8.
Citation: S.Ramachandran, C. J. Sivadharsini, Jibi Paul (2020). Comparative study between Mat, Swiss Ball and Theraband exercises on reducing abdominal obesity among college going female students, International Journal of Medical and Exercise Science, 6 (1); 686-696.
Jibi Paul1, Louis Christy Maxwell2*, Ena Dulom2, B D Mark Raj2, Moorthy A3
Author: 1Pofessor, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India. 2B.P.T. Graduate, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India 3Asst.Professor, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India. Corresponding Author: 2*B.P.T. Graduate, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India.Mail id: louismaxo336@gmail.com
ABSTRACT
Background of the Study: Shoulder is a very complex joint crucial to many activities of daily living. Decrease shoulder mobility is a serious clinical finding in Frozen shoulder or Adhesive capsulitis, which affects 2-5% of the population and is most common in 40-60-year age group. The aim of the study is to compare the aquatic training exercise over free exercise on shoulder function among pa patients.
Methodology: This was an Experimental study with 30 male and female players. They were divided into two groups by simple sampling method, 15 players in each group. Age group of the subjects was 40 to 60 years. Group A players were trained with aquatic training. Group B players were trained with the free exercise. Both the group players are trained for 4 weeks and 3 sessions in a week. Aquatic trainingwas done in swimming pool at Rajiv Gandhi stadium, Chennai and free exercise therapy executed at Physiotherapy department ACS Medical College and Hospital, Chennai. Outcome Measures were, Range of Movement measured by Goniometer, Pain measured by Visual Analog Scale and Function was measured by (SPADI) Shoulder pain and disability index.
Result: On comparing Pre-test and Post-test within Group A & Group B on Visual Analog Scale, SPADI & Shoulder Range of Motion shows significant difference in Mean values at P ≤ 0.001.
Conclusion: Study concluded that the subjects treated with Aquatic training showed more improvement than Free Exercise in shoulder pain, range of movement and function.
Keywords: Frozen Shoulder, Aquatic Training, Range of Movement, Shoulder Pain And Disability Index
Received on 12 th February 2020, Revised on 19th February 2020, Accepted on 26th February 2020
DOI:10.36678/ijmaes.2020.v06i01.003
INTRODUCTION
The shoulder is a very complex
joint that is crucial to many activities of daily living. Decrease shoulder
mobility is a serious clinical finding. Frozen shoulder or Adhesive capsulitis
affects 2-5% of the population and is most common in 40-60-year age group 1,2.
Adhesive capsulitis is a condition characterized by progressive loss of both active and passive range of motion. The patients with adhesive capsulitis experience more pain compared to other shoulder conditions. The movements are usually restricted to a characteristic pattern with proportional greater passive loss of shoulder shoulder external rotation and abduction than any other movement 3,4.
The Frozen shoulder can be due to idiopathic or post traumatic causes, but the term adhesive capsulitis includes female gender, age older than40years, diabetes, thyroid disease, strokes, presence of autoimmune disorders5,6.
Three stages of adhesive
capsulitis are; 1) Freezing Stage: Mainly
characterized by severe pain in the shoulder even at rest. There is also decrease in shoulder external
rotation and abduction ROM. 2) Frozen Stage:
Pain is no longer present at rest but only with movement. Pain gradually
subsides but stiffness is marked lasting 4 to 12 months. 3) Thawing Stage: There is slow but progressive recovery of ROM.
The freezing stage in this stage pain becomes worse and range of motion becomes
more restricted. This phase lasts between 3 to 9 months and is characterized by
an acute synovitis of the glenohumeral joint7.
The second stage is called the
frozen or transitional stage in this there is a lack of synovial fluid, which
normally helps the shoulder joint, a ball and socket move by lubricating the
gap between the humerus and the socket in the shoulder blade. The shoulder
capsule thickens, swells, and tightens due to bands of scar tissue (adhesions)
that have formed inside the capsule. As a result, there is less movement in the
joint for the humerus, making movement of the shoulder stiff and painful. The
thawing stage is the final stage during which range of motion gradually
improves over several months to years8,9.
METHODOLOGY
This was an Experimental study with 30 male and female players. They were divided into two groups by simple sampling method, 15 players in each group. Age group of the subjects was 40 to 60 years. Group A players were trained with aquatic training exercise. Group B players were trained with free exercises.
Both the group players are trained for 4 weeks and 3 sessions in a week. Aquatic training was done in swimming pool at Rajiv Gandhi stadium, Chennai and free exercise therapy executed at Physiotherapy department ACS Medical College and Hospital, Chennai. Outcome Measures were, Range of Movement measured by Goniometer, Pain measured by Visual Analog Scale and Function was measured by (SPADY) Shoulder pain and disability index.
Intervention
Group B trained with Free Exercise For Periarthritis
1.ShoulderPendulum Stretch: Procedure: Relax your shoulder, Stand and lean over slightly, allowing the affected arm to hang down. Swing the arm in a circle about a foot in diameter. Prefer 10 revolution in each direction ,over a day.
2.Towel Stretch : Procedure:Hold one end of a three –foot long towel behind your back and grab the opposite end withyour other hand. Hold the towel in horizontal position.Use the good arm to pull the affected arm upward to stretch it.Do this 10 to 20 times a day.
3.Finger walk : Procedure: Face a wall three quarters of an arms length away. Reach out and touch the wall at waist level with the finger tips of the affected arm.
Figure 3. Patient performingFinger walk
4.Cross Body Reach : Procedure: Patient in sit or standing position. Use patients good arm to lift the affected arm at the elbow and bring it up and across your body,exerting gentle pressure to stretch the shoulder. Hold the stretch for 15 to 20 seconds .do this 10 to 20 times per day.
Figure 4. Patient performing Cross Body Reach
5.Armpit stretch: Procedure: Using your good arm to lift the affected arm out a shelf about breast high. Gently bend your knees ,opening up the armpit. Deepen your knees bend slightly ,gently stretching the armpit and then straighten
Figure 5. Patient performingArmpit stretch
6.Outward Rotation : Procedure: Hold a rubber exercise band between your hands with your elbow at a 90 degree angle close to your sides.Rotate the lower part of the affected arm outward two or three inches and hold for five seconds.repeat 10 to 15 times in a day.
Figure 6. Patient performingOutward Rotation
7.Inward Rotation: Procedure:-stand nexr ro a closed door and hook one end of a rubber exercise band across the locknob.hold the other end with the hand of the affected arm,holding your elbow at a 90 degree angle.pull the band towards your body two or three inches and hold for two seconds
Figure 7 . Patient performingInward Rotation
Group A trained with Aquatic Exercise
1.Aquatic exercise for Gleno-humeral joint restricted abduction: Position of the Patient was in Prone lying. Position of The Therapist was stand by side of the patient, places her hand over the top of the shoulder to palpate for the motion.
Procedure: Therapist makes the patient to move his/her shoulder passively to the restricted position. Therapist stabilized the shoulder joint, holds along the restricted position and contracts away from the Barrier. the therapist ask the the patient to move the affected limb in the restricited side.till the target is achieved.
2.Aquatic Exercise For Gleno Humeral Joint Restricted External Rotation: Position of The Patient was in Prone lying. Position of The Therapist was stand by side of the patient.
Procedure: Make the patient to move his/her shoulder passively to the restricted position. Therapist stabilized the shoulder, holds along the restricted position I.e. towards external rotation and contracts away from the barrier. Ask the patient to bring it for internal rotation with 1/3 of maximal effort. Hold for 6-7 secs and allow the patient to relax for 2 secs and then repeat the same after every 2 minutes for consecutive weeks.
Figure 8 Patient performingshoulder restricted restricted abduction and External Rotation Table 1. Comparison of Visual Analog Scale score on pre and post test wihin Group-A and Group-B
This table shows that there is significant difference in Pre-Test and Post-Test values between Group A and Group B (P > 0.05).
Table 2. Comparison of SPADI score on pre and post test within Group – A and Group – B
This table shows that there is significant difference in pre-test values between Group A & Group B (P>0.05).
Table 3. Comparison of ROM on Pre and Post test values within Group -A
There is a statistically significant difference between the pre-test and post-test values within Group A ( P ≤ 0.001).
Table 4 Comparison of ROM on Pre and Post test values within Group -B
There is a statistically significant on pre-test and post-test values within Group B( P ≤ 0.001).
Table 5. Comparison of Visual Analog Scale score on pre and post test between Group-A and Group-B
This table shows NO statistically significant difference in pre and post-test values between Group A & Group B (P ≤ 0.05). But higher mean difference in Group A (6.33, 2.26) Shows better effect than Shows better effect than mean difference Group B (6.26, 2.13).
Table 6. Comparison of SPADI score on pre and post test between Group A and Group B
This table shows statistically significant
difference in pre and post-test values between Group A & Group B (P ≤ 0.05). Group A with mean difference 33.630, shows better
effect than Group B mean difference
26.53.
Table 7. Comparison of ROM on Pre and Post test values between Group A and B
There is NO statistically significant difference between the pre-test and post-test values between Group A and B ( P ≤ 0.05). But Group A with mean difference 24.2, 15.47, shows better effect than Group B mean difference 22.8, 13.08. Respectively on abduction and external rotation.
RESULT
On comparing the Mean values of Group A & Group B on Visual Analog Scale, both the groups showed decrease in the pain intensity based on post-test Mean values in which (Group A ) shows 2.26 & (Group B) 2.13 Therefore no significant difference was found between post-test mean values at P> 0.05 (Table 1).
On comparing the Mean values of Group A & Group B on SPADI score, both the groups showed significant decrease in the post-test Mean values but (Group A ) shows 29.69 which has the Lower Mean value is effective than (Group B ) 37.34 at P ≤ 0.05 (Table 2).
On comparing the Mean values within the Group A & Group B on Shoulder Range of Motion (Abduction & External Rotation) both the group showed increase in the post-test Mean values in which Group A shows 107.26 & 42.33 degree (Group B) 106.53 & 40.26 degree respectively. Therefore no significant difference was found between post-test mean values at P> 0.05 (Table 3 and 4).
On comparing Pre-test and Post-test within
Group A & Group B on Visual Analog Scale, SPADI & Shoulder Range of
Motion shows significant difference in Mean values at P ≤ 0.001.
Table-5. Comparison of Visual Analog Scale score on pre and post test between Group-A
and Group-B. This table shows
NO statistically significant difference in pre and post-test values between
Group A & Group B (P ≤ 0.05). But higher
mean difference in Group A (6.33, 2.26) Shows better effect than Shows better effect than mean difference
Group B (6.26, 2.13).
Table
-6. Comparison of SPADI score on pre and post test between Group A and Group B. This table shows
statistically significant difference in pre and post-test values between Group
A & Group B (P ≤ 0.05). Group A with mean difference 33.630, shows better
effect than Group B mean difference
26.53.
Table-7. Comparison of ROM on Pre and Post test
values between Group A and B. There is NO statistically significant
difference between the pre-test and post-test values between Group A and B ( P ≤ 0.05).
But Group A with mean difference
24.2, 15.47, shows better effect than Group B
mean difference 22.8, 13.08. Respectively on abduction and external
rotation.
DISCSSION
This study is done to investigate, to find the effectiveness of aquatic training and free exercise on functional ability, pain and Range of motion of shoulder in patients with phase II Adhesive capsulitis.
In Adhesive capsulitis, there is loss of
range of motion in all planes and pain persists for months. In subacute stage
pain during movement of shoulder joint is more evident. In this study pain was
measured on VAS Scale, range of motion by Goniometer and functional impairment
was measured on Shoulder Pain and Disability Index.
The result of the study stated that there is statistically significant improvement in VAS, Range of motion and functional disability after 15 days training on aquatic training and free shoulder exercise. The study observed that on comparing both the Groups, there was statistically difference between Group A and Group B in Shoulder pain, ROM and functional disability index .
The age of participants was taken between
40-60 years both male and female in both the groups. The mean age in group A is
54.83 ±4.31 and in Group B it was 53.05± 5.02.
According to Robert Marske et al in the second or subacute stage of adhesive capsulitis shoulder pain does not necessarily worsen but there is pain at end of ROM, use of arm is limited causing muscular disuse. The primary role of mobilization is to restore joint play and facilitate joint movement by restoring arthrokinematics. The biomechanical effect manifests itself when forces are directed towards resistance but within limit of patient’s tolerance 10,11.
The Mechanical changes may include breaking
up adhesion in capsule, collagen realignment and improving interfibre glide
when specific movement stress the specific part of capsular tissue 12.
The aquatic exercise has an effect in reducing pain, increasing ROM and functional ability in patients with Adhesive capsulitis 13.
The aquatic exercise can stretches were effective in treating Range of motion especially external rotation and abduction in patients with periarthritis shoulder 14.
The study shows that aquatic exercise beneficial for decreasing pain, has vast effect on increasing Range of motion and functional ability in patients with periarthritis of shoulder 15.
Ethical
Clearance: Ethical
clearance has obtained from Faculty of Physiotherapy, DR. MGR Educational and
Reasearch Institute, Chennai to conduct this study with reference number: C-21/
PHSIO/ IRB/ 2018-2019dated 08/01/2019.
Conflict of interest: There was no conflict of
interest to conduct this study.
Fund for the study: It was aself financed study.
CONCLUSION
The Study concluded that the subjects treated with Aquatic Exercise And Free Exercise showed more effective in improvement of shoulder pain, function and range of movement. Free exercise also shows improvement in shoulder pain and Range of motion (ROM) and functional disability .
Limitation of the Study: The sample size of this study was small. The
study was for a Short duration and performed only for subjects with
Periarthritis shoulder.
Recommendation of the Study:
This study can conduct with different age groups. The sample size can be
increased in upcoming studies.
REFERENCES
Pink
MM, Tibone JE. (2000).The painful shoulder in the swimming athlete. Orthop Clin
North Am., 31:247–61.
Wolf
BR, Ebinger AE, Lawler MP, et al. (2009). Injury patterns in division I
collegiate swimming. Am J Sports Med., 37:2037-42.
Bak K. (2010).
The practical management of swimmer’s painful shoulder: etiology, diagnosis,
and treatment. Clin J Sport Med., 20: 386- 90.
Wanivenhaus
F, Fox AJ, Chaudhury S, et al. (2012).Epidemiology of injuries and prevention
strategies in competitive swimmers. Sports Health, 4: 246-51.
Tate A,
Turner GN, Knab SE, et al. (2012). Risk factors associated with shoulder pain
and disability across the lifespan of competitive swimmers. J Athl. Train., 47:
149–58.
McKenna
L, Straker L, Smith A. (2012). Can scapular and humeral head position predict
shoulder pain in adolescent swimmers and non-swimmers? J Sports Sci., 30: 1767-76.
Wymore
L, Fronek J. (2015). Shoulder functional performance status of national
collegiate athletic association swimmers: baseline Kerlan-Jobe orthopedic
clinic scores. Am J Sports Med;43:1513–7.
Beach
ML, Whitney SL, Dickoff-Hoffman S. (1992). Relationship of shoulder
flexibility, strength, and endurance to shoulder pain in competitive swimmers.
J Orthop Sports Phys Ther., 16: 262-8.
Heinlein
S A, Cosgarea A J. (2010). Biomechanical
considerations in the competitive swimmer’s shoulder. Sports Health, 2: 519-25.
Hill L, Collins M, (2015). Posthumus M. Risk
factors for shoulder pain and injury in swimmers: a critical systematic review.
Phys Sports Med., 43:412–20.
Hibberd EE, Laudner K, Berkoff DJ, et al. (2016).Comparison
of upper extremity physical characteristics between adolescent competitive
swimmers and nonoverhead athletes. J Athl Train., 51: 65-9.
Bak K, Magnusson SP. (1997). Shoulder
strength and range of motion in symptomatic and pain-free elite swimmers. Am J
Sports Med., 25:454-9.
Harrington S, Meisel C, Tate A. (2014). A
cross-sectional study examining shoulder pain and disability in division I
female swimmers. J Sport Rehabil, 23: 65-75.
McMaster WC, Roberts A, Stoddard T. A (1998)
Correlation between shoulder laxity and interfering pain in competitive
swimmers. Am J Sports Med.,26: 83-6.
Zemek M
J, Magee D J. (1996). Comparison of glenohumeral joint laxity in elite and
recreational swimmers. Clin J Sport Med., 6: 40-7.
Citation: Jibi Paul, Louis Christy Maxwell, et al (2020). A comparative study of aquatic training exercises over free exercise technique on shoulder function among periarthritis shoulder patients, International Journal of Medical and Exercise Science; 6(1); 677-685.
Authors: 2Pofessor, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India. 3Asst. Professor, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India. Corresponding Author: 1B.P.T. Graduate, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India. Mail id: reenamol193@gmail.com
ABSTRACT
Background of The Study: Hamstring is one of the commonest muscles often get tight as the biomechanics of hamstrings are complex because they pull over hip and knee joints. Stretching methods often define the development and improves body’s range of motion. Goal of all stretching relaxation is to provide joint mobility while maintaining joint stability. Hold relax is a technique of facilitating normal muscle sensation and muscle awareness. It is a relaxation technique to obtain lengthening reaction of muscle whose action is antagonist to movement limited in range. It is effective, simple and pain-free. PNF is used to supplement daily stretching and employed to quick gain in ROM, decreases in fatigue, prevent overuse injuries. The main objective of this study is to compare the effectiveness of passive stretching over PNF hold relax technique on hamstring tightness in young individuals. Materials And Methods: 100 normal male and female subjects were recruited for the study with age group of 18-25 yrs and divided into two groups. Group A (n=50) treated with passive stretching Group B (n=50) treated with hold relax PNF technique. Outcome measures of the study were Finger Tip to Floor test, Back Saver Sit and Reach test. Result: The study shows there is statistical significant difference with P≤0.001 between Group A and B. When compare the two groups, Group B with PNF Hold relax gives more effective than the Group A with Passive stretching with Back Saver Sit and Reach test. Conclusion: The study concluded that PNF Hold Relax technique showed greater improvement than Passive Stretching on hamstring flexibility .
Key words: Hamstring flexibility, Passive stretching, PNF hold relax, Finger Tip to Floor test, Back Saver Sit and Reach test.
Received on 10 th February 2020, Revised on 19th February 2020, Accepted on 25th February 2020 DOI:10.36678/ijmaes.2020.v06i01.002
INTRODUCTION
Hamstring tightness is common in normal individual because of immobilization in a shortened position results in adaptive shortening. Tightness could make the musculo-tendinosus unit more susceptible to injury, increases resistance to anatomical structures, which may leads to overuse syndrome. Muscle tightness affects the normal length tension relationship. Muscle tightness also cause reciprocal inhibition 1.
The hamstring flexibility is defined as the ability to move a joint or series of joints through full, unrestricted, pain-free range of motion. Flexibility is a key component for Prevention of injury and rehabilitation, stretching decreases injury and improves performance in sports for overall fitness. Increased flexibility: While stretching your hamstring can increase flexibility and improve your range of motion in your joints. Improved hamstring flexibility which will be able to perform everyday activity like climbing stairs, lifting or bending over with greater ease. Reduced hamstring muscle flexibility has been implicated in lumbar spine dysfunction, with number of studies showing positive correlation between decreased hamstrings, flexibility and low back pain 2, 3.
The hamstring muscle refers to those muscles that lie on the back of upper leg and thighs. They are strong muscles that can stretch up to 1.5 times their size, with regular stretching exercises.These muscles are used in almost all physical activity and keeping them stretched and goes a long way in improving overall flexibility and strength.Hamstring stretch are popular stretch used by gymnast, runners and sprinter to improve the flexibility of their muscles and to get ready with a warm up stretches with just the wall or a study chair for support loosen up tight muscles and improves blood flow to the lower limbs. Hamstring muscles make more flexible, preventing injury and tearing of the muscles 4.
Passive stretching: Passive stretching is also referred to as relaxed stretching. A passive stretch is a stretch where an individual will assume a position and hold it with the help of therapist/partner. The specificity of movement that a person performs in regular physical activity and stretching method often define the development and improve body’s range of motion. Goal of passive stretching programme is to provide joint mobility while maintaining joint stability.
PNF Technique: PNF is defined as exercises that enhance a neuro muscular response through the proprioceptors. Proprioceptive neuro- muscular facilitation is used as inhibition technique to assist with muscle elongation. PNF is used to supplement daily stretching when employed to quick gain in range of motion; it decreases fatigue and prevents overuse injuries. Hold relaxtechnique involves lengthening a tightened muscle and asks the patient to isometrically contract the muscle for several seconds. As the patient relaxes, after the contraction, the therapist lengthen the involved muscle further and holds the stretch at the end range of motion. Hold relax is a technique of facilitating normal muscle sensation and muscle awareness, used in treating hyper tonicity or motor dysfunction. It is often applied when there is muscle tightness in one side of joint and when immobility is the result of pain. PNF stretching was found to decrease muscle force in the hamstring muscles in response to the application of sudden stretch as might occur during functional activity.
Need of the study: Hamstring is one of the commonest muscles often get tight. The biomechanics of hamstrings is complex because they are two joints (hip & knee). Goal of passive stretching relaxation should be provided for joint mobility and maintaining joint stability.PNF Hold relax is a technique for facilitating normal muscle sensation, muscle awareness and decreases fatigue to prevent overuse injuries. The main aim of this study is to compare the effectiveness of passive stretching and PNF hold relax technique on hamstring tightness in young individuals.
METHODOLOGY
This is an experimental study with Pre and Post Comparative test. The study was conducted at Physiotherapy department, ACS Medical college and Hospital campus, Chennai. 100 normal subjects with age group of 18-25 yrs were recruited for the study and divided into two groups. Random sampling method used to allocate the samples in each group. Group A (n=50) treated with passive stretching Group B (n=50) treated with hold relax PNF technique. The study conducted for a duration of 2 months. Subjects with Recent fractures, Spinal deformity, TB spine, Psychological disorders were excluded from this study. Outcome measures of the study were Finger tip to floor test, Back saver sit and reach test. Materials used for this study were informed concent, Inch tape, Scale, Couch Mark sheet.
Intervention
Finger -Tip- To Floor Test: The patient stands comfortably with the feet facing forward and is asked to bend forward. The instruction is to bend forward without bending their knees, attempt to touch the floor with your fingertips, go only as far as you can”.
Distance between the patient long finger and the floor is measured in inches. The process is performed once, the best effort is measured.
Back saver sit and reach test: The variations of the traditional sit and reach test is to measure the flexibility of the left and right legs separately. This is the procedure used for the Fitness Gram Program. This test measures the flexibility of the lower limb and hamstring muscles. Back Saver Sit And Reach Test is extremely high 5,6.
Fig. 1 Finger tip to floor test
Group A: passive stretching.
Procedure: The patient in supine position. The therapist should kneel down on the mat and place the patients heel against own shoulder and placed both hands along the anterior aspect of distant thigh to keep knee extended, opposite extremity is stabilized in extension position and therapist knee place by with in 0 degree extension, hip in neutral position and then investigator flexes the hip as far as possible. The stretching duration for 30 seconds.
Group B: PNF hold relax technique.
Procedure: The patient in supine lying position. For each stretching, therapist give passive stretching until the patient reports mild stretching sensation and hold that position for 30 seconds by asking his / her leg to push back towards against resistance of therapist shoulder, after contraction and relaxation for 30 seconds, measurement should be taken.
Fig .2 Passive StretchingFig.3 PNF Hold Relax technique
RESULT
In Table 1 with group a, ftf and bssr have significant difference between the pre test & post test (p≤ 0.001).
Table 1 Comparison of FTF and BSSR in group a between pre and post testGraph 1. Comparison of FTF and BSSR in Group A between Pre and Post test.Table 2 Comparison of FTF and BSSR in Group B between Pre And Post Test
In table 2 with Group B, FTF and BSSR have significant difference between the pre & post test value (P≤0.001).
Graph 2. Comparison of FTF and BSSR in Group B between Pre and Post testTable 3. Comparison of FTF between Group A And B in Pre And Post Test
This table shows that there is no significant difference in the pre test value between Group A and Group B (P≥0.05). This table shows that there is no significant difference in the post test value between Group A and Group B (P≥0.05).
Graph 3. Comparison of FTF between Group A and B In Pre and Post test.Table 4 Comparison of bssr between group a and b in pre and post test
This table shows that there is no significant difference in the pre test values in the score between Group A and B. This table shows statistically significant difference in post test values in BSSR score between Group A & Group B (p≤0.001).
Graph 4. Comparison of bssr between group a and b in pre and post test.
DISCUSSION
The present study compared the effectiveness of passive stretching and PNF Hold Relax technique on hamstring tightness in young individuals. In this study suggested that Group B [PNF Hold Relax technique] showed greater improvement than Group A .
There is another study which shows there is no significant difference in ROM in standing & supine hamstring stretching as they are equally effective conducted by “Decoster LC (2004) 7,8.
In Table 1,it shows significant increase in post test mean value of Group A [passive stretching] which has more effective mean value than pre test. In table-1 shows statistically highly significant difference in BSSR & FTF between pre test and post test (p ≤ 0.001).
In Table 2 shows significant increase in post test value of BSSR compare to FTF in Group B [PNF Hold Relax technique]. The pre test reduces compared to post test in BSSR of Group B shows significant between pre and post test (p ≤ 0.001).
In Table 3 shows effective increases in Group B compared to Group A, but it shows a negative pattern between pre and post test. Sharman Malanie who found that propioceptive neuromuscular facilitation produces superior ROM 9,10,11.
In Table 4 shows significant increases in Group B compared to Group A (P≤0.005). Therefore the use of PNF hold relax technique in Group B (p≤0.001) shows greater effective than Group A which will reduces the hamstring tightness.
A number of studies have demonstrated that stretching muscle tissue can increase joint range of motion 12,13,14.
Ethical Clearance: Ethical clearance has obtained from Faculty of Physiotherapy, DR.MGR Educational and Reasearch Institute, Chennai to conduct this study with reference number: 025/ PHSIO/ IRB/2016dated 06/02/2016.
Conflict of interest: There was no conflict of interest to conduct this study.
Fund for the study: It was aself financed study.
CONCLUSION
The result suggested that PNF Hold Relax technique showed greater improvement than Passive Stretching. This study reveals that there is a significant difference between passive stretching and PNF Hold Relax technique. In the end of this study, PNF Hold Relax Technique is found to be more effective and reduces the tightness of hamstring muscles compared to passive stretching groups.
Limitation of the Study: The sample size of this study was small.
Recommendation of the Study: This study can conduct with different age groups. The sample size can be increased in upcoming studies. Different outcome measures recommended.
REFERENCES
Carter, AM :Kinzey, ss, chitwood, LF, et al : (2009). PNF decreases muscle activity during the stretch reflex in selected posterior thigh muscles. Jo sports Rehabilitation :9 (4) 249-278.
Spernoga SG, Uhl TL. (2001). Duration maintained hamstrings flexibility after one time, modified hold relax stretching protocol. Journal of Athletic Training, 6:44-48.
Yogeeta SK. (2010). Effectiveness of passive stretching vs hold relax technique in flexibility of hamstring muscle. J. Health Allied Science, 9 (3); 13.
Corbin C B Noble, (1980). Flexibility-A major component of physical fitness, Journal of Physical Education, 51-57.
Hui S.S., Yuen P.Y. (2000) Validity of the modified back-saver sit-and-reach test: a comparison with other protocols. Medicine and Science in Sports and Exercise 32, 1655-1659.
Hui S.C., Yuen P.Y., Morrow J.R. Jr, Jackson A.W. (1999) Comparison of the criterion-related validity of sit-and-reach tests with and without limb length adjustment in Asian adults. Research Quarterly for Exercise and Sport 70, 401-406
Decoster L C. (2004). Standing & supine hamstring stretching are equally effective. Journal of Athletic training 39(4); 330-334.
Len Karvitz, P.H.D., (2000). Vivian H Heyward, Flexibility Training Journal of Fitness Training, 7:18-20.
Worrell, T., T. Smith, and J. Winegardner. (1994). Effects of hamstring stretching on hamstring muscle performance. JOSPT 20: 154-159.
Ross, M. (1999). Effects of lower extremity position & stretching on hamstring muscle flexibility. J. strength cond., Res. 13: 124-129.
Tanigawa MC. (1972). Comparison of the hold-relax procedure and passive mobilization on increasing muscle length phys. Ther., 7; 725-35.
Malanie S. (2006). PNF stretching mechanism & clinical implication. Journal of sports medicine 36(11) : 929-939.
Malanie S. (2006). Proprioceptive neuro-muscular facilitation stretching Mechanism and clinical implication. Journal of Sports Medicine, 36(11): 929-939.
Worrell TW, Smith TL et al. (1994). Effect of hamstring stretching on hamstring muscle performance. Journal of Orthopaedic Sports, 20(3):154-159.
Citation:
Reena R, Jibi Paul, Praveen Kumar (2020). To compare the effectiveness of passive stretching versus pnf hold relax technique on hamstring tightness in young individuals , International Journal of Medical and Exercise Science; 6 (1); 669-675.
Lucky Anggiat1, Wan Hazmy Che Hon2, Siti Nur Baait binti Mohd Sokran3, Nurul Mawaddah Binti Mohammad3
Author: 1Faculty of Vocational Studies, Physiotherapy Program, Universitas Kristen Indonesia, Jakarta, Indonesia 3School of Health Sciences, KPJ Healthcare University College, Nilai, Malaysia Corresponding Author: 2Consultant Orthopaedic Surgeon, KPJ Seremban Specialist Hospital and KPJ Healthcare University College, Jalan Toman 1, Kemayan Square, 70200 Seremban. Email address: whazmy@hotmail.com
ABSTRACT
Background of study: Non-specific low back pain (LBP) becomes the most common cases in University population. Prolonged sitting has been identified as one of the factors leading to non-specific LBP among University population. The purpose of the study is to identify the change of functional disability in non-specific LBP among university population after PNF and McKenzie method.
Methods: A quasi-experimental study involving 36 subjects (students and office workers) from the university population. The study population were selected from students and office worker of KPJ Healthcare University College (KPJUC) who met the inclusion criteria. The subjects were divided into three treatment groups: PNF group, McKenzie group and control group (hot pack and educational home exercise sheet) which underwent 12 treatment sessions distributed over three times in a week for four weeks duration. Subjects were measured on functional disability by Oswestry Disability Index (ODI). Measurement was performed at pre-test, mid-test and post-test. Repeated measures ANOVA was used to analyse the effectiveness of PNF and McKenzie treatments based on the measurement time.
Result: This study showed that the PNF and McKenzie gave effect in improving ODI score in within group analysis. However, the results of PNF showed that it has more effect than McKenzie method on functional disability score (p <0.05) after 4 weeks.
Conclusion: There was a change in functional disability on non-specific LBP after PNF and McKenzie method. Furthermore, the study findings showed that the PNF exercise has more effect in improving functional disability compared to McKenzie method on non-specific LBP among university population.
Received on 10th February 2020, Revised on 19th February 2020, Accepted on 24th February 2020
DOI:10.36678/ijmaes.2020.v06i01.001
INTRODUCTION
Low back pain (LBP) consists of two
types, which is specific and non-specific LBP. Specific back pain can further
be divided into LBP which that is related with vertebrae and
non-vertebrae. The non-specific LBP is developed from
the soft tissue, which is poorly localised 1. In addition,
non-specific LBP is further classified into LBP, which is not related to the
neurological problem and degenerative syndrome. Prolonged sitting led to
increased body discomfortness in the neck, shoulder, upper back,
low back, and buttock while prolonged slumped sitting may be related to
Internal Oblique or Transverse Abdominis muscle fatigues—compromising the stability of the spine, making it
vulnerable to injury 2.
University population mainly consists of students, office workers and academicians, which have similar habit to experience prolonged sitting. Students usually attend the classroom session for learning theories and at the same time working in front of computer to browse some resources. They experience prolonged
sitting in most of their daily activities. A previous study conducted by Nordin, Devinder, and Kanglun reported
31% of students usually sat in the classroom or worked daily in front of the computers everyday for 6 to 8 hours 3.
Similarly, majority of the office
workers working in the university, sit more than 4 hours daily with 90.8%
prevalence while other office workers who sit in the same working position
usually leave their office chair only for 10 minutes or less each day have
scored about 65.8% prevalence. Prolonged sitting is one of the factors causing
musculoskeletal pain among university population, which are student and office
worker, who experienced from having LBP (LBP), which commonly reported 4.
A study conducted by University in
Columbia found that 45% of the university population were having severe chronic
pain specifically in the lower back region. A study by Nordin, Devinder, and
Kanglun; also revealed similar results which stated that 64.6% of students had LBP and it was found that the students also sat in the classroom or worked in front of the computers everyday between 6 to
8 hours 5,6.
Some anatomical condition related
to those factors can be contributed to the
incidence of LBP. Low back pain may developed by some factors which increase lumbar lordosis, reduce abdominal muscle
length and strength, and decrease back extensor muscle endurance, back extensor muscle flexibility, length
of iliopsoas, hamstring muscle flexibility, body composition and others 7,8.
A study by Casas et al. found that
the prevalence of limitation for academic activities was almost 30% and it affected to both office
workers and students on their daily life activities. It caused potential effects to the life quality
of both the office workers and the students. The limitation in academic activities due to pain was 29.8%. The researchers concluded that there was moderate
disability due to LBP among physiotherapy students in Mumbai 9.
The similar potential risk happened
to office workers who were suffering from LBP. An employee with
LBP usually took a day off from his work for medical check-up would decrease the company’s productivity if it had a significant number of employees who were absent from work due to having LBP. The impact
of LBP on physical activities does not only
depend on the pain but also on some functional disability, which is
inter-related one to another 10,11.
There are several options and
suggestions on the treatment to reduce LBP in the population . Exercise is also
one of the physiotherapy treatments that can
strengthen the muscle that supports the spine 12,13.
Theraphy exercise was found to be the best choice to reduce LBP
and to increase body functions in adult
people who experienced LBP. The therapeutic exercise for LBP uncommonly
performed by physiotherapist called Proprioceptive
Neuromuscular Facilitation (PNF), however; this treatment is commonly used for
neurological conditions 16,17.
PNF has been recommended for
sensory-motor control training, as well as for stimulating lumbar muscle
proprioception. Kofotolis and Kellis stated in their
study that PNF significantly improve the muscle endurances. They defined that the Rhytmical Stabilization (RS) exercise provided the trunk static endurance and
Combination of Isotonic (COI) provided dynamic muscle
endurance 18,19.
In other studies, in comparing modalities of
therapy exercises, PNF was shown to have better result than manual therapy,
core stability exercise and ball exercise for LBP which was commonly used for the trunk muscle, pelvic
stability, and core muscle 20, 21.
A common therapy exercise used for LBP was developed by Brian McKenzie, which was
recognised as McKenzie method. A systematic review study has shown that
McKenzie therapy is more effective than the comparred treatment at short-term follow up for spinal
pain. The comparative treatments in these trials include Non-Steroid Anti
Inflammation Drugs (NSAIDs), educational booklet, back massage with back care
advice, strength training and spinal mobilization and general mobility
exercises. McKenzie method can be a familiar treatment and it is one of the common choices used by most
physiotherapists for treating LBP 22,23.
There were several studies that
performed the specific exercises to treat LBP, such as McKenzie method, PNF,
ball exercise, yoga, spinal stabilization exercise, Mat based Pilates and
ordinary exercise that is aerobic exercise which is effective and it has a good result for LBP. However, these previous
studies did not conduct any comparison between PNF exercise
and McKenzie method to verify the effect of each treatment. Therefore, this
study carried out the changes of functional disability among university
population after the PNF exercise and McKenzie method and specifically
comparing the effects of those treatments 24,25.
METHODOLOGY
This was an experimental study using
quasi-experimental study. Quasi-experimental study is defined as study
comparing the effect and value of intervention in between three groups at their
pre-test, mid-test and post-test design in which subjects are equally differentiated
on the treatment given and on
the control group. All
subjects that included in this study were assigned to three groups. Upon
selection, subjects were given written and verbal study information and
informed consent, which states that they are willing to be the subject of this
research. Informed concent received from all subjects then physiotherapist
assessed the subject based on the measurements called disability score using Oswestry Disability Index (ODI). In addition, the information about age, gender, occupation and years of
working or studying were collected and presented as socio-demographic data of
the subjects.
The three groups of subjects, who had been managed with PNF exercise,
McKenzie method and control group respectively, were compared. The assessment point was performed at three points;
pre-test as the baseline measurement, mid-test was given two weeks after treatment and post-test as the
last measurement after four weeks treatment. The subjects had to undergo 12
sessions of treatment, 3 sessions in each week of four-week-treatment. This
study was conducted in a private academic institute and the ethical approval
has be obtained from School of Health Sciences, Research Management Centre, KPJ
Healthcare University College (KPJUC), in Nilai, Negeri Sembilan, Malaysia
before starting the study.
The inclusion criteria were the subjectssuffering from chronic
non-specific LBP. Chronic non-specific low back pain was determined based on the subjects’ report. The
physiotherapist conducted the assessment to make sure the low back pain was
non-specific in nature 3, 4. All subjects were also asked about their
duration of sitting in a typical working day because prolonged sitting is one
of the contributing factors for non-specific low back pain with age ≥ 18 to 45 years old 26, 27.
Participants were excluded in this study
according to the exclusion criteria, which are subjects with any history of
pathological conditions or diagnosed with disk herniation, spinal stenosis,
spondylolisthesis, spondylitis, radiculopathy, vertebral fracture, surgery to
lumbar spine, reported with pregnancy and reported with other medical illnesses such
as tumour, kidney disease, and visceral disease 28.
The subjects were 36 subjects and the office workers
of KPJUC who met the selection criteria prior to sample screening. The determination of the sample size was done using G*power 3. The three groups used F test, the effect size f was 0.25 and power was 0.8. Based on the data, the calculated total sample size is thirty and as additional subject is 20% from total sample size, which is six and therefore, the total sample size were thirty-six with twelve subjects for each group. The sample size was determined based on a previous study.The timing for the implement-tation of data collection and testing of the research subjects was from August 2017, December 2017.
Three of the physiotherapists
participating in this study were trained by the principal physiotherapist to
perform the specific PNF exercise and McKenzie method used as experimental treatment in this study. The training includedwith visual demonstrations, hands-on experience and technique evaluation. The training was continued until
all physiotherapists had successfully mastered each technique. Physiotherapists
performing the PNF exercise and McKenzie method reached the training criteria
within two-week period. In addition, these three
physiotherapists were closely supervised by the principal physiotherapist in
charge in KPJUC Rehab Centre to assure proper performance of PNF exercise and
McKenzie method for the techniques and the assessment of the subjects.
Measuring Tools: The Oswestry Disability Index (ODI)
was used to assess the subject’s disability that caused by the non-specific LBP. The questionnaire contains 10 sections, with six
statements for each section. The questionnaire can be self-administered
by the patient or assessed by the physiotherapist; it is usually completed in
less than five minutes and scored in less than one minute 29.
Each subject was asked to select one
statement in each section of the questionnaire which best represents his or her
perceived ability to perform a function and a quantity of pain experienced on the assessment day. Each statement is scored on a 6-point scale (0-5), where a score of
“0” is awarded if the client selects the first statement of the section and a
score of “5” is awarded if the client selects the last statement. The section
scores are tallied to produce a total raw score. Total raw scores can vary from
0 to 50 and the percentage ranges from 0-100 30.
Intervention Procedures: Subjects in the group I received the
PNF exercise intervention. The PNF technique was performed on the trunk movement. The patient was in a sitting position. First, the
physiotherapist conducted the Rhythmic Stabilisation (RS). The RS exercise
consisted of alternating (trunk flexion-extension) isometric contractions
against resistance for 10 seconds, with no motion intended. The subjects
performed three sets of 10 repetitions at maximal resistance provided by the
same physiotherapist. The resting intervals of 30 seconds and 60 seconds were provided after the completion of 10 repetitions
for each pattern and between sets, respectively. Secondly, the physiotherapist
conducted combination of isotonic technique with flexion or extension for
lumbar, depending on the patient condition. The combination of isotonic technique consists of alternating
concentric and eccentric contractions of agonists without relaxation. The
resisted active concentric contraction for 5 seconds, resisted eccentric contraction
for 5 seconds, and resisted maintained during contraction for 5 seconds (trunk
flexion-extension). The combination of isotonic performed three set of 10
repetitions with resting intervals of 30 second and 60 second were provided
after completion of 10 repetitions for each pattern and between sets,
respectively. Then, all PNF exercises will be held for
30-45 minutes 31.
The subjects in the group II
received the McKenzie method treatment. The physiotherapist guided the subject
to conduct four extension exercises and three flexion exercises. The extension
exercise started with these
following stages. Firstly,
the subjects laid their face down for one until two minutes.
Secondly, they laid their faces down with
extension. The subject were asked to start laying their faces into down position followed by the extension of the trunk on the elbow and held on for five seconds and went back to the first position as a relaxation. Thirdly, extension on lying, the subjects were instructed to
start lying their faces into down position, followed by the extension of the trunk with elbow extension
(push-up position) for ten seconds, then the subject were asked to relax by going back to the first position.
Forthly, extension on standing, the subjects were instructed to
get standing position and then they were asked to do the extension of the trunk and to hold for five seconds with hands of the back
and the fingers pointing backwards, followed by a relaxation by going back to the standing position. All extension exercise were repeated for ten repetitions in two sets.
The flexion exercise was started by these following steps. Firstly, flexion on lying, the
subjects wereasked to get a lying position and asked to flex the
trunk with both knees to the chest and to hold with both
hands. Subjects were instructed to hold that position for
five seconds and get a relaxation by going back to the first lying position. Secondly, flexion on sitting, the subject were asked to sit on the edge of a chair and instructed to bend the trunk forward and to grasp the ankle or to touch the floor with both hands. This position was maintained for five seconds and it was followed by a relaxation to the first position. Thirdly, flexion on standing, the subjects wereasked to get a standing position, then instructed to bend
forward or to flex the trunk with fingers down to the legs as far as the subjects comfortably reach them. The subjects wereasked to hold on the last position for five seconds and asked to go back to a standing position
as a relaxation. Then, all flexion exercise was also repeated for ten repetitions in two sets. There were three minutes for resting intervals in every
set. The McKenzie treatment lasted for 20-40 minutes 30.
The subjects in the group III were treated using hot pack for 15 minutes as a basic
treatment for non-specific LBP. The physiotherapist
gave them some home exercises guided by educational exercise sheet and teach the subjects how to use
it. A narrative review,
written by Bardin, King and Maher , revealed
that a hot pack considered as the first line of care for non-specific LBP
along with self-management with home exercise. The exercise based on the
educational exercise sheet lasted for 7-10 minutes that can be done at home or
the office. All of the subject in each group underwent 12 sessions of treatment, 3
sessions in each week of a four-week-treatment.
Data analysis: All data analysed were
performed by
using IBM SPSS Statistics for Windows,
Version 22.0. Repeated measures ANOVA analysis were used to
determine the result of differences before and after treatment given in every group. Repeated measure ANOVA
within-between groups analysis were applied to
determine the effect between three treatment groups based on time measurement.
Bonferroni adjustment were applied for multiple comparison.
RESULT
The total number of subjects of 36 was divided into 3 treatment groups, and each group consisted of 12 subjects. Most of the participants were 18-25 year-old subjects (75%), female (63.9%), and students (61.1%) who had been studying or working for 1-3 years (75%). The socio-demographic details such as age, gender and occupation are tabulated in Table 1.
Table 1. Socio-demographic distribution of the subjects (n=36)
Table 2 described the within group result of PNF exercise, McKenzie and Control group using Oswestry Disability Index (ODI) in terms of Mean Difference (MD) and Confidence Interval (CI). There was a significant effect of time on ODI F = 97.91, p = 0.001.
Table 2. Comparison of Oswestry Disability Index (ODI) for each treatment group based on time (n=36)
Table 3 below describes between group result of PNF exercise, McKenzie and Control group in Oswestry Disability Index (ODI) in terms of Mean Difference (MD) and Confidence Interval (CI). There was significant difference of ODI score between the group (F= 6.19, p = 0.005).
Table 3. Overall mean difference of ODI among three treatment group based on treatment effect) (n=36)
Table 4 describe the comparison between PNF exercise with Control group, McKenzie method and Control group treatment on ODI in terms of Mean difference and p-value for every comparison group. The Multivariate test for ODI-treatment interaction result based on F-test showed the p < 0.005.
Table 4. Comparison of ODI among three treatment group based on time
DISCUSSION
The findings of the present study
showed that there was a good improvement in functional disability that was
assessed by using Oswestry Disability Index (ODI) in within group analysis.
Those three treatments showed significant result in reducing the ODI score
after treatments both after 2 weeks and after 4 weeks. This implied that all
the three treatments were successful in reducing the ODI score. In between
groups and time-treatment interaction, showed there was significant difference
result in increasing ODI score by PNF than control group treatment after 2
weeks of treatment, however, comparison between PNF and McKenzie showed no
significant difference so as between McKenzie and control group comparison.
After 4 weeks treatment, PNF showed more statistically significant difference
in reducing the ODI score than the McKenzie group and extremely significant
difference than the control group. Although, the McKenzie also showed
significant difference in reducing the ODI score than control group, it could
be implied that the PNF exercise was superior to the McKenzie and control group
31.
The result of this present study was
also supported with the findings of the study by Kumar, Zutshi and Narang, who
reported that PNF showed significant improvement in ODI score compared with
conventional exercise for LBP that consist of knee to chest, pelvic bridging,
pelvic rolling and alternate arm leg extension after 4 weeks. This study also
revealed that PNF showed better result in muscle endurance test, which can be
concluded the improvement in muscle endurance test can contribute in reducing
the ODI score result after the PNF exercise. Thus, prolonged sitting activity
which was one of the habits in the present study population contributed to
reduction in trunk muscle endurance 32.
Sawant and Ghodey studied on PNF
functional ability and trunk muscle endurance which confirmed that PNF has
shown significant improvement in trunk muscle endurance and functional ability
with ODI on chronic mechanical LBP patient. The study on the effectiveness of
PNF for LBP done by Franklin et al. reported that the PNF showed highly
significant difference to improve the ODI score compared with core stability
exercise. The PNF exercise in this previous study underwent 4 weeks session at
the same period with core stabilisation exercise 33.
Similar
study conducted by Dhaliwal et al. [36] regarding to PNF program versus core stabilisation exercise
for decreasing pain and improving function on patient with LBP, reported that
the PNF significantly decrease the ODI score among patient with LBP. Thus,
those previous studies strengthened the facts that PNF is better in
strengthening of the core muscle than the core stability exercise, with further
improvement in the functional ability outcomes of LBP. The results from
previous studies also implied that the PNF, compared with core stabilisation
exercise, were better in reducing the ODI score and supported the present study
result. Another study comparing the PNF with conventional strengthening
exercise, which consist of exercise for transversus abdominis muscle and
multifidus showed that PNF gave better improvement in ODI score than the
conventional exercise 34.
The
exercise period in their study was only for 3 weeks, which can be implied that
the PNF could be improving the ODI score even before 4 weeks. As McKenzie focusing more on postural correction and not on providing the core strength exercise, it can be
concluded that the PNF was more superior in reducing the ODI score with
improved trunk muscle endurance than McKenzie method.
This study had several limitations. Firstly, the sample size
was small, leading to reduced statistical power. Secondly, even though the
result revealed there are statistically significant, the difference score of
ODI did not meet the minimal clinically important. Future study is required to
meet minimal clinically important score of ODI. The McKenzie method was
followed the Treat your Own back booklet from McKenzie which not the proper
Mechanical Diagnosis and Treatment (MDT), however, the results showed the
McKenzie method have a good effect to subjects. Future study also needed to compare
the MDT with PNF properly.
Since this study was conducted to determine the
direct impact of the treatment, it could not be guaranteed for the treatment to
produce better effects if the follow-up sessions are extended, which the present study does not assess on the
long-term effects. This present study used a
quasi-experimental design, thus the development of study
design for future study is also suggested in improving the level of other studies.
The researchers recommended using PNF exercise for the physiotherapist
in order to get better outcome for non-specific LBP patient. Furthermore, as a prevention and self-management
for the patients which are engaged in a prolonged sitting, the physiotherapist can provide them with educational
exercise sheet and McKenzie method for home exercise program besides their
regular treatment with physiotherapist.
Ethical Clearance: Received approval letter from
the Research Ethics Committee, School of Health Sciences, KPJ Healthcare
University College with reference
number: KPJUC/RMC/ MPT/ EC/ 2017 /89 dated 02/08/2017.
Fund for the
study: Research
Management Center, Department of Physiotherapy, School of Health Sciences, KPJ
Healthcare University College, Malasia.
Conflict of Interest: All authors have no conflict of
interest to declare on conduct of this study.
CONCLUSION
This study
revealed that the three treatments made change on ODI score in each group
analysis. However, further comparison between PNF exercise and McKenzie method
showed that PNF exercise has more effect in improving the functional disability
score than McKenzie method on patient with Non-specific LBP.
Acknowledgement: We would like to thank the Research
Management Center, Department of Physiotherapy, School of Health Sciences, KPJ
Healthcare University College, for all the physiotherapists and all the facilitators.
Lastly, we extend our gratitude to all those who participated in this study.
REFERENCES
Taguchi,
T. (2003). Low back pain in young and
middle-aged people, Journal of Japan Medical Association; 46(10); 417–423.
Waongenngarm, P.,
Rajaratnam, B. S., & Janwantanakul, P. (2016). Internal Oblique and
Transversus Abdominis Muscle Fatigue Induced by Slumped Sitting Posture after 1
Hour of Sitting in Office Workers. Safety
and Health at Work; 7(1);
49-54.
Nordin, N. A., Devinder, A. S., & Kanglun,
L.(2014). Low Back Pain and Associated Risk Factors among Health Science
Undergraduates. Sains Malaysiana
43(3); 423-428.
Janwantanakul, P., Sihawong R.,
Sitthipornvorakul E., Paksaichol, A.(2015). A screening tool for non-specific
low back pain with disability in office worker : a 1 year prospective cohort
study. BMC Musculoskeletal Disorders;
16 : 298.
Mozafari, A., Vahedian, M., Mohebi, S., Najafi
M. (2015). Work-related Musculo-skeletal disorder in truck drivers and office
worker. Acta medica Iranica;
53: 7.
Koley S, Kaur J, Sandhu JS.(2010). Biological
risk indicators for non-specific low back pain in young adults of Amritsar,
Punjab, India. Journal of Life Sciences; 2: 43-48.
Koley S, Sharma L, Kaur S.(2010). Effects of
occupational exposure to whole body vibration in tractor drivers with low back
pain in Punjab. Anthropologist;
12: 183-187.
Patil, V.S., Master, M.F., Naik, R.V.(2016). A
cross-sectional observational study on the prevalence of mechanical low back
pain in physiotherapy students. National Journal of Intergrated Research
Medicine; 7(6): 9-12
Castellini, G.,
Gianola, S., Banfi, G., Bonovas, S., & Moja, L.(2016). Mechanical low back
pain: Secular trend and intervention topics of randomized controlled trials. Physiotherapy Canada; 68(1):
61-63.
Koes B,
W., van Tulder M., Lin, C., Macedo, L, G., McAuley J., Maher C. (2010). An
update overview of clinical guidelines for the management of non-specific low
back pain in primary care. European Spine Journal; 19; 2075-2094.
Gordon, R., Bloxham, S. (2016). A Sytematic review of the effects
of exercise and physical activity on non-specific cronic low back pain, Healtcare
journal; 4 : 22; 10.3390.
Scharrer M, Ebenbichler G, Peiber K, Crevenna,
Gruther W, Zorn C, Grimm- Steiger, Herceg M, Keilani M, Ammer K.(2012). A
systematic review on the effectiveness of medical training therapy for subacute
and chronic low back pain. European Journal Phyhsical Rehabilitation Medicine; 48: 361-70.
Westwater-Wood, S., Adam N., Kerry, R. (2010).
The use of proprioceptive neuromuscular facilitation in physio-therapy
practice. Physical Therapy Reviews;
15(1).
Lee YJ.(2009). The effects of the PNF Techniques
on lumbar stability and the functional activity in chronic low back pain
patients. Department of Physical Therapy Graduate School of Dongshin
University,; pp
1–60.
Kofotolis,
N., Kellis, E.(2006). Effect of two 4-week proprioceptive neuromuscular
facilitation programs on muscle endurance, flexibility, and functional outcomes
performance in women with chronic low back pain. Physical Therapy; 86 (7):
1001-1012.
Park, S. E., Wang, J.S.(2006).
Effect of joint mobilization KEOMT and PNF on a patient with CLBP and a lumbar
transitional vertebra : a case study, Journal of Physical Therapy Sciences,
2015; 27 : 1629-1632.
Lee, C.-W.,
Hwangbo, K., & Lee, I.-S.( 2014). The effects of combination patterns of
proprioceptive neuromuscular facilitation and ball exercise on pain and muscle
activity of chronic low back pain patients. Journal of Physical Therapy Science; 26(1): 93-6.
Kumar A., Zutshi K,. Narang N. (2011). Efficiacy
of Trunk Propioceptive Neuromuscular Facilitation Training on Chronic Low Back
Pain. International Journal of Sports Science and Engineering; 5 (3): 174-180
Johnson
GS., Johnson VS. (2002). The application of the principles and procedures of
PNF for the care of lumbar spinal disabilities. The journal of manual and manipulative
therapy; 10(2); 83-105
Clare H,
Adams R and Maher CG.(2004). A
systematic review of efficacy of McKenzie therapy for spinal pain. Australian Journal of Physiotherapy; 50;
209-216.
Garcia, A.N., Gondo, F.L.B., Costa, R.A.,
Cyrillo, F.N., Costa, L.O.P.(2011). Effects of two physical therapy
interventions in patients with chronic non-specific low back pain : feasibility
of a randomized controlled trial. Revista Brasileira Fisioterapia, Sao Carlos;
15(5): p.420-7
Young, K. J., Je,
C. W., & Hwa, S. T. (2015). Effect of proprioceptive neuromuscular
facilitation integration pattern and swiss ball training on pain and balance in
elderly patients with chronic back pain. Journal
of Physical Therapy Science; 27(10):
3237–40.
Casser HR, Seddigh S, Rauschmann M. (2016).
Acute lumbar back pain-investigation, differential diagnosis and treatment.
Deutsches Ärzteblatt International; 113: 223 34.
Issa LF,. Seleem NA,. Bakheit AM,. Baky AA,.
Alotaibi AF.(2016). Low back pain among undergraduate student at Taif University-
Saudi Arabia. International Journal of Public Health and Epidemiology ; 5(6), pp 275-284.
Maher, C., Underwood, M., Butchbindee, R.(2017).
Non-specific low back pain. Seminar, Lancet; 389: 736-47.
Sihawong, R.,
Janwantanakul, P., & Jiamjarasrangsi, W.(2014). A prospective,
cluster-randomized controlled trial of exercise program to prevent low back
pain in office workers. European Spine
Journal; 23(4); 786–793.
Hasanpour-Dehkordi, A., Dehghani, A., Solati, K.
(2017). A comparison of the effects of Pilates and McKenzie training on pain
and general health in men with chronic low back pain: A randomized trial.
Indian Journal of Palliative Care; 23: 36-40.
Longo G, Loppini M, Denaro L, Maffulli N, Denaro
V. (2010). Rating scales for low back pain. British Medical Bulletin 98;
81-144.
Jadeja,
T., Vyas, N., Sheth, M. (2015). To Study the effect of proprioceptive
neuromuscular facilitation on back muscle strength, pain, and quality of life
in subjects with chronic low back pain-an experimental study. International
Journal of Physiotherapy; 2(5); 778 -785.
Aziz,
S., Ilyas, S., Imran S., Yamin F., Zakir A., Rehman A., Adnan S., Khanzada S.
(2016). Effectivenes of Mc. Kenzie Exercise in Reducing Neck and Back Pain
Among Madrassa Student. International Journal Physiotherapy; 3 (1): 78-85.
Paatelma,
M., Kiplikoski, S., Simonen, R., Heinonen, A., Alen, M., Videman, T. (2008).
Orthopedic manual therapy, McKenzie method or advice only for low back pain in
working adults : A Randomised controlled trial with one year follow-up. Journal
of Rehabilitation Medicine; 40; 858-863.
Sawant,
R., Ghodey S. (2017). Added effect of proprioceptive neuromuscular facilitation
on functional ability and trunk endurance in chronic low back pain patients. International Journal
of Allied Medical Sciences and Clinical Research; 5(2): 480-486.
Franklin,
C.V.J., Kalirathinam, D., Palekar T., Nathani N. (2013). Effectiveness of PNF
Training for Cronic Low Back Pain. IOSR
Journal of Nursing and Health Science (IOSR-JNHS); 2: 41-52.
George, A, J., Kumar D, K, U., Nikhil N.P. (2013). Effectiveness of trunk proprioceptive neuromuscular facilitation training in mechanical low
back pain. International Journal of Current Research; 5(7); pp.1965-1968.
Citation:
Lucky Anggiat, Wan Hazmy Che Hon, et al (2020).The changes of functional disability in
non-specific low back pain among university population after proprioceptive
neuromuscular facilitation and mckenzie method , International
Journal of
Medical and Exercise Science, 6 (1): 656-667.
Dhanalakshmi.M.R1 , Prashanth V Mangalvedhe2 , Jibi Paul3
Authors:
1 B.P.T. Graduate, JSS College of Physiotherapy, JSS Hospital Campus, Mysuru, Karnataka,India. 3 Professor,Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India.
Corresponding Author:
2 Lecturer, JSS College of Physiotherapy, JSS Hospital Campus, Mysuru, Karnataka,India. Mail id: dhanuphysio7@gmail.com
ABSTRACT
Introduction: Moberg pickup test (MPUT) is a standardized test for hand dexterity developed by Erik Moberg, in 1958. This test also assesses cognition, stereognosis, and comprehension. Aim of the study was to find the normative values for the Moberg pickup test and to find the impact of gender and handedness on hand dexterity among carpel tunnel syndrome patients.
Method: This was a Cross-sectional study, conducted at JSS College of physiotherapy, Mysuru, Karnataka for a duration of 2 months. This study was done on a population of 171 typical young adults comprising of 37 males and 134 females with an age group between 17 and 25 years. Test objects were placed on the table on the same side of right and left hands being tested with eyes open and closed, whereas the container was placed on the opposite side of the hand being tested. Three trials were done and the best out of the three was taken for analysis to obtain the normative values for Mobergpickup test.
Result: The results show that the hand dexterity of the subjects was significantly good. Eyes open and close on dominant hand and Non dominant hand with mean values of 7.735, 12.806 and 9.206, 14.327 respectively.
Conclusion: Females performed the test faster than males, and task performance with the dominant hand was faster than the non-dominant hand.