S. M. Divya Mary1, S. Bhargavy2
Author:
2BPT Internee, Faculty of physiotherapy, Dr. MGR. Educational and research institute University, Velappanchavadi, Chennai, Tamilnadu, India
Corresponding Author:
1Assistant professor, Faculty of physiotherapy, Dr.MGR Educational and research institute University, Velappanchavadi, Chennai, Tamilnadu, India, Email id: divyamary.physio@drmgrdu.ac.in
ABSTRACT
| Background of the study: Forward head posture is the anterior positioning of the “cervical spine”. This posture is sometimes called “text neck” or “reading neck”. Mostly the targeted group is younger & older adults. The main reason is our sedentary lifestyle-sitting at computers for hours, playing games continuously, driving for long distance time. Objective of the study is to find out the effectiveness of conventional exercise over fencing exercise to correct the forward head posture in individuals with abnormal head posture. Methodology: this study is the experimental design comparative pre & post type.30 subjects will be divided into two groups. Group a will be given conventional exercise & group b will receive fencing exercise. Ruler measurement & Cranio vertebral angle will be used as outcome measures. Result: on comparing pre test & post test within group a% group b on ruler measurement & cranio-vertebral angle shows highly significant difference in mean values p ≤ 0.001. Conclusion: This study shows that there was improvement in forward head posture in both groups. however conventional exercise(Group-A) showed more improvement than fencing exercise (Group-B) & to correct forward head posture & brings them back to normal posture. Keywords: Fencing exercise; Ruler measurement; Forward head posture; Cranio-vertebral angle. |
| Received on 29th January 2021, Revised on 14th February 2021, Accepted on 26th February 2021; DOI:10.36678/IJMAES.2021.V07I01.006 |
INTRODUCTION
Forward head posture is one of the most commonly recognized types of poor head posture in the sagittal plane. Forward head posture has been defined as any alignment in which external auditory meatus is positioned anterior to the plumb line through the shoulder joint1, 2.
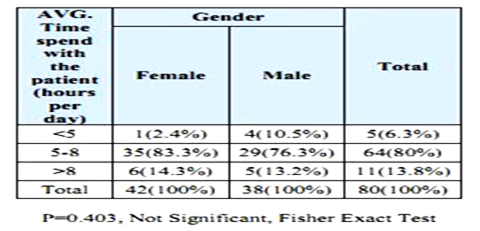
Mostly, the targeted group is younger and older adults. Totally,100 peoples are affected in the age group between 20-70 years old. The prevalence of anterior head translation in neck pain patients was found to be 37%, out of which 58% were female and 42% were male number. A review of different observational studies of neck pain around the world showed that its 1-year prevalence ranged from 16.5 to 75.1% for the entire adult population which aged from 17 to 70 years3, 4.
Data show that the people affected by “Forward Head Posture” in their fifties accounting for more than 23% of the total followed by those in their forties, thirties, and seniors over sixty. It has become more prevalent in modern times as the COG shifts in the body posture. For, compensation the upper body drifts backward and shoulder slump forward by placing head anterior to the trunk5,6.
While sitting, forward head inclination involves a combination of lower cervical flexion, upper cervical extension, which reduces the average lengths of muscle fibers, contributing to extensor torque around the upper cervical joint. In addition to this, abnormal posture causes musculoskeletal abnormalities such as decreased scapular upward rotations well as greater internal rotation and anterior tilting, which may be the difficulties in maintaining upright posture .Conventional exercise aims at improving function of muscle, which counteracts the forces of gravity in order to maintain the head and neck in upright position7-9.
Fencing response designation arises from stimulating the “asymmetric tonic neck reflex” in infants. like reflex, a positive fencing response resembles the en grade position that initiates fencing with extension of one arm and flexion of other. This study aims at the effectiveness of fencing exercise with conventional exercise in forward head posture in individuals with abnormal head posture10.
Biomechanics: In forward head posture, the head shifts anteriorly from the line of gravity, the scapulae may rotate medially, a thoracic kyphosis may develop and overall vertebral height may be shortened. The features are as follows: there is an obliteration of the cervical lordosis and a compensatory tilting back of the head at the atlanto-occipital joint. In the posterior cervical muscles there is stretching and weakness of semispinalis cervicis and overaction with ultimate shortening of semispinalis capitis 11.
Pathomechanics: Instabilities lead to more serious pathology eventually, such as desiccation(thinning disc),cervical spine spondylosis, disc pathology facet ¢ral cord stenosis, thoracic spine compression fractures. People with uncorrected FHP posture potentially suffer chronic or unpleasant conditions, such as pinched nerves 12.
Upper Cross Syndrome– Tightness of the upper trapeziums and elevator scapula on the dorsal side crosses with tightness of pectorals major and minor. Weakness of the deep cervical flexors ventrally crosses with weakness of middle and lower trapeziums’ his pattern of imbalance creates joint dysfunction, particularly at the Atlanta occipital joint,C4-C5 segment, cervico-thoracic joint, gleno-humeral joint&T4-T5 segment 13.
METHODOLOGY
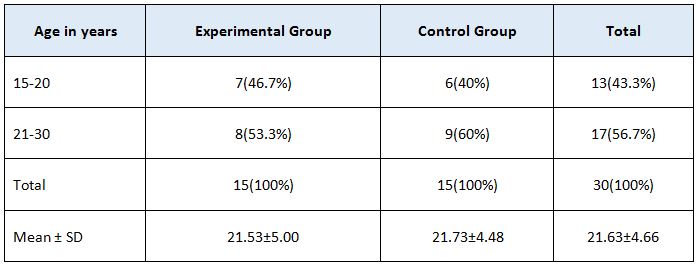
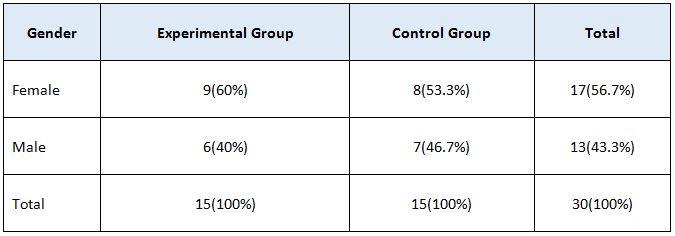
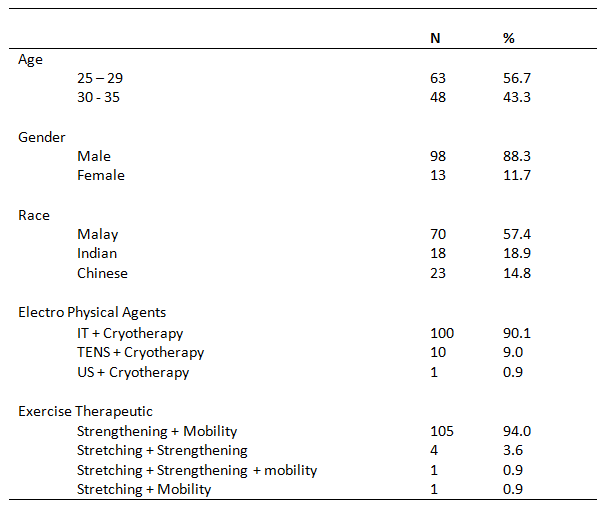
This study is the experimental design comparative pre & post type. 30 subjects were recruited from dr.mgr educational & research institute (A.C.S medical college and hospital) – physiotherapy – opd, Chennai. Subjects were selected by simple random sampling method. Study duration was 5 days in a week for 4 weeks. Inclusion criteria were both male and female subjects between age group 18-35 years old, who have 4-12cm in “ruler measurement” & “cranio-vertebral angle” less than 50 degree. Exclusion criteria were age group between below 18 & above 35 years were excluded. Subjects with systemic illness, no recent injuries & neurological complications were excluded. Ruler measurement & cranio-vertebral angle will be used as outcome measures. Mobile application (on protractor), adhesive skin markers, millimeter ruler were the materials used.
Procedure: 30 volunteers fulfilling the inclusion criteria were included in this study. The forward head posture is identified by measuring the spinal column alignment.
Measurement of Forward Head Posture Ruler Measurement: This method is done with ruler (scale),ask the patient to lean on the wall in relaxed position & measure the length between the wall and head.
Cranio-vertebral Angle
This method was measured using smartphone application-“ON PROTRACTOR”. This application allows to take picture and draw angle by touching the screen at the reference points on the markers. Two markers were Used: One placed on the tragus of the ear and second placed on C7 vertebra were measured and photographs taken.
Position of patient: The patient is made to stand against the wall. 30 Volunteers Were Divided Into 2 Groups,
Group A- In this group, 15 volunteers performed forward head posture correction program ,the exercise were done 5 days in a week for 4 weeks, which consists of 2 sets with 15 repetitions.
Chin tucks, Isometric neck exercise, Shoulder retraction/ Protraction, Shoulder shrugging/ Dropping, Then followed by posture correction techniques. The patient should stand in front of the mirror and correct the abnormal posture, Chin tucked position. Shoulder retracted position. The patient should correct their abnormal posture for every one hour.
Group B- In this group, 15 volunteers performed fencing exercise, the exercise were done 5 days in week for 4 weeks, which consists of 2 sets with 15 repetitions. The patient is given a wand to perform fencing movements. All the fencing movements are done under the instruction and supervision of physiotherapist only.
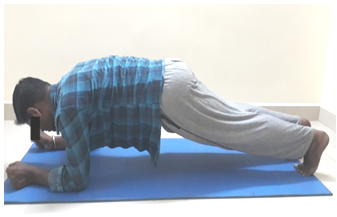
Lunge pose:
Lead Side:
Upper body:
Neck position- Chin tucked. Shoulder- Retraction., Arm- Fully extended at 90 degree. Trunk- Neutral position. Wrist- Mid prone.
Other Side: Upper body:
Neck position- Chin tucked. Shoulder- Retraction. Trunk- Neutral position.
Arm- Fully extended at 90 degree. Wrist- Supination.
Lower body: Lunge position.
Parry pose:
Lead Side
Upper body:
Neck position- Chin tucked.
Shoulder- Shoulder abducted at 160 degree & internally rotated. Trunk- Neutral position.
Wrist- Pronation.
Lower body: Knee semi -flexed
Other Side
Upper body:
Neck position- Chin tucked. Shoulder- Adduction. Elbow- Flexion. Wrist- Supination.
Trunk- Neutral position.
Lower body:
Leg abducted.
Riposte pose:
Lead Side; Upper body:
Neck position- chin tucked. Shoulder- Adduction. Elbow- Slightly flexed. Wrist- Supination.
Trunk- Neutral position
Other Side: Upper body:
Neck position- Chin tucked. Shoulder- Abduction 90 degree. Elbow- Flexed.
Wrist- Flexion.
Lower body: Mid squat position.
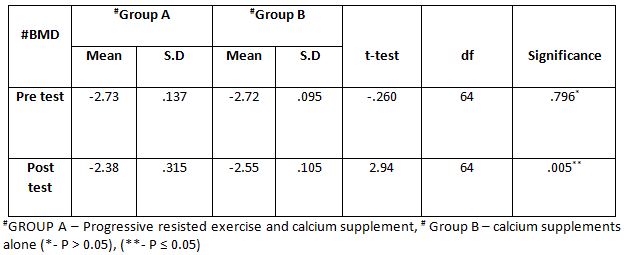
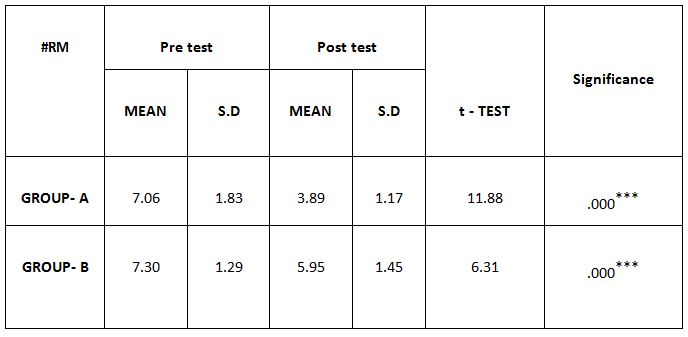
Group – B In Pre And Post Test
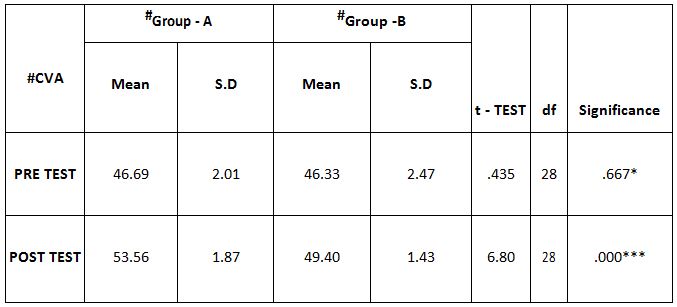
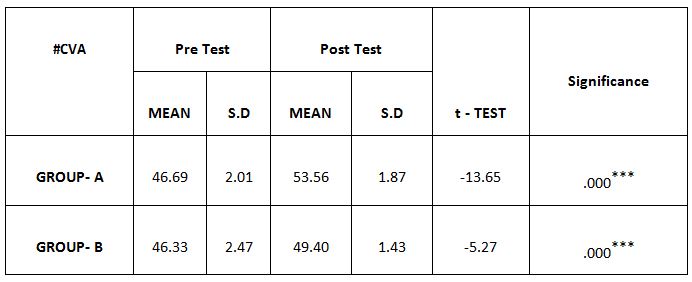
Comparison of Cranio-vertebral Angle Between Group – A And Group – B In Pre And Post Test
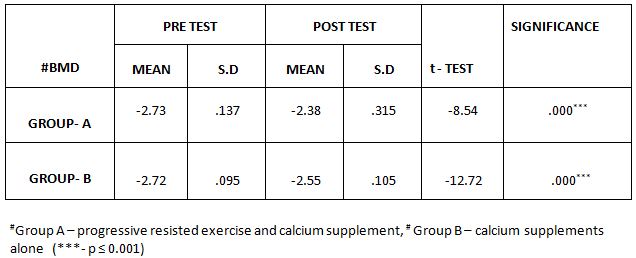
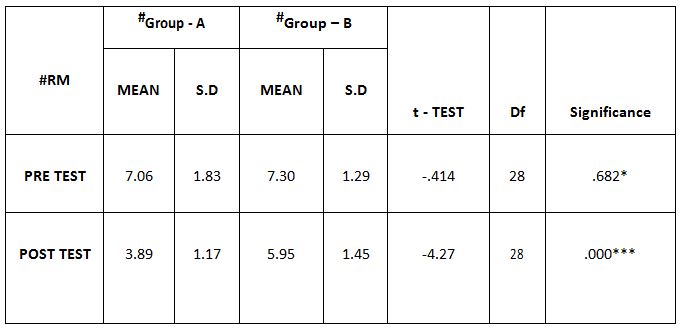
Comparison Of Ruler Measurement Score Within Group – A & Group – B Between Pre & Post Test Value
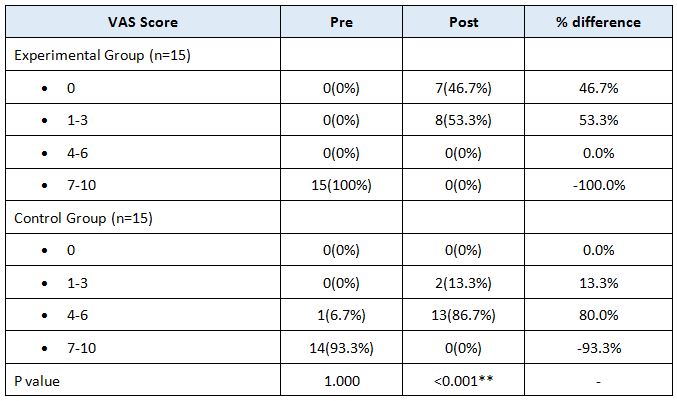
RESULT
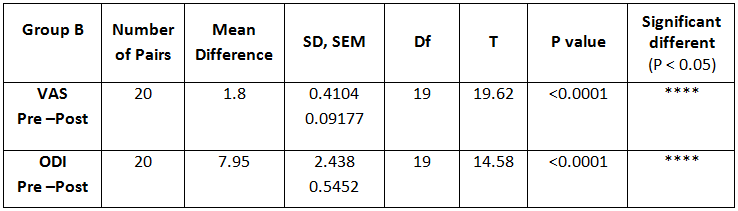
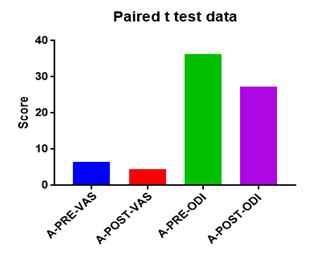
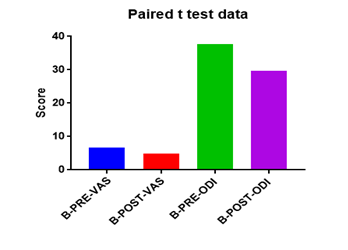
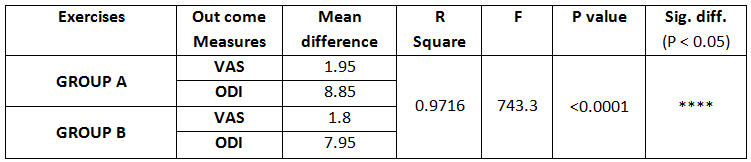
On comparing the pre and post test values within the experimental group, Group A & Group B on Ruler Measurement & Cranio-vertebral Angle shows highly significant difference in Mean values where p value is P ≤ 0.001.Group A – Conventional Exerciseshows statistically significant improvement then Group B – Fencing Exercise.
DISCUSSION
In this world, almost everywhere including schools, colleges, offices and even in homes computers and Smartphone’s are commonly used today. Forward head posture is the misalignment of head on trunk, leads to increased lordotic curve of the cervical spine and accompanied by increased kyphosis of thoracic spine. Forward head posture leads to body mechanical deformation anterior to centerline of gravity, this reduces muscle strength of neck stabilization muscles, reduces
the activity of the stabilizer muscles of the scapulae and changes body mechanics of the scapulae. A sample of 30 subjects were selected and assessed then recorded the values. After, giving treatment the values are analyzed for significant differences. Cranio-vertebral angle is a good indicator for measuring forward head posture. The cranio-vertebral angle was measured using, ”On Protractor App” which is available on goggle play store 13,14.
A study on validity and reliability of “ON PROTRACTOR” smartphone application for measurement of cranio-vertebral and cranio-horizontal angle. In this study, the mean cranio-vertebral angle in non forward head posture is 50 degrees. The result of the study showed a effectiveness between conventional exercise and fencing exercise. This study proved that there was an increased effect in conventional exercise than fencing exercise after correction forward head posture 15.
The conventional exercise treatment showed improved ability in holding an upright posture of cervical spine and retraining these muscles was shown to reduce the neck symptoms and improved ability in maintaining an upright posture of cervical spine. The result showed that forward head posture significantly, reduced in the treatment groups after 4 weeks exercises, this improvement was also maintained after 1 month follow-up. Moreover, when compared with group A and group B, the forward head posture was reduced in group A (conventional exercise), which is effective 16.
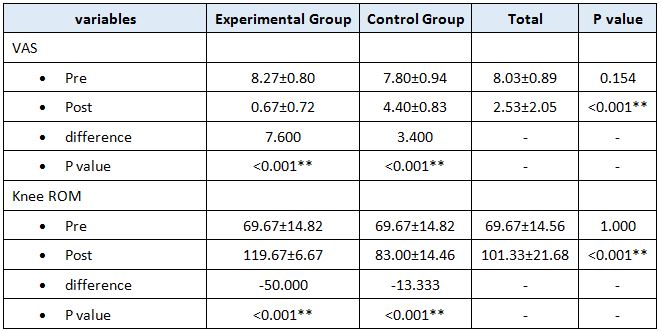
In this study 15 subjects were included for conventional exercise (Group-A). It supported on effect in forward head posture which reveals significant difference in mean values. In pre-test 7.09 in ruler measurement and 46.69 in cranio-vertebral angle. In post-test 3.89 in ruler measurement and 53.56 in cranio-vertebral angle. Another 15 subjects included in fencing exercise (Group-B) .The fencing exercise also showed effect in forward head posture correction. The study reported significant differences in mean values. In pretest 7.30 in ruler measurement and 46.33 in cranio-vertebral angle. In post-test 5.95 in ruler measurement and 49.40 in cranio-vertebral angle.
Fencing is a great cardiovascular exercise, using several sets of muscles at a demanding intensity level over an extended period of time. The physical benefits of fencing include increased agility, balance, flexibility, Strength and cardiovascular endurance. While fencing is a whole exercise, it exercises the arms, thighs, buttocks hardest of all .You also benefit from fencing by gaining greater mental agility. Key muscles used for fencing exercise are, Upper body-Back muscles and Trapezius, Lower body-quadriceps, hip flexors, Gluteus, Hamstrings, Calves and core 17.
The purpose of this present study is to focus the effects of conventional exercise and fencing exercise in correction of forward head posture in younger adults. The conventional exercise is very effective because it demands deep muscles to work and strengthen muscles. Conventional exercise are very easy to learn and 15 subjects were practiced at home without the supervision of physiotherapist.These,15 subjects set remainder in their mobile phones to correct their posture and to do exercise regularly. They, also see mirror to correct their head posture which act as visual feedback. Because, of active participation of subjects in group A showed good and effective results.
In fencing exercise, especially in upper body few sets of muscles are used like trapezius, back muscles, biceps, triceps which is used for holding a wand and to keep shoulders in retracted position. The 15 subjects in group also actively participated for fencing exercise. To prevent unwanted consequences fencing exercise was done under the supervision of physiotherapist. Fencing exercise also showed values nearing to conventional exercise in 4 weeks duration. The pre-test and post-test of ruler measurement and cranio-vertebral angle in experimental groups is statistically significant at p<0.01 i.e. there is improvement in correction of forward head posture after treatment.
Ethical Clearance: Ethical clearance has obtained from Faculty of Physiotherapy, DR.MGR. Educational and Research Institute, Chennai to conduct this study with reference number: A-12/ PHSIO/IRB/2018-19dated 08/01/2019.
Conflict of interest: The author reported no conflict of interest to do this study
Funding: The researchers had self financial support to conduct this research.
CONCLUSION
By the obtained result from this experimental study , it is concluded that there was improvement in forward head posture in both groups. However, conventional exercise(Group-A) showed more significant improvement than fencing exercise (Group-B) and corrects forward head posture and brings them back to normal posture.
REFERENCES
- Levangie P,Norkin C. (2012). Joint structure and function, 5th edition. New Delhi:Jaypee Brothers Medical publishers (P) Ltd; .P 502.
- Jung Won Kwon, Phd, PT, et ai. (2015). Changes in upper-extremity muscle activities due to head position in subjects with a forward head posture and rounded shoulders. J Phys Ther Sci; 27(6): 1739-1742.
- Gupta BD,Aggarwal S, Gupta B, Gupta M, Gupta N. (2013). Effect of Deep Cervical Flexor Training vs. Conventional Isometric Training on Forward Head Posture, Pain, Neck Disability Index In Dentists Suffering from Chronic Neck Pain. J Clin Diagn Res. 7(10):2261-4.
- Deborah Falla, Gwendolen Jull, et al.(2007). Effect of neck exercise on sitting posture in patients with chronic neck pain.Physical therapy 87 (4), 408-417.
- John S.Y. Chanaalan C.N. et al. (2011). Fencing expertise and physical fitness enhance action inhibition. Psychology of Sport and Exercise Volume 12, Issue 5, September Pages 509-514.
- Johnson, Gillian M., Dip Phty, Msc Spine. (1998). The Correlation between Surface Measurement of Head and Neck Posture and the Anatomic Position of the Upper Cervical Vertebrae. April 15, – Volume 23 – Issue 8 – p 921-927.
- Bhuvan Deep Gupta, Shagun Aggarwal, and Neha Gupta. (2013). Effect of Deep Cervical Flexor Training vs. Conventional Isometric Training on Forward Head Posture, Pain, Neck Disability Index In Dentists Suffering from Chronic Neck Pain. J Clin Diagn Res.; 7(10): 2261-2264.
- Alireza Rabieezadeh, et al. (2016). The relationship of height, weight and body mass index with curvature of spine kyphosis and lordosis in 12-15 year old male adolescents of Tehran. Turkish Journal of Sport and Exercise.6Year: -Volume: 18 – Issue: 3 – Pages: 42-46 .
- Kyeong-Jin Lee, et al.(2015).The effect of forward head posture on muscle activity during neck protraction and retraction. J. Phys. Ther. Sci. 27: 977-979.
- Jae Woong Han (2016). Biomechanical Analysis of Chin Tuck Exercise with a Subject-Specific Neck Model for the Forward Headed International Journal Of Precision Engineering And Manufacturing Vol. 19, No. 4, pp. 587-592.
- Jeong-Gon Na, et al. (2018). Effects of Exercise Type on Neck Disability, Pain, and Postural Changes in Subjects with Forward Head Posture: Systematic Review and Meta-Analysis. J Korean Soc Phys Med;13(3): 121-132.
- Lindsay M. Bottoms, et al (2011). Physiological responses and energy expenditure to stimulated epee fencing in elite female fencers. Serbian Journal of Sports Sciences, 5(1): 17-20.
- Jonathan D. Wiles, et al. (2018) The safety of isometric exercise Rethinking the exercise prescription paradigm for those with Stage 1 hypertension. Wiles et al. Medicine 97:10.
- Minou Khakhali-Zavieh, et al. (2003) .The validity and reliability of measurement of thoracic kyphosis using flexible ruler in postural hyper kyphotic patients. Archives of Rehabilitation 4 (3), 18-23.
- Jay Smith, Brian R Kotajarvi, Denny J Padgett, Joe J Eischen. (2002). Effect of scapular protraction and retraction on isometric shoulder elevation strength. Archives of physical medicine and rehabilitation 83 (3), 367-370.
- Jerrold S Petrofsky, Richard L Burse, AR Lind. (1975). Comparison of physiological responses of women and men to isometric exercise. Journal of Applied Physiology 38 (5), 863-868.
- Karthikeyan selvaganapathy, Roshini Rajappan, Thom hung dee. (2017). The effect of smartphone addiction on craniovertebral angle and depression status amount university students. International journal of integrative medical sciences, vol4(5): 537-42.
| Citation: S. M. Divya Mary, S. Bhargavy(2021). Effect of movement therapy in individuals with abnormal head posture , ijmaes; 7 (1); 960-968. |